
Abstract
Introduction
Laser lipolysis is a rapidly growing noninvasive body-contouring treatment in Asians. There is increasing demand for leg contouring, especially in areas where unwanted fat deposits are prominent despite diet and exercise. Medial fat knees are one of the esthetic concerns of women today and can be a challenging problem in terms of treatment. There are few noninvasive options to remove fat from these areas. This study aims to evaluate the safety and efficacy of a 1060-nm diode laser for medial knee fat reduction.
Methods
Nineteen subjects with localized unwanted fat on the medial knees were enrolled into this study. All of them were treated with a single session of 1060-nm diode laser at a power setting of 1.0–1.4 W/cm2, depending on patient tolerance. Body weight, knee circumference at 3 cm above the medial epicondyle of the femur, and knee fat thickness measured by ultrasonography were recorded at baseline and 1, 3, and 6 months after treatment. Clinical photographs and ultrasound images were taken before and after treatment. Side effects were documented during follow-up visits. Subjects answered a satisfaction questionnaire at the completion of the study.
Results
All subjects were female, with mean age of 32.3 ± 5.3 years and body weight of 59.8 ± 11.6 kg. The average power setting was 1.3 ± 0.1 W/cm2 with pain score of 6.1 ± 1.0. Significant reduction in knee circumferences (p < 0.001) at 1-, 3-, and 6-month follow-up visits compared with baseline, and knee fat thickness measured by ultrasound in both axial and sagittal plane at 1 and 6 months after treatment (p = 0.036 and p < 0.001, respectively) were recorded. Side effects were mild and transient, including mild erythema and tenderness.
Conclusion
The 1060-nm diode laser is effective and safe for knee circumference and medial knee fat layer thickness reduction.
Trial registration
ClinicalTrials.gov identifier, TCTR20220219002. Retrospectively registered on February 19, 2022.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study? |
The 1060-nm diode laser can be used for noninvasive laser lipolysis to remove unwanted fat on medial knees. |
The study aims to evaluate the safety and efficacy of a 1060-nm diode laser for medial knee fat reduction. |
What was learned from the study? |
The results showed a significant reduction in knee circumferences and knee fat thickness measured by ultrasound. |
The 1060-nm diode laser is effective and safe for knee circumference and medial knee fat layer thickness reduction. |
Introduction
Many women share concerns about the appearance of their knees. Weight gain, sagging skin related to aging or recent weight loss, and decreased muscle tone from inactivity or injury can all affect the appearance of the knee area. These changes are frustrating to women and can affect them emotionally and socially [1]. According to Chamosa, the medial knee zone has the greatest deposits of adipose tissue [1, 2]. Excessive fat on knees can also be genetically predisposed and is resistant to diet and regular exercise [1].
Liposuction and lipectomy are some of the surgical procedures carried out by medical professionals to address unwanted fat in this area [1, 3]. However, these can be traumatic to patients and have slower recovery time, and can have unpredictable results and serious adverse events [1, 3]. According to literature, lipectomy on knee area is prone to persistent edema, hyperpigmentation, prolonged pain, irregularities, and cutaneous necrosis [1].
With the advancement of technology, many noninvasive treatment modalities have been developed to address fat reduction in several areas of the body, such as monopolar and bipolar radiofrequency (RF) [4], cryolipolysis [5,6,7], high-intensity focused ultrasound (HIFU) [8, 9], and lasers [1, 3, 10,11,12,13]. These procedures have quicker postoperative recovery and better patient safety profiles [1, 3,4,5,6,7,8,9,10,11,12,13].
The 1060-nm diode laser had been proven to cause fat reduction in several studies by clinical and histological assessments [10,11,12,13]. Because of its longer wavelength, it produces hyperthermia within the range of 42–47 °C, which can reach the subcutaneous tissue, resulting in adipocyte apoptosis, which subsequently stimulates inflammatory response [10]. The inflammatory response signals the removal of disrupted adipocytes and cellular debris by attracting more macrophages and removing them through phagocytosis. Its safety in patients with skin of color was evident in previous studies [10, 12, 13].
Decorato and colleagues demonstrated the optimal duration of 1060-nm diode laser treatment, which is 20–25 min to cause significant adipocyte injury. When used for longer than 25 min, it can create palpable nodules in the subcutaneous fat [11, 13]. Katz and colleagues demonstrated significant fat reduction in the flanks at 12 weeks post-treatment based on calculations from ultrasound images [10]. Similarly, significant fat layer thickness reduction in the abdomen was documented from the study initiated by Bass et al. [11]. So far, no clinical studies have been carried out on the use of 1060-nm diode laser for knee contouring. The purpose of this study is thus to evaluate the safety and efficacy of a 1060-nm diode laser for medial knee fat reduction.
Methods
A prospective study was carried out, enrolling 19 healthy female subjects aged from 26 to 43 years and presenting with body weight of 45–87 kg. Demographic data, clinical history, and physical examination of medial knees at 3 cm above the medial epicondyle of the femur of each subject were taken by the investigators.
Subjects with the following conditions were excluded from the study: pregnant or lactating women and those with previous history of liposuction or surgical procedures, previous treatment of botulinum injections and laser procedures, or immunosuppressive disorders such as human immunodeficiency virus (HIV) infections and malignancies, those taking immunosuppressant drugs, with previous history of herpes virus infection, underlying psychological conditions, history of hypertrophic scar or keloid formation, history of any skin infections, and skin hypersensitivity or photosensitivity reaction.
The investigators evaluated each subject’s unwanted localized fat on their medial knees. The area to be treated was outlined while the subject was in upright position. The treated area was marked with a template by investigator. Each subject was treated with a single session of 1060-nm diode laser (Sculpsure, Cynosure, Westford, MA) on their medial knees in straight-leg sitting position. One applicator was placed at each medial knee along the contour of treated area. The frame and strap were placed at each side of medial knee to ensure constant distance aligned with the template mark. The power settings used were 1.0–1.4 W/cm2, depending on the subject’s tolerance. The exposure time in all subjects was 25 min for each side of the medial knee [10, 11]. After treatment, subjects were asked to rate their pain using a 10-point scale (0 = none to 10 = worst).
At 1, 3 and 6 months posttreatment, subjects were asked to return for follow-up visits. During these visits, clinical photographs and ultrasound images were taken. Knee circumferences of the subjects in upright position were measured. Fat thickness in the axial and sagittal plane was also measured using ultrasound images. The primary endpoint of this study was to demonstrate a statistically significant reduction in knee circumference and fat layer thickness at 1, 3, and 6 months posttreatment compared with baseline. Knee circumference was measured in upright position, while fat thickness was measured in supine position using ultrasound imaging device (IU 22 xMATRIX US system, Philips Healthcare, Eindhoven, the Netherlands). Additionally, weight measurements in kilograms were also documented at each visit.
The secondary endpoint of the study was subject satisfaction of 75% or greater after treatment completion. All subjects answered the percentage improvement scale survey at each follow-up visit. Any serious side effects such as hypopigmentation, hyperpigmentation, scarring, fat dystrophy, infection, and paradoxical adipose hyperplasia were also assessed.
Descriptive analysis was used for the demographic data. The data were analyzed using paired t-test (normality) and repeated-measure analysis of variance (ANOVA) for parametric distribution. The statistical analysis was performed using IBM SPSS statistical software for Windows, version 24.0 (IBM Corp., Armonk, NY, USA), with p value < 0.05 indicating statistical significance.
This study was approved by the ethics committee of the Siriraj Institutional Review Board (si 369/2018) and Ethical Committee on Research involving human subjects and conformed to the guidelines of the Declaration of Helsinki of 1964 and its later amendments. Written informed consent was obtained from all subjects prior to their enrollment in the study.
Results
All 19 female subjects completed the study. The demographic data are presented in Table 1. The average age and body weight of all subjects was 32.3 ± 5.3 years and 59.8 ± 11.6 kg, respectively. They received a single treatment session of 1060-nm diode laser with average power setting of 1.3 ± 0.1 W/cm2 (range 1.0–1.4 W/cm2) (Table 1). Body weight changes of subjects at post-treatment follow-ups did not show statistically significant difference (p = 1.000) (Table 2).
The average knee circumference at baseline was 44.0 ± 4.5 cm. Data showed significant reduction of average knee circumference at 1 month (42.7 ± 4.2 cm), 3 months (41.9 ± 4.8 cm), and 6 months (41.3 ± 4.4 cm) compared with baseline (p < 0.0001) (Table 3). There was continuous decrease of circumference at each follow-up period.
The average fat layer thickness at baseline in axial and sagittal plane was 2.4 ± 0.8 cm and 2.5 ± 0.8 cm, respectively (Table 4). Fat thickness of 2.0 ± 1.1 cm in axial plane and fat thickness of 2.0 ± 0.9 cm in sagittal plane both evaluated by ultrasound showed a significant reduction as early as 1 month after treatment compared with baseline (p = 0.036, p = 0.001, respectively) (Table 4). Further decrease of fat thickness at 6 months after treatment in axial plane (1.5 ± 0.8 cm) and sagittal plane (1.6 ± 0.9 cm) was noted. The results were statistically significant (p < 0.001) (Table 4).
Based on the dynamic subgroup analysis, non-weight-gainers responded better to treatment (Tables 3, 4). The average knee circumference of non-weight-gainers was reduced significantly at 1, 3, and 6 months after a single treatment (p < 0.001, p = 0.005, and p < 0.001, respectively). The fat thickness of the non-weight-gainer group showed significant reduction at 6 months after treatment in axial plane (p < 0.001) and at 1 and 6 months in sagittal plane (p = 0.026 and p < 0.001, respectively).
On the other hand, the average knee circumference of weight-gainers showed significant reduction at 3 and 6 months only compared with baseline (p = 0.002 and p = 0.028, respectively) (Table 3). The fat thickness of the weight-gainer group showed significant reduction at 6 months after treatment, in both axial and sagittal plane (p = 0.006 and p = 0.003, respectively) (Table 4).
The results showed that 17.7% of subjects at 3 months and 47.1% of subjects at 6 months after treatment rated greater than 75% improvement and were satisfied with treatment outcome (Fig. 1). Clinical photographs and ultrasound images of representative subjects are shown in Figs. 2 and 3, each showing improvement in contour at 1, 3, and 6 months after the treatment.

Improvement scale evaluated by patients

Representative images of right medial knee of patient (case 1) after single session of 1060-nm diode laser

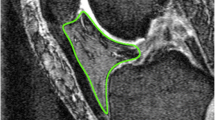
Representative ultrasound images of patient after single session of 1060-diode laser; S skin, SF subcutaneous fat, M muscle
The average pain score recorded was 6.1 ± 1.0 (Table 1). All subjects reported mild erythema and mild tenderness immediately after treatment. The side effects were transient. No serious side effects including hypopigmentation, hyperpigmentation, scarring, fat dystrophy, infection, and paradoxical adipose hyperplasia were found throughout the study.
Discussion
The advent of new technology such as noninvasive body-contouring devices has changed the business of surgical treatments and provided new options for addressing fat reduction. Lipolysis devices such as radiofrequency [4], cryolipolysis [5,6,7], ultrasound [8, 9], and lasers [1, 3, 10,11,12,13] are now being used worldwide as alternative procedures to remove fat in unwanted areas with a better safety profile compared with liposuction and other surgical procedures [1,2,3,4,5,6,7,8,9,10,11,12,13]. Each device has its own mechanism and efficacy profile [4,5,6,7,8,9,10,11,12].
A previous cryolipolysis study of 20 females with localized subcutaneous fat on arms or inner thighs showed significant circumference reduction at 3- and 6-month follow-up visits [5]. The efficacy was comparable to the present study, which also demonstrated reduction at 3 and 6 months post-treatment. Cryolipolysis works by inducing adipocyte apoptosis and inflammatory response using cold temperatures without damaging surrounding areas [5,6,7], while laser lipolysis generates controlled hyperthermia using a specific wavelength and optimal power in the subcutaneous layer and causes photothermal reaction that destroys adipocytes and stimulates inflammatory response [10, 13]. In the study by Decorato et al., hyperthermic laser lipolysis was comparable to cryolipolysis in average fat reduction at 3 and 6 months after treatment [13].
Previously conducted studies of 1060-nm diode laser showed significant reduction of localized subcutaneous fat on flanks [10] and abdomen [11]. The previous pilot study on the flanks demonstrated significant average fat reduction based on ultrasound images [10]. At 12 weeks after treatment, 96% (41/43) of subjects rated that they were satisfied with the treatment outcome [10]. Using the same device, Bass et al. showed a mean reduction in fat layer thickness of the abdomen from baseline at both 6 and 12 weeks after treatment [11]. At 12 weeks, 91% (31/34) of subjects were satisfied with the treatment [11].
In the present study, the results showed significant reduction of average knee circumference at 1 month (42.7 ± 4.2 cm), 3 months (41.9 ± 4.8 cm), 6 months (41.3 ± 4.4 cm) compared with baseline (p < 0.0001) (Table 3). Also, significant reduction in fat thickness of 2.0 ± 1.1 cm in axial plane and fat thickness of 2.0 ± 0.9 cm in sagittal plane at 1 month after treatment (p = 0.036, p = 0.001, respectively) and fat thickness of 1.5 ± 0.8 cm in axial plane and 1.6 ± 0.9 cm in sagittal plane at 6 months after treatment (p < 0.001) (Table 4) were also calculated based on ultrasound images. In our study, 17.7% of subjects at 3-month and 47.7% of subjects at 6-month follow-up visits rated > 75% improvement. The results of this study highlight that the 1060-nm diode laser is effective for subcutaneous fat reduction on medial knees. Considering that the laser device is kept in contact with the treated area using accessories (strap and frame) and the tapering of the temperature, the heat from the diode laser is localized to adipose tissue in the treatment area [10]. The patient satisfaction may be due to the medial knee fat reduction with smooth contour and lower rates of complications.
Similar to previously conducted studies, no severe adverse events were reported in our study [10, 11]. In a previous study using 924/975-nm diode laser, none of the patients presented persistent edema and pain. Of the 30 patients, 29 recommended the treatment [1]. In the study by Katz et al., the majority (83%) of reported events were mild and temporary. The subsequent events reported in the study by Katz were edema (resolved within 4–6 days), pain and bruising (resolved within 9–11 days), and subcutaneous nodules (resolved within 32–78 days) [10]. In addition, Bass and colleagues documented post-treatment tenderness as the most common adverse event [11]. Seventy-four percent of adverse events were reported as mild, 26% as moderate, and none as severe [11].
In our study, the average pain score recorded was 6.1 ± 1.0 (Table 1). All subjects reported mild tenderness and erythema immediately after treatment. No hypopigmentation, hyperpigmentation, scarring, fat dystrophy, infection, or paradoxical adipose hyperplasia were documented. The authors suggest that the best candidates and indications for noninvasive body contouring are patients who expect a mild to moderate result. Therefore, good candidates must be selected with realistic expectations.
In addition, our study showed that non-weight-gainers responded better to treatment. The average knee circumference of non-weight-gainers was reduced significantly at 1, 3, and 6 months after the single treatment (p < 0.001, p = 0.005, and p < 0.001, respectively) (Table 3). The average fat thickness of the non-weight-gainer group showed significant reduction at 6 months after treatment in both axial and sagittal plane (p < 0.001 and p < 0.001, respectively) (Table 4). Considering the current findings, the authors believe that diet control and regular exercise must be integrated with the subject’s lifestyle to maintain the treatment results and patient satisfaction.
To the best of our knowledge, this is the first study reporting the clinical efficacy and safety of a 1060-nm diode laser in the treatment of localized fat on medial knees. The limitations of the study include the small sample size, the lack of a comparative group, and short follow-up period. It would be prudent to conduct related studies with more subjects, additional treatment sessions, and longer follow-up to further examine the safety and efficacy of the 1060-nm diode laser on medial knees.
Conclusions
The 1060-nm diode laser demonstrated significant efficacy for knee circumference and medial knee fat layer thickness reduction. The future of the 1060-nm diode laser looks bright given its favorable safety profile.
References
Moreno-Moraga J, Trelles MA, Mordon S, et al. Laser-assisted lipolysis for knee remodelling: a prospective study in 30 patients. J Cosmet Laser Ther. 2012;14(2):59–66.
Chamosa M. Liposuction of the kneecap area. Plast Reconstr Surg. 1997;99(5):1433–8.
Brañas EB, Moraga JM. Laser lipolysis using a 924- and 975-nm laser diode in the lower extremities. Aesthetic Plast Surg. 2013;37(2):246–53.
Sugawara J, Kou S, Kokubo K, et al. Application for lower facial fat reduction and tightening by static type monopolar 1-MHz radio frequency for body contouring. Lasers Surg Med. 2017;49(8):750–5.
Wanitphakdeedecha R, Sathaworawong A, Manuskiatti W. The efficacy of cryolipolysis treatment on arms and inner thighs. Lasers Med Sci. 2015;30(8):2165–9.
Jalian HR, Avram MM. Cryolipolysis: a historical perspective and current clinical practice. Semin Cutan Med Surg. 2013;32(1):31–4.
Putra IB, Jusuf NK, Dewi NK. Utilisation of cryolipolysis among asians: a review on efficacy and safety. Open Access Maced J Med Sci. 2019;7(9):1548–54.
Saedi N, Kaminer M. New waves for fat reduction: high-intensity focused ultrasound. Semin Cutan Med Surg. 2013;32(1):26–30.
Hong JY, Ko EJ, Choi SY, et al. Efficacy and safety of high-intensity focused ultrasound for noninvasive abdominal subcutaneous fat reduction. Dermatol Surg. 2020;46(2):213–9.
Katz B, Doherty ST. Safety and efficacy of a noninvasive 1060 nm diode laser for fat reduction of the flanks. Dermatol Surg. 2018;44:388–96.
Bass LS, Doherty ST. Safety and efficacy of a noninvasive 1060 nm diode laser for fat reduction of the abdomen. J Drugs Dermatol. 2018;17(1):106–12.
Schilling L, Saedi N, Weiss R. 1,060 nm diode hyperthermic laser lipolysis: the latest in noninvasive body contouring. J Drugs Dermatol. 2017;16(1):48–52.
Decorato JW, Chen B, Sierra R. Subcutaneous adipose tissue response to a non-invasive hyperthermic treatment using a 1060 nm laser. Lasers Surg Med. 2017;49(5):480–9.
Acknowledgements
Funding
This research project, and the journal’s Rapid Service Fee, was supported by the Faculty of Medicine Siriraj Hospital, Mahidol University.
Authorship
All named authors meet the International Committee of Medical Journal Editors criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Author contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Chadakan Yan, Ploypailin Tantrapornpong, and Panittra Suphatsathienkul, Nittaya Lektrakul, Thanya Techapichetvanich, Sasima Eimpunth and Woraphong Manuskiatti. Rungsima Wanitphakdeedecha had full access to all the data in the study and takes responsibility for the integrity of data and the accuracy of the data analysis. The first draft of the manuscript was written by Kristy Elleza R. Evangelista and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Medical writing, editorial, and other assistance
The authors wish to thank Ms. Phonsuk Yamlexnoi, Ms. Chutikan Kiatphansodsai, Ms. Apichaya Jutaphonrakul, and Dr. Surachet Sirisuthivoranunt for their assistance in recruiting subjects and managing the database.
Disclosures
Chadakan Yan, Rungsima Wanitphakdeedecha, Kristy Elleza R. Evangelista, Ploypailin Tantrapornpong, Panittra Suphatsathienkul, Nittaya Lektrakul, Thanya Techapichetvanich, Sasima Eimpunth, and Woraphong Manuskiatti have nothing to disclose.
Compliance with ethics guidelines
The study was approved by the ethics committee of the Siriraj Institutional Review Board (Si 369/2018). Written informed consent was obtained for the publication and use of all patients’ images prior to their enrollment in the study. This study was performed in accordance with the Helsinki Declaration of 1964 and its subsequent amendments.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Thanking patient participant(s)
We thank the patients who participated in the study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visithttp://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Yan, C., Wanitphakdeedecha, R., Evangelista, K.E.R. et al. Efficacy of Noninvasive 1060-nm Diode Laser for Medial Knee Fat Reduction. Dermatol Ther (Heidelb) 12, 1253–1261 (2022). https://doi.org/10.1007/s13555-022-00730-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13555-022-00730-0