
Abstract
The use of point-of-care ultrasound in trauma provides diagnostic clarity and routinely influences management. A scanning protocol known as the Focused Assessment with Sonography in Trauma (FAST) has been widely adopted by trauma providers of all specialties. The FAST exam addresses a broad array of pathologic conditions capable of causing instability, including hemoperitoneum, hemopericardium, hemothorax, and pneumothorax. The exam is an integral component to the primary assessment of injured patients and an iconic application of point-of-care ultrasound.
This review article aims to summarize the application of the FAST exam with special consideration, where relevant, to anesthesiologists. The scope of the FAST exam, technical considerations, and clinical decision-making in trauma are explored.
Résumé
Dans les cas de traumatisme, l’utilisation de l’échographie au chevet procure une facilité diagnostique et a souvent un impact sur la prise en charge. Un protocole d’examen, connu sous l’acronyme FAST (pour Focused Assessment with Sonography in Trauma, soit Évaluation ciblée du traumatisme grâce à l’échographie), a été largement adopté par les spécialistes de traumatologie dans toutes les spécialités. L’examen FAST porte sur un vaste éventail de conditions pathologiques pouvant provoquer une instabilité, y compris l’hémopéritoine, l’hémopéricarde, l’hémothorax et le pneumothorax. L’examen est une composante intégrale de l’évaluation initiale des patients blessés et une application phare de l’échographie au chevet.
Ce compte rendu vise à résumer l’application de l’examen FAST et porte une attention particulière, le cas échéant, aux anesthésiologistes. L’objectif de l’examen FAST, des considérations techniques et la prise de décision clinique en trauma sont expliquées.
Similar content being viewed by others



Avoid common mistakes on your manuscript.
Over the last 30 years, the incorporation of point-of-care ultrasound within the initial assessment of the injured patient has become an essential skill for trauma providers.1 The Focused Assessment with Sonography in Trauma (FAST) exam is a goal-directed ultrasound protocol fashioned to address common life-threatening injuries in traumatized patients.
Originally derived to assess for hemoperitoneum and hemopericardium, the FAST examination has evolved since its original introduction to North American trauma centres in the 1990s.2,3 The scanning protocol now routinely includes the assessment for hemothorax and pneumothorax. This expanded format may be referred to as the extended FAST or “eFAST” exam, but as this scope has become routine, special distinctions are no longer necessary.
The FAST exam is rapidly performed and can be completed in concert with the trauma primary survey. The exam has good diagnostic performance and, in the presence of altered physiology, can lead to life-saving interventions at the bedside or expedite transfer to definitive care.4,5,6,7
Statement of purpose
This review article aims to introduce the basic components of the FAST examination, with attention to methods of image acquisition and interpretation. We also aim to outline the role of the FAST examination in patient care from an anesthesiologist’s perspective.
FAST exam and the anesthesiologist
Anesthesiologists have been proficient users of perioperative ultrasound for over thirty years, with a scope that continues to evolve.8 Although the FAST examination is typically the domain of the front-line traumatologist, the incorporation of the FAST examination into the anesthesiologist’s armamentarium is feasible and has merit.9 Fluency in trauma ultrasound and in its implications for surgical disposition is recommended for any anesthesiologist who routinely cares for injured patients (Fig. 1).

Typical blunt abdominal trauma algorithm and role of the assessment for free abdominal fluid in decision-making
Beyond its traditional role in the trauma suite, the components of the FAST exam may be of additional value to the anesthesiologist caring for patients who deteriorate after abdominal procedures, allowing rapid assessment for evolving intra-abdominal hemorrhage, whether in the operating room, postanesthesia care unit, or intensive care unit.9 Furthermore, intraoperative assessment with ultrasound has been shown to facilitate the identification of pneumothorax, a condition that can go unrecognized in the trauma bay and may worsen as the patient is exposed to positive pressure ventilation.10,11,12
Components of the FAST exam
There are eight essential views that comprise a complete FAST examination. These are summarized in the Table.
Image acquisition and interpretation
Equipment
As the FAST exam calls for only two-dimensional images, even the most basic modern-day, portable ultrasound machine may be used. The FAST exam is centred on torso imaging and therefore calls for a low frequency (1-5 MHz) transducer capable of adequate tissue penetration. The two most commonly available transducers in this frequency range are the curvilinear probe and the phased array probe (Fig. 2). Either probe is appropriate for the FAST examination, though we favour the phased array probe for its smaller footprint and ability to resolve cardiac motion temporally.

Transducers suitable for the Focused Assessment with Sonography in Trauma (FAST) exam: the curvilinear (left) and phased array (right) probes each offer excellent penetration into the abdomen and thorax due to their low frequency (2-5 MHz). Note the smaller footprint of the phased array probe – ideal for imaging between ribs
Hemoperitoneum
Right upper quadrant (RUQ)
Right upper quadrant anatomy
The hepatorenal interface, known as Morison’s pouch, has been shown to be the most common region in which hemoperitoneum is detected during a FAST examination.13 Given this predilection for fluid to collect in the right upper quadrant (RUQ), it is the first view obtained when performing the FAST exam.
Right upper quadrant image acquisition
The RUQ is not only the most sensitive view for the detection of hemoperitoneum but is also the easiest image to acquire. The RUQ view is performed by placing a longitudinally oriented probe where the mid-axillary line meets the costal margin (Fig. 3). The solid organ appearance of the liver and the renal “double density” (black/anechoic cortex and white/hyperechoic medulla) are readily recognizable (Fig. 4).

Image acquisition of the abdominal component of the Focused Assessment with Sonography in Trauma (FAST) exam. (A) (B) Upper quadrant views are performed by orienting the index marker on the probe toward the patient’s head. (C) Pelvic image acquisition is performed by placing the probe in a horizontal plane above the pubic symphysis. (D) The probe is then rotated 90 degrees into a longitudinal plane in the midline. Note the red marker indicating the direction of the probe marker

A normal right upper quadrant examination. The readily recognizable double density of the kidney is juxtaposed with the liver. The potential hepatorenal space is nonexistent (white arrow), and the clinician should see the hyperechoic fascia that surrounds the kidney abutting against the liver. K = kidney; L = liver
There are two important considerations when interrogating both upper quadrants. First, the entire length of the interface where the kidney meets the liver/spleen, including the inferior pole of the kidney, must be visualized. Second, Morison’s pouch and the perisplenic interface are three-dimensional spaces, and the clinician must “sweep” the ultrasound beam through this space to image them completely (Video 1; available from Electronic Supplemental Material [ESM]).
Right upper quadrant image interpretation
Once an image of the juxtaposed liver and kidney is captured, the clinician’s attention should be directed to the hepatorenal interface. In a negative RUQ view, the liver and kidney will be tightly apposed to one another without any interceding fluid (Fig. 4). In a positive study, anechoic appearing blood will pool at this interface and create a black layer that separates these two organs (Fig. 5).

A positive right upper quadrant scan reveals anechoic blood pooling in the hepatorenal interface (white arrow). L = liver; K = kidney
If adequate views are not obtained due to operator, patient, or equipment factors, the exam must be interpreted as indeterminate and no clinical decisions should be made based on the exam. If the clinician interprets a positive exam in the RUQ, no further abdominal images need to be obtained, the presence of hemoperitoneum has been diagnosed and patient stability will dictate the next step in care (Fig. 1). If a negative or indeterminate RUQ study is interpreted, the clinician must continue with the remaining abdominal views.
Left upper quadrant (LUQ)
Left upper quadrant anatomy
There are important anatomic distinctions between the LUQ and the RUQ. The presence of the phrenicocolic ligament tends to direct free fluid to the subphrenic space, rather than to the renal interface. Compared with the RUQ, the kidney sits higher on the left side, structures are more cephalad, and some adjustments to technique are required.
Left upper quadrant image acquisition
An adequate LUQ view often requires the probe be more posterior than with the RUQ. In addition to observing the splenorenal interface, the subphrenic interface must be seen (Fig. 6). Observing the diaphragm is often challenging due to multiple artifacts, including those generated from aerated lungs and rib shadows.

Left upper quadrant view. Assessing the subphrenic space is an essential component of assessing the left upper quadrant. This assessment ideally captures a continuous stripe of the diaphragm as it wraps around the medial spleen tip (shown by the white arrow). S = spleen; K = kidney)
Left upper quadrant image interpretation
Just as in the RUQ, interpretation of the LUQ view hinges on finding anechoic fluid collecting between solid organs and interrupting otherwise clean interfaces (Fig. 7).

Positive left upper quadrant examination. A subtle amount of fluid can be seen collecting in the subphrenic and splenorenal interface (arrows). S = spleen; K = kidney
Pelvis
Pelvic anatomy
The pelvic anatomy relevant to the FAST exam is more straightforward. In males, the region lies in the rectovesicular pouch. In females, fluid can be found collecting in the potential space between the posterior wall of the uterus and the rectum in the rectouterine space (pouch of Douglas).
Pelvic image acquisition
To maximize sensitivity, acquisition of the pelvic image is performed in two planes (Fig. 3). Image quality relies heavily on the presence of an adequately filled urinary bladder. For patients with Foley catheters, the creation of an acoustic window has been described by instilling fluid into the bladder retrograde through the catheter.
The urinary bladder should be visualized in the near field, and the uterus and/or the rectum will be seen deep to the bladder. Moving the probe subtly will allow imaging of the entire potential space in the search for free fluid.
Pelvic image interpretation
Just as in all the other views, varying amounts of anechoic content will represent free fluid. Anechoic free fluid will be detected immediately posterior to the bladder in males and/or in the pouch of Douglas in females (Fig. 8).

Positive pelvic examination (A) Male patient with anechoic fluid collecting in the rectovesicular space (white arrow) (B) Female patient with anechoic fluid collecting in both the vesicouterine pouch and the rectouterine pouch (pouch of Douglas; white arrow). B = bladder; U = uterus
Pearls and pitfalls of the abdominal exam
-
Repeating the abdominal ultrasound exam sequentially is encouraged in a patient who is highly suspicious for intraperitoneal fluid or has a sudden change in hemodynamics, as repeat FAST exams have been shown to increase sensitivity.14
-
Trendelenburg positioning has also been shown to increase the sensitivity of the RUQ FAST exam by using gravity to drive fluid up the pericolic gutters into the RUQ and, to a lesser extent, the LUQ.15
-
The FAST examinations completed early in the patient’s course of illness may be falsely negative as it takes time for intraperitoneal fluid to collect.
-
Once blood has begun to coagulate, it creates an iso- or hyperechoic appearance that may not be interpreted accurately (false negative) (Fig. 9).
Fig. 9 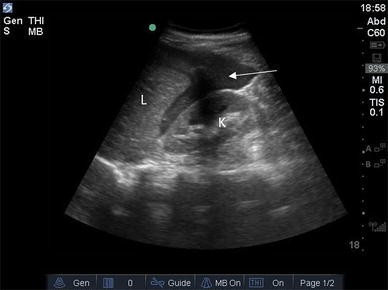
A right upper quadrant view demonstrating that the appearance of hemoperitoneum is more echogenic as coagulation occurs. This can lead to a false-negative interpretation, as the appearance of hemoperitoneum can be difficult to distinguish from the hepatic and splenic parenchyma. L = liver; K = kidney. White arrow indicates coagulated blood

Hemopericardium
Pericardial anatomy
With cardiac injury, rapid accumulation of hemopericardium can lead to significant hemodynamic compromise through cardiac tamponade.
Pericardium image acquisition
Due to its abdominal approach and feasibility from a supine patient position, the subcostal four-chamber view has evolved as the standard choice for imaging the pericardium in the setting of trauma (Fig. 10).

(A) The subcostal four-chamber view is obtained by placing the ultrasound probe in a transverse position with the index marker pointing towards the patient’s right (red dot—NB: this is the trauma/ER convention. If using the cardiology convention, the index mark may point to the patient’s left side). (B) A normal subcostal four-chamber view demonstrating the superficial liver which acts as an acoustic window to the heart. The bright echogenic structure (white arrow) represents the pericardium
The near-field image is of the superficial liver, which acts as an acoustic window to the heart. Beyond the liver, a bright echogenic structure represents the pericardium which encases the heart (Fig. 10).
There could be many reasons why the subcostal four-chamber view may not be visualized, including body habitus, abdominal dressings, and subcutaneous emphysema. In these situations, additional echocardiographic views, such as the parasternal long- or short-axis view, can be employed to assess the pericardium with high sensitivity.
Pericardium image interpretation
Once the echogenic pericardium has been identified, the clinician assesses for the presence or absence of anechoic free fluid collecting between this bright pericardium and the cardiac muscle (Fig. 11).

Two examples of a positive subcostal chamber view. (A) Large pericardial effusion (B) A smaller pericardial effusion, but one that should be considered clinically relevant in a trauma patient presenting with hemodynamic instability or penetrating thoracic trauma. Until proven otherwise, any amount of pericardial fluid must be considered to represent evolving hemorrhage due to cardiac injury
Pearls and pitfalls of the pericardial exam
-
Epicardial fat is a common source of a false-positive subcostal pericardial exam (Fig. 12).
-
As hemopericardium begins to coagulate, it becomes more iso- or hyperechoic.
-
Small pericardial effusions may lead to important hemodynamic consequences as the physiology of a rapidly accumulating hemopericardium is vastly different from slowly acquired medical effusion.
Fig. 12 
False-positive pericardial assessments are often due to epicardial fat. Typically located anterior to the right ventricle, distinguishing features of epicardial fat, demonstrated by the arrow, are that it rarely tracks around the left ventricle and it often has a iso-dense, speckled appearance.

Pneumothorax
Background
Chest radiograph (CXR) has evolved as the most rapid and reliable method of detecting the hemo- and pneumothoraces. Nevertheless, ultrasound is superior to a CXR for detection of pneumothorax in the supine patient.16 The ease of image generation, interpretation, portability, and immediate availability has led to the incorporation of thoracic ultrasound in the FAST examination.
Anatomic considerations in assessing for pneumothorax
With traumatic injuries, air can become entrained within the pleural space. In the supine trauma patient, image acquisition is directed at the most dependent location for air, the anterior thoracic wall.
Pneumothorax image acquisition
The exam begins by imaging the anterior chest by placing the probe longitudinally in the mid-clavicular line between the second and fourth rib (Fig. 13).

Image acquisition for the assessment of pneumothorax. The probe’s footprint rests mostly in a rib space, and the index marker is directed at the patient’s head
The resulting image will show chest wall soft tissue in the near field, followed by ribs (and their corresponding rib shadows). The area of interest to the clinician is the pleural line, which is the first hyperechoic line seen deep to the ribs (Fig. 14).

Standard sonographic appearance of the anterior chest in the assessment for pneumothorax. R = ribs. The arrow points at the pleural line
Pneumothorax image interpretation
In a normal lung, the pleural line can be seen sliding as ventilation creates movement between the visceral and parietal pleura. In the presence of pneumothorax, the two pleural layers are no longer apposed and sliding is absent as only the parietal pleura is seen (Video 2; available as ESM). The presence of lung sliding rules out pneumothorax at the site of the transducer with 100% accuracy. This power to rule out pneumothorax offers significant diagnostic advantage in an unstable patient and underlies the rapid uptake of this modality for trauma and for any context of cardiorespiratory failure.
The anterior chest wall offers the most sensitive location for detection of large life-threatening pneumothoraces. Marginal improvement in diagnostic accuracy for clinically significant pneumothoraces is gained with the addition of multiple scanning regions, but additional sites of insonation may be beneficial in some clinical scenarios (e.g., prior to air transport, long delays in radiography).17
Pearls and pitfalls of the assessment for pneumothorax
-
Imaging of the pleural space assesses for the presence or absence of pneumothorax only at the location of the transducer.
-
Absence of sliding is not specific to pneumothorax and may be caused by conditions that diminish or abolish normal pleural anatomy and function.
Hemothorax
The assessment of hemothorax is now routinely incorporated into the FAST examination. Ultrasonographic assessment provides similar sensitivity to CT for detection of hemothorax.17
Anatomic considerations in assessing for hemothorax
Thoracic trauma can result in bleeding within the thoracic cavity and lead to accumulation of blood in the pleural space. As with pneumothorax, the assessment for hemothorax interrogates the most dependent location for the intrapleural process. For the pooling blood of hemothorax, this is the mid-posterior costodiaphragmatic recess.
Hemothorax image acquisition
In the trauma scenario, an assessment of the pleural space for blood is closely related to the abdominal upper quadrant views. The clinician needs only to move the probe 1-2 rib spaces cephalad in the same coronal plane and to ensure the probe is in the mid-posterior axillary plane.
Hemothorax image interpretation
In the absence of fluid in the pleural space, the ultrasound image should show a well-aerated lung above the diaphragm that, during tidal breathing, will largely obliterate the view of the diaphragm or any solid organs with the characteristic “curtain sign”.
The presence of an acoustic window above the diaphragm and the absence of a curtain sign should raise the suspicion of the presence of fluid in the hemithorax. The sonographic appearance of hemothorax appears starkly black or may take on the appearance of a complex fluid, which may represent fibrin and clot forming within the ongoing hemorrhage (Fig. 15).

Image of the right hemithorax in a patient with a large hemothorax (white arrow). The anechoic region (with some complexity) cranial to the diaphragm is consistent with hemorrhage. D = diaphragm; L = collapsed lung
Pearls and pitfalls of the assessment for hemothorax
-
Thoracic ultrasound is quite sensitive, thus identification of pathology does not always necessitate intervention. While unstable patients with positive findings may need tube thoracostomy, stable patients will typically benefit from further radiographic studies to assess and trend the size and anatomic burden of the disease process.
-
Similar to the assessment of hemoperitoneum, blood appears iso- or hyperechoic as it begins to coagulate.
Future directions
The utilization of point-of-care ultrasound is rapidly growing in all disciplines of medicine.18,19,20,21,22 Within the care of trauma patients, a particular area of development that will be of interest to anesthesia providers is the use of ultrasound in traumatic brain injuries and its ability to detect intracranial hypertension through insonation of the optic nerve.23 Early work applying transcranial Doppler and transesophageal echocardiography in the trauma bay has also been described and appears promising.24,25,26,27
Training considerations
The number of scans required to achieve competency in performing and interpreting the FAST examination varies amongst practitioners.28,29 Emergency physicians practicing in Canada must perform 50 directly supervised scans before they are deemed to have achieved competency and receive credentialing to perform the FAST exam.30 That said, the authors discourage this kind of numeric, boilerplate approaches to credentialing and certification and instead favour incorporating point-of-care ultrasonography skills into the core competencies of residency training.31 This approach would ensure that all medical trainees responsible for the care of critically ill patients have baseline familiarity and skill with bedside sonography from which they can adopt advanced applications.
Conclusions
The FAST exam is one of the most widely used and iconic applications of point-of-care ultrasound. It rapidly surveys the torso for life-threatening events in the context of traumatic illness. The technical and cognitive elements outlined in this paper are transferable to multiple environments other than trauma, including the operating room or the postoperative setting where anesthesiologists are most likely to see its impact first hand.
References
Kool DR, Blickman JG. Advanced Trauma Life Support. ABCDE from a radiological point of view. 2007; 14: 135-41.
Tso P, Rodriguez A, Cooper C, et al. Sonography in blunt abdominal trauma: a preliminary progress report. J Trauma 1992; 33: 39-43.
Rozycki GS, Ochsner MG, Schmidt JA, et al. A prospective study of surgeon-performed ultrasound as the primary adjuvant modality for injured patient assessment. J Trauma 1995; 39: 492-8.
Melniker LA, Leibner E, Mckenney MG, Lopez P, Briggs WM, Mancuso CA. Randomized controlled clinical trial of point-of-care, limited ultrasonography for trauma in the emergency department: the first sonography outcomes assessment program trial. Ann Emerg Med 2006; 48: 227-35.
Nishijima DK, Simel DL, Simel DL, Wisner DH, Holmes JF. Does This adult patient have a blunt intra-abdominal injury? JAMA 2012; 307: 1517-27.
Wilkerson RG, Stone MB. Sensitivity of bedside ultrasound and supine anteroposterior chest radiographs for the identification of pneumothorax after blunt trauma. Acad Emerg Med 2010; 17: 11-7.
Ma OJ, Mateer JR. Trauma ultrasound examination versus chest radiography in the detection of hemothorax. Ann Emerg Med 1997; 29: 312-5.
Johnson DW, Oren-Grinberg A. Perioperative point-of-care ultrasonography: the past and the future are in anesthesiologists’ hands. Anesthesiology 2011; 115: 460-2.
Ramsingh D, Rinehart J, Kain Z, et al. Impact assessment of perioperative point-of-care ultrasound training on anesthesiology residents. Anesthesiology 2015; 123: 670-82.
Ball CG, Hameed SM, Evans D, Kortbeek JB, Kirkpatrick AW, Canadian Trauma Trials Collaborative. Occult pneumothorax in the mechanically ventilated trauma patient. Can J Surg 2003; 46: 373-9.
Ball CG, Kirkpatrick AW, Laupland KB, et al. Incidence, risk factors, and outcomes for occult pneumothoraces in victims of major trauma. J Trauma 2005; 59: 917-24; discussion 924-5.
Ueda K, Ahmed W, Ross AF. Intraoperative pneumothorax identified with transthoracic ultrasound. Anesthesiology 2011; 115: 653-5.
Rozycki G, Ochsner M, Feliciano D, et al. Early detection of hemoperitoneum by ultrasound examination of the right upper quadrant: a multicenter study. J Trauma 1998; 45: 878-83.
Blackbourne LH, Soffer D, McKenney M, et al. Secondary ultrasound examination increases the sensitivity of the FAST exam in blunt trauma. J Trauma 2004; 57: 934-8.
Abrams BJ, Sukumvanich P, Seibel R, Moscati R, Jehle D. Ultrasound for the detection of intraperitoneal fluid: the role of Trendelenburg positioning. Am J Emerg Med 1999; 17: 117-20.
Blaivas M, Lyon M, Duggal S. A prospective comparison of supine chest radiography and bedside ultrasound for the diagnosis of traumatic pneumothorax. Acad Emerg Med 2005; 12: 844-9.
Brooks A, Davies B, Smethhurst M, Connolly J. Emergency ultrasound in the acute assessment of haemothorax. Emerg Med J 2004; 21: 44-6.
Helland G, Gaspari R, Licciardo S, et al. Comparison of four views to single-view ultrasound protocols to identify clinically significant pneumothorax. Acad Emerg Med 2016; 23: 1170-5.
Arntfield R, Pace J, Hewak M, Thompson D. Focused transesophageal echocardiography by emergency physicians is feasible and clinically influential: observational results from a novel ultrasound program. J Emerg Med 2016; 50: 286-94.
Lichtenstein D, Goldstein I, Mourgeon E, Cluzel P, Grenier P, Rouby JJ. Comparative diagnostic performances of auscultation, chest radiography, and lung ultrasonography in acute respiratory distress syndrome. Anesthesiology 2004; 100: 9-15.
Woo MY, Hecht N, Hurley B, Stitt D, Thiruganasambandamoorthy V. Test characteristics of point-of-care ultrasonography for the diagnosis of acute posterior ocular pathology. Can J Ophthalmol 2016; 51: 336-41.
Costantino TG, Parikh AK, Satz WA, Fojtik JP. Ultrasonography-guided peripheral intravenous access versus traditional approaches in patients with difficult intravenous access. Ann Emerg Med 2005; 46: 456-61.
Dubost C, Le Gouez A, Jouffroy V, et al. Optic nerve sheath diameter used as ultrasonographic assessment of the incidence of raised intracranial pressure in preeclampsia: a pilot study. Anesthesiology 2012; 116: 1066-71.
Turek R, Linzer P, Filip M, Samal F, Jurek P. Application of transcranial color-coded sonography in severe brain injury. Acta Neurochir Suppl 2013; 118: 265-7.
Landau JH, Power AH, Leeper WR, Arntfield RT. Bedside identification of blunt thoracic aortic injury with point-of-care transesophageal echocardiography. Trauma 2016; 18: 287-90.
Llompart Pou JA, Abadal Centellas JM, Palmer Sans M, et al. Monitoring midline shift by transcranial color-coded sonography in traumatic brain injury. A comparison with cranial computerized tomography. Intensive Care Med 2004; 30: 1672-5.
Jaffres P, Brun J, Declety P, et al. Transcranial Doppler to detect on admission patients at risk for neurological deterioration following mild and moderate brain trauma. Intensive Care Med 2005; 31: 785-90.
Frezza EE, Solis RL, Silich RJ, Spence RK, Martin M. Competency-based instruction to improve the surgical resident technique and accuracy of the trauma ultrasound. Am Surg 1999; 65: 884-8.
Ma OJ, Gaddis G, Norvell JG, Subramanian S. How fast is the focused assessment with sonography for trauma examination learning curve? Emerg Med Australas 2008; 20: 32-7.
Canadian Point of Care Ultrasound Society. CEUS Certification. Available from URL: https://www.cpocus.ca/ceus-certifications/levels-certification/basic-ip-1-certification/ (accessed September 2017).
Mok D, Schwarz SK, Rondi K. Point-of-care ultrasonography in Canadian anesthesiology residency programs: a national survey of program directors. Can J Anesth 2017. https://doi.org/10.1007/s12630-017-0935-8.
Conflicts of interest
Dr. Arntfield has served as an educational consultant for Fujifilm Sonosite Inc.
Editorial responsibility
This submission was handled by Dr. Gregory L. Bryson, Deputy Editor-in-Chief, Canadian Journal of Anesthesia.
Funding
None
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary material 1 (MP4 47535 kb) Video 1 A complete Focused Assessment with Sonography in Trauma (FAST) examination in a healthy individual.
Supplementary material 2 (MP4 228 kb) Video 2 A right anterior chest wall view demonstrating the lack of lung sliding indicative of a pneumothorax at the site of insonation. Note that the image is acquired with a vascular probe, as evidenced by the transducer’s linear footprint.
Rights and permissions
About this article

Cite this article
Pace, J., Arntfield, R. Focused assessment with sonography in trauma: a review of concepts and considerations for anesthesiology. Can J Anesth/J Can Anesth 65, 360–370 (2018). https://doi.org/10.1007/s12630-017-1030-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-017-1030-x