
Abstract
Understanding how countries improve children’s nutrition can inform policies and contribute to further improvements. We examined the relationship between improvements in nutrition in Rwanda (1992–2017) and political commitment to- and policy coherence in- nutrition. We reviewed nutrition-relevant Rwandan policies and programs (2000–2018) and conducted 90 semi-structured interviews with national (n = 32), mid-level (n = 38), and community (n = 20) nutrition stakeholders and 40 community-level focus group discussions (FGDs). FGDs and sub-national interviews were conducted in ten purposefully selected districts, five each in which stunting decreased (reduced) and increased or stagnated (non-reduced) between the 2010 and 2014/15 Rwanda Demographic and Health Surveys. Analysis consisted of thematic analysis and the assessment of events, policy developments, and strategies that influenced nutrition in Rwanda, including operationalization of political commitment and policy coherence for nutrition. Political and institutional commitment to nutrition increased in Rwanda as evidenced by the adoption of a multisectoral nutrition policy that was reinforced with national and subnational horizontal coordination platforms. These platforms strengthened multisectoral strategies to address nutrition and supported operational and institutional commitment. The role of mid-level actors in nutrition governance increased as responsibilities for planning, implementing, and monitoring nutrition programs were increasingly delegated to sub-national administrative levels. Variations in policy implementation existed between reduced and non-reduced districts. Despite improvements, challenges remained in coordination, financial commitment, and capacity to address, monitor, and evaluate nutrition. Political commitment to- and policy coherence in- nutrition at the national level are important for improving nutrition, and when reinforced institutionally, can be translated to sub-national levels where implementation occurs.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Undernutrition remains highly prevalent and a global challenge, with Africa and Asia bearing the greatest burden of stunting and wasting (WHO et al., 2019). Given the high prevalence of undernutrition and its associated human and economic costs to populations, countries, and development, attention has increased on what countries can do to reduce undernutrition (Black et al., 2013; Caulfield et al., 2004; Gillespie et al., 2013; Victora et al., 2008). This increased attention has reinforced the need to address nutrition in a multisectoral manner, through the engagement of the different sectors that influence nutrition in policy and programs, and the enabling environment for nutrition, such as leadership, horizontal and vertical coordination, and capacity (Black et al., 2013; Gillespie et al., 2013; Ruel & Alderman, 2013). Addressing the enabling environment recognizes that targeting the immediate and underlying determinants of undernutrition or economic growth alone do not always translate into improved nutrition outcomes, especially regarding reducing child stunting (Mejía Acosta & Haddad, 2014; Menon et al., 2011). Rather, the complex political, policy, and operational domains that affect how countries address nutrition must be considered (Gillespie et al., 2013; Lapping et al., 2012; Pelletier et al., 2012). The experiences of countries that successfully reduced child stunting show that interlinked political, policy, and institutional processes, including political commitment and policy coherence in nutrition, contributed to changes in nutrition programming and eventually in nutritional status (Gillespie and van den Bold 2017; Harris et al., 2017; Kampman et al., 2017; Mejía Acosta & Haddad, 2014).
Political commitment to nutrition is the intent and reflection of that intent through policy, processes, resources, and sustained actions over time to improve nutrition (Baker et al., 2018; Development Initiatives, 2017; Gillespie & Bold, 2017; Heaver, 2005; Lintelo & Lakshman, 2015). Political commitment can take four forms: rhetorical (political attention and stated intent through speech), institutional (reflection of rhetorical commitment through policy, structures, and procedure), operational (translation of rhetorical and institutional commitment from all actors involved in implementation), and financial (financial resources needed for implementation) (Table 1). Countries with high political commitment to nutrition generate the political attention needed to prioritize nutrition, place it high on the political agenda, and ultimately create and adopt relevant policies (Heaver, 2005; Hoey & Pelletier, 2011; Pelletier et al., 2012). Many countries, however, face challenges transforming this prioritization into other forms of political commitment that can sustain the prioritization through concrete actions and effective implementation (Gillespie & Bold, 2017; Heaver, 2005).
Policy coherence in nutrition occurs when political commitment to nutrition is converted into a system that has institutional structures and processes to coordinate nutrition policy and program implementation in a mutually reinforcing manner (Gillespie & Bold, 2017). Given that nutrition is multisectoral, actions to address nutrition cut across different sectors. Policy coherence in nutrition, therefore, consists of the coordination and consistency of actions in relation to nutrition across institutions with coordination responsibilities (institutional coherence), sectors and actors related to nutrition (horizontal coherence), and administrative levels (vertical coherence) (Garrett & Natalicchio, 2011).
Research on nutrition governance has mostly focused on political commitment and policy coherence at the national level, with attention to the establishment of national nutrition coordination bodies and coordination across national ministries (Garrett & Natalicchio, 2011; Gillespie & Bold, 2017; Kampman et al., 2017; Mejía Acosta & Fanzo, 2012). Countries also face challenges translating the political commitment observed at national level to mid-level actors who oversee the coordination and implementation of nutrition-related actions at sub-national levels (Baker et al., 2018; Heaver, 2005; Hoey & Pelletier, 2011). Studies that have explored the experiences of mid-level actors working on nutrition find that they believe there is minimal sense of responsibility for nutrition outside of the health sector, which leads to weak horizontal coherence among sectors (Kennedy et al., 2015; Warren & Frongillo, 2017). Furthermore, these actors believe that resources, personnel, and training are insufficient to address nutrition at the sub-national level.
The aim of this study was to understand the role of political commitment to nutrition and policy coherence in reducing undernutrition in Rwanda between 1992–2017 from the perspective of national, mid-level, and community (i.e., local) actors. We used previously established theoretical frameworks of political commitment and policy coherence to understand how commitment and coherence contributed to the nutritional improvements observed in the country. During this period, Rwanda experienced substantial improvements in children’s nutrition. Between 2005 and 2015, the prevalence of stunting among children under 5 years of age fell from 52 to 38%, wasting was nearly eliminated, and anemia among children 6–59 months of age decreased from 50 to 36% (NISR et al., 2015).
2 Methods
2.1 Context
Rwanda has faced many political and social challenges over the years, including the 1994 genocide against Tutsis. The country has made great efforts to rebuild and restructure following this tragedy. In 2001, Rwanda adopted a national decentralization policy to reform public sector governance. Decentralization is the dispersion of responsibilities such as public planning, management, and decision-making from centralized national levels to lower levels of government. The policy aimed to improve service delivery, empower people to partake in local development, and enhance transparency and accountability of local governments to communities as the country reconstructed post the genocide (Kauzya, 2007; Ministry of Local Government, 2012) To achieve this, the policy restructured and condensed its administrative structure in 2006 and devolved responsibilities and functions to lower levels of government.
Previously divided into 12 provinces and over 150 districts (referred to as communes), Rwanda today has five provinces that consist 30 districts (Table 2) (World Bank, 2015). Districts are further divided into the administrative units of sectors, cells, and villages. Districts are led by a mayor and two vice mayors, one of economic affairs and another of social affairs, and are responsible for coordinating planning, financing, and overseeing the implementation of most public services, including health, education, and agriculture (RGB, 2018; World Bank, 2015). Districts are financed through both locally generated revenues such as property taxation, trading licenses, land rent, and intergovernmental transfers from the central national government (World Bank, 2015). While the amount of locally generated revenue has increased, from 49 billion Rwandan Francs in 2006 to 440 billion Rwandan Francs in 2017/18, this amount only makes up 10 to 15% of district financing (RGB, 2018). Most district funds continue to come from the national government.
Planning at the district level is divided into medium-term five-year district development strategies (DDSs) and yearly action plans. These plans translate national policies from the central government into actions that address the local needs of each district. The delivery of basic services and reporting are conducted at the sector level of the administrative structure, which is led by an executive secretary and committee. The cell unit, also led by a secretariat of district staff, is responsible for conducting community mobilization and needs assessments and prioritizations (World Bank, 2015). The village, though not considered a formal administrative unit, is led by an executive committee of elected village leaders.
2.2 Study design
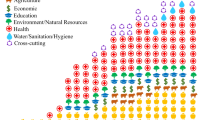
For this study we conducted a document review of nutrition-relevant programs and policies along with semi-structured interviews and focus group discussion (FGDs) with key stakeholders in nutrition (Fig. 1).

Study design
2.3 Document review
The purpose of the document review was to understand changes in policy and governance that occurred in Rwanda between 2000 to 2018. Through this review, we synthesized information on nutrition and nutrition-related policies and programs in Rwanda during that period. Nutrition-relevant policies that were included came from sectors that affect nutrition and that have responsibilities in nutrition per the national nutrition policy (Black et al., 2013; NFNP, 2013). These sectors were agriculture, education, social protection, gender, water and sanitation, and economic development (Supplemental 1). Specifically, the policy review assessed if and how nutrition as an objective was addressed and how nutrition-related actions and indicators to track progress had been integrated in policies.
2.4 Sample for interviews and focus group discussions
We conducted district- and community-level interviews in all five provinces: North, South, East, West, and the City of Kigali. In each province using results of the DHS 2010 and 2024/15 survey, we selected two districts. Given that improvements in undernutrition varied across districts, assessing the effect of political commitment and policy coherence in relation to the extent of improvement in nutrition outcomes was important. We, therefore, purposively selected one district with the largest reduction in stunting prevalence (reduced district) and one district with the lowest reduction or the highest increase in stunting prevalence (non-reduced district). In total, 10 study districts were selected (Table 3). To determine where community-level interviews would be conducted, we first ranked sectors (administrative unit) within each of the selected districts based on the type of roof, wall, and energy used for lighting according to Rwanda’s Fourth Population Housing Census (National Institute of Statistics of Rwanda & Ministry of Finance and Economic Planning, 2014). We then randomly selected two sectors, one from the low and one from the middle ranking, of those district lists for a total of 20 sectors.
Our study included 90 key informant semi-structured interviews and 40 focus group discussions (FGD) (Table 4). At national level, we conducted 32 semi-structured interviews with government stakeholders (technical staff and ministry leaders) from the different ministries involved in nutrition (n = 8) (e.g., health, agriculture, gender, education) per Rwanda’s National Food and Nutrition Policy 2013–2018 (NFNP) and non-government stakeholders from civil society (n = 10) and donor, international, and non-governmental organizations (n = 14). The organizations included were purposefully selected with in-country collaborators based on the organizations’ involvement in nutrition in Rwanda. Snowball sampling was also used to identify additional respondents and organizations. Selected ministries and organizations identified their respective respondents based on who they believed was best positioned to participate in the interview given the study’s aim.
At the district level, we conducted 38 semi-structured interviews, 20 in reduced districts and 18 in non-reduced districts. District-level respondents were mid-level actors from the health, agriculture, local government, and nutrition sectors involved in the coordination and implementation of nutrition and nutrition-related activities. These respondents, selected based on their job position, represented district leaders such as vice mayors of social affairs, directors of health, directors of agriculture, and district nutritionists.
At the community level, we conducted 20 interviews with frontline workers who provide community services in health (community health workers) and agriculture (agriculture extension workers). Frontline workers were selected with the help of local leaders in charge of nutrition at the sector (administrative unit) level. We also conducted 20 community FGDs (10 male and 10 female) in both reduced and non-reduced districts (n = 40) to gain community members’ perspectives on nutrition, changes in nutrition, and contributors to changes in nutrition. Each FGD consisted of either 10 males or 10 females who worked in agriculture and lived in the same catchment area as frontline workers interviewed. At least one-third of participants had to have children under the age of five years because child nutrition was a key topic of discussion.
2.5 Data collection
All data were collected between June and November 2017. Separate interview guides were developed for the different types of respondents and FGDs, but they covered similar topics. Interview respondents received a letter with the study’s aim, intent, and the organizations involved in the study, and gave signed consent to participate in the study. FGD participants provided oral consent to participate and selected one representative to provide signed consent on behalf of the group.
Interviews at the national and district levels were conducted by the lead author and a colleague with training in qualitative methods. Frontline worker interviews and FGDs were conducted by trained data collectors. All interviews and FGDs were audio recorded, with consent from respondents. When consent to audio-record was not given (n = 9 or 10% for semi-structured interviews; n = 0 for FGDs), detailed notes were taken. Rwanda has three official languages: English, French, and Kinyarwanda (Republic of Rwanda, 2021). Study instruments were translated in the three official languages, and interviews were conducted in the language chosen by each respondent. Interviews at the national level were conducted in English (n = 23), French (n = 1), or Kinyarwanda (n = 8). Interviews conducted at the district and community level and FGDs were conducted in Kinyarwanda. Interviews were translated and transcribed into English and FGDs into French because it was the language in which the transcribers were most fluent. The lead author who led data collection and analysis is fluent in all three languages.
This study received approval from the institutional review boards of the University of South Carolina, the International Food Policy Research Institute, and the Rwanda National Ethics Committee.
2.6 Data analysis
Data analysis was informed by the 5C’s framework developed by the Stories of Change in Nutrition case studies, by which this study was guided (Gillespie & van den Bold, 2017). The 5C’s framework (changes, challenges, commitment, coherence, and community) examines changes in commitment, coherence, and community in relation to improvements in undernutrition and the challenges that remain in these categories in different contexts (Gillespie, 2015). For political commitment to nutrition, we drew from the framing in Stories of Change in Nutrition (Gillespie & Bold, 2017), Heaver (2005), and Baker and colleagues (2018) to identify four forms of commitment to examine: rhetorical, institutional, operational, and financial commitment. For policy coherence, we used the framing from Stories of Change in Nutrition along with Garret and Natalicchio’s (2011) framework to assess institutional (across the different coordination platforms established to address nutrition at national level), horizontal (across sectors and actors involved in addressing nutrition), and vertical (across administrative levels from national to community) coherence in Rwanda. For this paper, we focus mostly on changes in commitment and coherence.
To analyze the data, an a priori coding list was developed based on the study instruments and the categories of political commitment and policy coherence. Transcripts were coded using this a priori coding list but allowing for emerging codes. Axial coding was then used to organize codes into conceptual themes. The conceptual themes identified during the coding process under political commitment and policy coherence were then mapped onto the different forms of political commitment and coherence to characterize changes that occurred in Rwanda and the challenges that remain. We also conducted a comparative analysis that used the two sets of reduced and non-reduced districts as the unit of analysis to identify similarities and differences in described themes between the two sets of districts (Miles et al., 2014). Because changes in undernutrition varied across the country, identifying if there were differences in governance between the districts that were able to register improvements and those that were less successful was important.
Lastly, theory-testing process tracing, which uses existing literature to construct hypothesis about mechanisms, was used to understand the causal mechanisms that led to changes in undernutrition in Rwanda (Bennett & George, 2005; Lapping et al., 2012; Beach, 2017). In process tracing, causal mechanisms are different from causality; they are interacting parts that work together or on each other to produce an outcome (Beach, 2017). In this study, process tracing was conducted using the document review and multiple sources of collected primary data to gain case-specific information and understanding of the processes that led to changes in nutrition in Rwanda. Process tracing focused on four steps: 1) the theoretical conceptualization of political commitment and policy coherence in nutrition, 2) what policy or strategy changes occurred in Rwanda, 3) what events and actions influenced these changes, and 4) how political commitment to and coherence in nutrition were operationalized.
3 Results
3.1 Policy environment
The progress observed in nutrition in Rwanda occurred within a policy environment that was adopting new agendas across many sectors, including those that affect nutrition. In 2000, Rwanda adopted Vision 2020, a long-term development strategy with specific objectives in agriculture and in human resource development through investments in health and education (Ministry of Finance & Economic Planning, 2000). The following year, Rwanda adopted its decentralization policy which focused on improving efficiency in the provision and delivery of public services to local communities. After Vision 2020 and the decentralization policy, Rwanda rolled out new policies and programs across the different sectors that affect nutrition, including in health, education where universal access to education was adopted, and in agriculture (Supplemental 1).
Outside of health, policies developed between 2000 and 2008 in education, agriculture, infrastructure, and gender and family promotion did not mention nutrition as a goal or issue of relevance. Around 2009, national nutrition summits began to be organized in the country, illustrating a shift towards making nutrition a priority according to respondents. Respondents reported that in 2009, the President of Rwanda made a public commitment through speech to fight malnutrition in Rwanda after a trip to health centers in Kirehe District, thereby increasing national level prioritization of nutrition. By 2012, an updated Vision 2020 policy recognized that improvements in the human resource development pillar could not be achieved without adequately addressing undernutrition (Republic of Rwanda, 2012). By 2013, sectoral policies or strategic plans in agriculture, social protection, education, and health increasingly reflected their role and potential contributions to improving nutrition. The infrastructure sector, however, which works on water and sanitation did not identify its sectoral contribution to nutrition until its 2016 National Water Supply Policy.
The country introduced a few national nutrition and nutrition-related programs such as Community-Based Nutrition in the health sector (1996), a One Cow per Family program in agriculture (2006), and a dietary supplementation program called One Cup of Milk per Child in the education sector (2010). As it signed on to the African Union’s Comprehensive Africa Agriculture Development Program in 2007, Rwanda initiated the national Crop Intensification Program with the goal to increase food production. Rwanda also established the national universal health insurance program Mutuelle de Santé which was first piloted in 1999 and became national policy in 2004 to improve access to health services.
3.2 Leadership and decentralization
After facing political instability and a genocide, respondents described that good leadership resulted in reconstruction, peace, and security, and the promotion of good governance and that these elements created an environment conducive to development. Respondents described the country’s leadership to be more “people-focused” and dedicated to developing the country and its citizens compared to the past.
Decentralization strengthened the quality of leadership in Rwanda, according to respondents, because the decentralized administrative structure improved interactions between communities and district leaders, who are mid-level actors. For example, district leaders acted on their increased awareness of and responsibilities for nutrition by transmitting nutrition messages and sensitizing communities to the importance of nutrition. Some respondents described that this communication by district leaders demonstrated nutrition prioritization at sub-national level and the leaders’ ability to communicate nutrition’s importance to further decentralized levels.
Rwanda used a yearly national performance contract initiative, called Imihigo, to increase accountability in the execution of planned programs and service delivery across sectors and districts. Although identified at the district level, Imihigos’ programs and services are in line with national priorities. Respondents believed that these performance-based contracts increased district leaders’ accountability to both the communities they served and national goals.
Lastly, national, and international development partners highlighted that a decentralized governance system facilitated the implementation of nutrition-related programs because of their ability to collaborate with mid-level actors at decentralized levels on program implementation and community participation.
“What allowed for these changes in nutrition is the decentralization of authorities. The authorities are close to us and if you have any problem, you can go to them.” – FGD participant from a non-reduced district
“Another thing that has changed is that local leaders are currently motivated to prevent malnutrition. In community meetings, villages chiefs discuss nutrition related issues with village members.” – Civil society organization respondent
3.3 Changes in political commitment to nutrition
Rwanda developed high political commitment to nutrition through rhetorical, institutional, operational, and financial commitment. Respondents described the emergence of nutrition champions, including the President, who publicly voiced through discourse and community visits the need to reduce undernutrition as a national development goal (Table 1). National nutrition summits in 2009 and 2011 strengthened rhetorical commitment to nutrition by bringing together diverse stakeholders to emphasize and discuss how to tackle burden and consequences of undernutrition in the country. Rwanda converted this political attention to nutrition into institutional commitment, according to respondents, by shifting from health-centered strategies towards more multisectoral strategies to address undernutrition and establishing platforms for implementation.
In 2010, the national Joint Action Plan to Eliminate Malnutrition (JAPEM) was established. JAPEM is a high-level joint plan, developed annually at the ministerial level, and used to implement and monitor nutrition-relevant activities across the different ministries that affect nutrition. The country further solidified its multisectoral strategies to address undernutrition through its second national nutrition policy, the National Food and Nutrition Policy 2013–2018 (NFNP), a multisectoral policy that specifically mapped out the roles and responsibilities of each of the ministries involved in nutrition. According to respondents, the NFNP increased these ministries’ ownership, responsibility, and participation in addressing undernutrition.
“This policy [NFNP] is multisectoral because it involves education, local government, agriculture etc. and this shows how nutrition has been given importance… Now nutrition is no longer only considered as responsibility of Ministry of Health but also of all other relevant institutions, whereby each institution has its own role in nutrition.” - National government respondent
The rhetorical and institutional commitment to nutrition at national level were translated at decentralized levels into operational commitment. For example, the increased nutrition awareness observed at national level was also observed in mid-level actors who received information on nutrition from civil societies. These mid-level actors used their positions to promote messages on preventing malnutrition and on the availability of relevant programs at decentralized levels. Through these messages, mid-level actors communicated on the roles that members of society, from leadership to program implementers and to citizens, should play to improve nutrition. Respondents believed that such messages increased ownership in nutrition at all administrative levels and in communities.
“The policy focuses on bringing together the different domains. It’s about knowing that it’s not any single sector’s job to fight undernutrition. This was the reason things failed in the past. But now, every sector is involved in nutrition starting from the national level down to our level here in the districts. Everyone who is engaged in the administration finds himself involved in responsibilities and this responsibility goes all the way down to the main implementer, who is the CHW [community health worker] in the community.” – Mid-level actor from reduced district
Another form of commitment to nutrition was the establishment of District Plans to Eliminate Malnutrition (DPEM) in 2010. DPEMs are annual plans that focus solely on nutrition; the plans describe nutrition and nutrition-related activities within each of Rwanda’s 30 districts. Every quarter, leaders from all the sectors involved in nutrition at the district level, including health, nutrition, social protection, education, agriculture, and gender, meet in DPEM committees to plan, monitor, and evaluate nutrition-related activities and progress in outcomes. The DPEM committee meetings involve development partners and staff from further decentralized units such as the sector and cell working on nutrition within a district. Respondents believed that DPEMs illustrated Rwanda’s institutional commitment to advance multisectoral action in nutrition through a decentralized platform that involved mid-level actors. The quality of implementation of DPEM committee meetings varied by study districts, however. For example, respondents from non-reduced districts tended to report that DPEM committee meetings were organized on an ad hoc basis with less participation and less integration of sectors such as agriculture. DPEM committees were intended to also be established at the sector, cell, and village levels, but they were only functional at the district level during our study.
Lastly, respondents described increased financial commitment to nutrition in Rwanda compared to the past based on the country’s increased investments and provision of nutrition and nutrition-related programs and services.
3.4 Changes in policy coherence
The development of the multisectoral NFNP and establishment of multisectoral platforms to facilitate coordination across sectors showed Rwanda’s commitment to addressing nutrition through multisectoral strategies. The operationalization of the policy and the established platforms illustrate how communication and actions across policies, institutions, and actors help to achieve coherence in addressing nutrition (Table 5).
3.4.1 Institutional coherence
At national level, communication and actions on nutrition across policies, institutions, and actors were first organized around the National Food and Nutrition Technical Working Group. Formed in 2013, the National Food and Nutrition Technical working Group brought together government, development partners, donors, civil society, and academic stakeholders working on nutrition. Respondents, mostly at the national level, found this working group beneficial because it created a space to coordinate and share information on program implementation, results, and experiences of different actors. Some respondents, however, saw this platform more as an information-sharing body than a multisectoral coordination body with convening power given the weak participation of people and sectors represented during meetings. In 2016, Rwanda established a National Food and Nutrition Coordination Secretariat (NFNCS), housed within the Ministry of Local Government, to coordinate all the ministries, partners, administrative levels, and different stakeholders involved in nutrition in Rwanda.Footnote 1 While some respondents perceived the NFNCS as a platform with stronger convening power to integrate nutrition in other ministries and to oversee monitoring and evaluation, others remained skeptical about placing a multisectoral coordination body in one ministry to coordinate other ministries. The NFNCS was in the early stages of implementation during our study, but respondents believed that it would be beneficial if implemented well.
3.4.2 Horizontal coherence
The NFNP brought together ministries that affect nutrition but with various individual goals and missions and assigned them responsibilities through nutrition-related actions. The perceived roles in nutrition by respondents in the involved sectors, mainly aligned with the described policy roles, showing sectoral acceptance of their roles and responsibilities in nutrition (Supplemental 2). Minor differences were observed, however, between the perceived and the policy-assigned role for actors in the agriculture sector especially at the national and district levels. For example, agriculture actors at the community level compared to their counterpart at the district and national level were more likely to describe their sector’s nutrition-related responsibilities.
Ministries, including agriculture, health, education, gender, and local government, collaborated to jointly implement national nutrition-specific, nutrition-sensitive, and nutrition-related programs. They also coordinated plans and activities through JAPEM at national level and DPEMs at decentralized levels. These platforms mirrored each other as they were both jointly designed yearly plans that described each sector’s nutrition-related activities. JAPEM and DPEMs provided a space for the different sectors to meet regularly to share information, assess implementation of activities and programs, and evaluate progress in implementation and outcomes. Because of these meetings, both platforms were credited for helping the sectors that did not traditionally see themselves as involved in nutrition to understand their sectoral contribution to nutrition especially at decentralized levels, thereby increasing acceptance of multisectoral nutrition strategies. District leaders described that DPEMs and their associated committee meetings allowed nutrition to be prioritized, thereby not fighting for attention from the many other issues that mid-level actors attended to.
“At the district level, we coordinate through DPEM because we discuss what is there and what is needed in nutrition… We will all hear about what is needed to help fight malnutrition and who will be in charge of what… Everyone [each sector] knows his responsibility in implementing the plan… In the past, certain sectors didn’t feel involved in nutrition, but it doesn’t mean that they were not involved. It was just not reflected in the policies. And it’s important to explain things to people and the more people meet, they start to feel that the problem [of nutrition] concerns them too.” – Mid-level actor from reduced district
3.4.3 Vertical coherence
Respondents described that the decentralized governance system in Rwanda facilitated vertical coherence because each administrative level had specific roles and responsibilities and staff responsible for nutrition, thereby improving government response to the issue. Each administrative level also answered to the level above it, which fostered incentives to collaborate vertically.
“There are institutions at national level from the ministry of health…and when you go at the district level, you find that authorities know about nutrition. At district level they do the follow-up and at the sector level there is a person in charge of nutrition. At the cell level there is also a person in charge of nutrition. At the village level, there is a person in charge of the well-being of people. Among people at the village level, there are community health workers who advise people and monitor children’s growth every month. This is all due to good, decentralized leadership.” -Mid-level actor from reduced district
Good relations and communication across administrative levels characterized the relationship between national and district levels, according to respondents. Respondents’ perspectives about these interactions differed, however, between reduced and non-reduced districts. District and community level respondents from reduced districts described communication and relationships with the national level and development partners more positively, stating that although the national government led policy development, they could share their experiences and provide feedback on policy and program decisions to the national level. Respondents from non-reduced districts tended to describe their relationship with the national level in neutral terms, focusing on the reporting relationship between the two levels. From the perspective of development partners implementing programs, mid-level actors facilitated the implementation of nutrition-relevant programs in communities because they provided local government buy-in and support during implementation. Development partners also reported that they participated in DPEM coordination meetings which strengthened their engagement in planning and addressing nutrition within the districts in which they worked.
“As the local administration and health structures are decentralized, it becomes easy for [our organization] to plan nutrition projects together with district leaders and to get the support of the district and community leaders while implementing those nutrition projects in districts. We are very close to them…ownership in nutrition and nutrition practices must exist from the high level to the village.”- Non-government national respondent
3.5 Challenges in political commitment and policy coherence are interlinked
Despite the positive changes in political commitment to- and policy coherence in- nutrition, respondents described remaining challenges. These challenges were often interlinked and affected program and policy implementation. Financial commitment to nutrition was a challenge mentioned by respondents at all administrative levels. Despite the increased provision of nutrition and nutrition-related programs and services in Rwanda, a sign of increased financial commitment to nutrition, respondents believed that resources remained insufficient. Insufficient funding affected the implementation of planned JAPEM and DPEM activities such as limiting participation of actors at the sub-district levels in DPEM meetings due to a lack of transportation resources and hindered cross-sector nutrition monitoring trips in communities by district leaders and program implementers. Insufficient funding also limited the human resources available to convene DPEMs. The convening role was held by vice mayors of social affairs, but they, along with many other respondents, described attending to their other responsibilities and coordinating DPEMS across sectors led to work overload. Work overload was also mentioned as a challenge at national level by the technical staff in charge of nutrition as they too had other responsibilities in addition to those related to nutrition. Respondents suggested that districts and ministries needed staff whose sole role would be to convene and coordinate DPEMs or focus solely on sectoral nutrition goals.
Overall, more respondents described challenges in coherence than in political commitment. In institutional coherence, there was a lack of distinction and overlap in function, role, and responsibilities of the coordination bodies at national level such as the National Food and Nutrition Technical Working Group and the NFNCS, which as one respondent stated could cause conflict and a lack of understanding of how these bodies should support each other in nutrition coordination. While JAPEM and DPEMs facilitated sectors coming together to coordinate nutrition-relevant activities, some respondents believed that sectors reported on their sector-specific activities within these platforms rather than holistically evaluating activities in an integrated manner to inform progress towards reducing undernutrition. The consequence of this challenge, which was reported more in non-reduced districts, was that although JAPEM and DPEMs were perceived to improve collaboration across sectors on nutrition, some sectors still worked in silos or did not sufficiently integrate nutrition. For example, in non-reduced districts, district leaders in agriculture were less likely to mention nutrition-sensitive responsibilities and also more likely to remark that their sector was not involved in the implementation of DPEMs because DPEMs are health-centered platforms. One recommendation made by respondents was to reinforce existing nutrition-related programs, especially those from the agriculture sector by making them more nutrition-sensitive and able to address the food security challenges faced by many vulnerable households in Rwanda.
“DPEM deals with health. It is in the social affairs department while agriculture is in the economic development department. People who work in the social affairs department like health or education sector are the ones involved in DPEM.” – Mid-level actor from non-reduced district
Mid-level actors also faced challenges that hindered the DPEM committees’ ability to monitor and evaluate district progress in implementation and outcomes. While awareness on nutrition, its multiple determinants, and the need for a multisectoral response had increased over the years, some of the mid-level actors in charge of DPEMs requested further training in both nutrition and monitoring and evaluation. These mid-level actors, also more from non-reduced districts, requested further training to improve technical skills in nutrition and monitoring and evaluation to better use existing monitoring tools, understand the relevance of the data available, and evaluate progress of the changes and challenges that remain in nutrition in their districts. Respondents both at national and district level also expressed that nutrition monitoring and evaluation in Rwanda could use an integrated framework that could help to evaluate nutrition-related indicators across the different involved sectors. Lastly, respondents at district and national level also noted that a problem in horizontal coherence was that DPEM committee meetings were not always conducted as planned in some districts.
Challenges in vertical coherence mainly regarded relationships between actors across administrative levels. Respondents, mainly from non-reduced districts reported that improvements were needed in communication and financial and input support from the national government. Mid-level actors and frontline workers also voiced challenges with their relationship with the NGOs and international organizations funding and implementing programs in communities. These respondents explained that the distribution of development partners working in nutrition across districts was uneven, reflecting poor coordination, and that it led to some districts benefiting more in program support, including technical and funding support for DPEM activities and evaluation. Some respondents perceived that development partners poorly implemented programs in their districts given the low program coverage, short program duration, or programs’ failure to address district population’s specific needs. Respondents also saw a duplication of efforts in the types of programs and geographic areas where partners implemented programs, which limited impact on nutrition outcomes in their districts.
4 Discussion
Despite many challenges over the last three decades, including civil conflict and the 1994 genocide against Tutsis, Rwanda has rebuilt itself, increased economic growth, and undergone significant changes that helped the country reduce child stunting and improve other nutritional outcomes. Rwanda established national goals and ambitions to turn itself into a middle-income country in a 20-year timeframe. The global nutrition community’s agreement on the causes and short-, mid-, and long-term consequences of undernutrition in the late 2000’s resonated with the political and policy context in Rwanda that was focused on human resource development to achieve its economic development objectives. After 2008, nutrition became a national priority in rhetoric but also in policy and institutionally as it was gradually integrated into different sectoral policies and in national economic development strategies.
Decentralization emerged as a theme. Respondents believed that the decentralization of the country’s administration improved accountability and as advocacy for nutrition at the different sub-national levels, thereby increasing nutrition awareness in the country. Such governance systems present an opportunity to integrate nutrition with other sectors at more local levels where implementation occurs (Thow et al., 2020). In the context of Rwanda, decentralization included the consolidation and reconfiguration of the administrative structure, which reduced the number of districts from over 150 to 30, and was a response to the needed reconciliation between the government and local communities after instability (Rwanda Ministry of Health, 2013). Some argue, however, that Rwanda’s governance system and consolidation of the administrative structure retains a lot of power at the central level, as has occurred for example with human resource for health management in Ghana (Sumah & Baatiema, 2019), thereby limiting the decentralization of power and responsibilities (Ansoms, 2009; Desrosiers & Thomson, 2011; Kauzya, 2007). The consolidation of the administrative structure as observed in Rwanda diverges, however, from other countries that tend to expand administrative levels in the decentralization process to gain political patronage (World Bank, 2015). One explanation for this consolidation is that, after experiencing extensive destruction during the genocide, Rwanda strongly sought an efficient system that could implement its agenda expeditiously to achieve the country’s pursuit of economic and social development (Chemouni, 2014).
Generating political commitment to nutrition at the national level and establishing platforms to increase policy coherence in nutrition do not necessarily result in changes in actions or outcomes on the ground. Effective engagement on nutrition at sub-national levels is important for generating and sustaining commitment and turning it into action in communities (Gillespie et al., 2013; Okeyo et al., 2021). We found that Rwanda, while already implementing a national decentralization policy, established platforms and joint nutrition plans to foster multisectoral collaboration on nutrition at decentralized levels in the early stages of their prioritization of nutrition. Developing this institutional political commitment to nutrition at decentralized levels was important for generating buy-in for nutrition across sectors at this level. In some countries, the lack of commitment as sub-national levels hindered actions. For example, in Bolivia, institutional platforms were established at decentralized levels to facilitate cross-sector collaborations in nutrition, but there was insufficient commitment and ownership from actors in sectors outside of health (Hoey & Pelletier, 2011). Despite initial high commitment at national level, these platforms became inactive. In Vietnam, decentralization led to a delegation of planning responsibilities for nutrition to the provincial levels, but the practice focused more on fiscal planning and did not generate ownership for nutrition among the planners (Lapping et al., 2014).
In the past, nutrition governance has often focused on governments establishing national multisectoral nutrition policies or national multisectoral coordination committees, but which political leaders sometimes established to satisfy external pressures (Field, 1987; Heaver, 2005; Mejía Acosta & Fanzo, 2012). Focusing on these national level decisions, however, can mask the lack of clear procedures for program and policy implementation which occurs at sub-national levels (Benson, 2007). Rwanda addressed this shortcoming by establishing multisectoral nutrition coordination platforms within its existing political and administrative structures through DPEMs whereby mid-level actors in all the country’s districts had the responsibility to plan, manage, implement, and monitor nutrition and nutrition-related activities in their jurisdiction. DPEMs address both multisectoral nutrition and decentralized nutrition program implementation. These platforms were a mechanism to increase engagement between actors with different sectoral interests and improve collaboration, which contributes to improvements in health outcomes (Okeyo et al., 2021; Schneider et al., 2020). Although the quality of implementation differed across districts in this study, with reduced districts reporting more optimal implementation of DPEMs compared to the districts with non-reduced stunting, DPEMs were a national response. In Peru and Zambia, establishing coordination platforms embedded within government structures and implemented by mid-level actors at decentralized levels increased the priority given to nutrition and how stakeholders worked collaboratively to address nutrition (Harris et al., 2017; Mejía Acosta & Haddad, 2014), but these decentralized platforms within government structures were localized and not streamlined in the countrywide institutional structure. In Peru, Ayacucho was highlighted as a success story for its high reductions of stunting prevalence and poverty rates and for being an area that had taken the initiative to establish an intersectoral committee to facilitate cross-sector collaboration (Mejía Acosta & Haddad, 2014). The intersectoral committee strengthened commitment to the national strategy and improved alignment with other sectoral programs. In Zambia, Mumbwa district became a model for other districts in the country after establishing a district nutrition coordination committee embedded in the existing government system with the support of the non-government organization Concern Worldwide (Harris et al., 2017). The coordination committee led to stronger networks between partners addressing nutrition in the district and helped change the framing of malnutrition as a food security issue alone.
Despite establishing platforms to increase cross-sector collaboration at different administrative levels, Rwanda still faced implementation challenges related to resources and capacity, elements of the enabling environment (Gillespie et al., 2013). Implementing multisectoral nutrition strategies involves organizational complexities to coordinate activities and manage policy trade-offs across sectors with different institutional goals (Field, 1987; Nilsson & Weitz, 2019). These complexities place increased workload on the actors and platforms in charge of this coordination, which was reflected at both the national and decentralized levels in Rwanda. Technical staff in the ministries involved in nutrition at the national level and mid-level actors discussed challenges they faced regarding nutrition technical capacity and heavy workloads related to their respective institutional and nutrition responsibilities. At decentralized levels, where there is often the risk of having “underprepared middle level management” to plan, budget, and advocate for the needs of decentralized levels, giving nutrition responsibilities to mid-level actors from different sectors requires skills in not just planning and budgeting for nutrition but also technical and monitoring and evaluation skills for nutrition (Men et al., 2005). In Rwanda, some mid-level actors explicitly requested this further training to help them understand nutrition-related data, monitor progress, and to inform decision-making for their district’s context-specific needs. To truly integrate nutrition in different sectors and improve the capacity for decentralized leadership in nutrition will require investments in technical trainings and on-going trainings on nutrition for the mid-level actors from various sectors, how their activities complement each other to address nutrition, and how to plan for and monitor change and progress in the communities within their districts. Such investments in these mid-level actors who provide leadership at decentralized levels may help to improve their role in assessing the suitability of existing programs, new programs, their design, targeting, and coverage within their districts. It may also help nutrition actors better manage emerging issues in nutrition such as the double-burden of malnutrition. Challenges with funding and resources, which are often reported in many country case studies, were also observed in Rwanda. These challenges affected the implementation of the procedures meant to improve coherence in nutrition-related policy and programing (Gillespie & van den Bold, 2017). Resources were perceived to have increased over the years, but they continued to constrain the implementation of activities and overall program coverage. Financial constraints limited the human resources available to effectively implement the policy leading to work overload for implementers. Work overload was especially highlighted for the mid-level actors who lead DPEMs along with their existing responsibilities. Due to these competing time demands, many of these actors felt unable to allocate the time needed to lead and coordinate DPEMs optimally. Increasing staff or hiring nutrition conveners who specifically focus on coordinating nutrition at the sub-national levels could increase the implementation and effectiveness of DPEMs. One limitation of this study was that we were not able to further investigate financial commitments to nutrition, one of the biggest identified challenges.
Strengths of this study include its sampling which included districts across the five provinces of Rwanda; this sampling allowed for the perspectives of respondents form different contexts across the country. This study provides an understanding of the sub-national context and the perspectives of the mid-level actors translating and implementing nutrition policies and programs. A limitation is that we did not assess the coverage of nutrition and nutrition-related programs which could have provided more information on the translation of actions on the ground.
This study provides information on what countries facing similar challenges as Rwanda can do to achieve progress in reducing undernutrition and provides understanding of the role of mid-level actors in translating and implementing nutrition policies and the challenges they face. Political commitment to nutrition and the establishment of platforms to promote cross-sector collaboration for the implementation of multisectoral nutrition strategies were important drivers and sustainers of changes in child nutrition in Rwanda. These efforts were developed and promoted both at national and decentralized levels and focused on getting mid-level actors and frontline workers engaged in nutrition. Rwanda used its existing political and administrative structures to prioritize local response and involvement in nutrition. Sustaining these efforts and the improvements observed in nutrition will require increased resources for program implementation, human resources, and technical trainings in nutrition for the government stakeholders with responsibilities in nutrition. Although coordination platforms have been established across the country to facilitate coherence across sectors, these too need to be strengthened, especially in districts where implementation was weak.
Availability of data and material
The data that support the findings of this study are available from the corresponding author, [EI], upon reasonable request. The data are not publicly available due to the privacy of research participants.
Code availability
Not applicable.
Notes
After our data collection, the National Food and Nutrition Secretariat moved from the Ministry of Local Government and was integrated with the National Early Childhood Development Program (NECDP) in 2018 and in 2020 into the National Child Development Agency within the Ministry of Gender and Family Promotion.
References
Ansoms, A. (2009). Re-engineering rural society: The visions and ambitions of the Rwandan elite. African Affairs, 108(431), 289–309. https://doi.org/10.1093/afraf/adp001
Baker, P., Hawkes, C., Wingrove, K., Demaio, A. R., Parkhurst, J., Thow, A. M., & Walls, H. (2018). What drives political commitment for nutrition? A review and framework synthesis to inform the United Nations Decade of Action on Nutrition. BMJ Global Health, 3(1), e000485. https://doi.org/10.1136/bmjgh-2017-000485
Beach, D. (2017). Process-Tracing Methods in Social Science (pp. 1–28). Oxford Research Encyclopedia of Politics. https://doi.org/10.1093/acrefore/9780190228637.013.176
Bennett, A., & George, A. L. (2005). Case studies and theory development in the social sciences. MIT Press.
Benson, T. (2007). Cross-sectoral coordination failure: How significant a constraint in national efforts to tackle malnutrition in Africa? Food and Nutrition Bulletin, 28(2), 323–330.
Black, R. E., Victora, C. G., Walker, S. P., Bhutta, Z. A., Christian, P., De Onis, M., & Uauy, R. (2013). Maternal and child undernutrition and overweight in low-income and middle-income countries. The Lancet, 382(9890), 427–451. https://doi.org/10.1016/S0140-6736(13)60937-X
Caulfield, L. E., De Onis, M., Blössner, M., & Black, R. E. (2004). Undernutrition as an underlying cause of child deaths associated with diarrhea pneumonia malaria and measles. The American Journal of Clinical Nutrition, 80(1), 193–198. https://doi.org/10.1093/ajcn/80.1.193
Chemouni, B. (2014). Explaining the design of the Rwandan decentralization: Elite vulnerability and the territorial repartition of power. Journal of Eastern African Studies, 8(2), 246–262.
Desrosiers, M. E., & Thomson, S. (2011). Rhetorical legacies of leadership: Projections of “benevolent leadership” in pre- and post-genocide Rwanda. Journal of Modern African Studies, 49(3), 429–453. https://doi.org/10.1017/S0022278X11000279
Development Initiatives. (2017). Global Nutrition Report 2017: Nourishing the SDGs. UK: Bristol. https://doi.org/10.1891/1058-1243.21.1.9.
Field, J. O. (1987). Multisectoral nutrition planning: A post-mortem. Computer and Operations Research, 2(2), 115–119. https://doi.org/10.1080/13504850500401858
Garrett, J., & Natalicchio, M. (2011). Working Multisectorally in Nutrition: Principles practices and case studies. International Food Policy Research Institute.
Gillespie, S. (2015). Stories of Change in Nutrition: A Tool Pool. IFPRI.
Gillespie, S., & van den Bold, M. (2017). Stories of Change in nutrition: An overview. Global Food Security, 13, 1–11. https://doi.org/10.1016/j.gfs.2017.02.004
Gillespie, S., Haddad, L., Mannar, V., Menon, P., & Nisbett, N. (2013). The politics of reducing malnutrition: Building commitment and accelerating progress. The Lancet, 382(9891), 552–569. https://doi.org/10.1016/S0140-6736(13)60842-9
Harris, J., Drimie, S., Roopnaraine, T., & Covic, N. (2017). From coherence towards commitment: Changes and challenges in Zambia’s nutrition policy environment. Global Food Security, 13, 49–56. https://doi.org/10.1016/j.gfs.2017.02.006
Heaver, R. (2005). Strengthening Country Commitment to Human Development. World Bank Publications. https://doi.org/10.1596/0-8213-6037-X
Hoey, L., & Pelletier, D. L. (2011). Bolivia’s multisectoral Zero Malnutrition Program: Insights on commitment collaboration and capacities. Food and Nutrition Bulletin, 32(2), 70–81. https://doi.org/10.1177/15648265110322S204
Kampman, H., Zongrone, A., Rawat, R., & Becquey, E. (2017). How Senegal created an enabling environment for nutrition: A story of change. Global Food Security, 13, 57–65. https://doi.org/10.1016/j.gfs.2017.02.005
Kauzya, J. (2007). Political Decentralization in Africa: Experiences of Uganda Rwanda and South Africa (pp. 75–91). Brookings Institution Press Discussion Paper.
Kennedy, E., Tessema, M., Hailu, T., Zerfu, D., Belay, A., Ayana, G., & van Wassenhove, J. (2015). Multisector nutrition program governance and implementation in Ethiopia: Opportunities and challenges. Food and Nutrition Bulletin, 36(4), 534–548. https://doi.org/10.1177/0379572115611768
Lapping, K., Frongillo, E. A., Nguyen, P. H., Coates, J., & Webb, P. (2014). Organizational factors planning capacity and integration challenges constrain provincial planning processes for nutrition in decentralizing Vietnam. Food and Nutrition Bulletin, 35(3), 382–391.
Lapping, K., Frongillo, E. A., Studdert, L. J., Menon, P., Coates, J., & Webb, P. (2012). Prospective analysis of the development of the national nutrition agenda in Vietnam from 2006 to 2008. Health Policy and Planning, 27(1), 32–41. https://doi.org/10.1093/heapol/czr013
Lintelo, D. J. H. T. E., & Lakshman, R. W. D. (2015). Equate and Conflate: Political Commitment to Hunger and Undernutrition Reduction in Five High-Burden Countries. World Development, 76, 280–292. https://doi.org/10.1016/j.worlddev.2015.07.013
Mejía Acosta, A., & Fanzo, J. (2012). Fighting Maternal and Child Malnutrition: Analyzing the political and institutional determinants of delivering a national multisectoral response in six countries (pp. 1–39). Brighton: IDS A synthesis.
Mejía Acosta, A., & Haddad, L. (2014). The politics of success in the fight against malnutrition in Peru. Food Policy, 44, 26–35. https://doi.org/10.1016/j.foodpol.2013.10.009
Men, B., Grundy, J., Cane, J., Rasmey, L. C., Sim An, N., Soeung, S. C., ... & Biggs, B. A. (2005). Key issues relating to decentralization at the provincial level of health management in Cambodia. The International Journal of Health Planning and Management, 20(1), 3–19.
Menon, P., Frongillo, E. A., Pelletier, D. L., Stoltzfus, R. J., Ahmed, A. M. S., & Ahmed, T. (2011). Assessment of epidemiologic operational and sociopolitical domains for mainstreaming nutrition. Food and Nutrition Bulletin, 32(2), 105–114. https://doi.org/10.1177/15648265110322S207
Miles, M. B., Huberman, A. M., & Saldaña, J. (2014). Qualitative data analysis: A methods sourcebook. Sage Publications.
Ministry of Finance and Economic Planning. (2000). Republic of Rwanda Vision 2020, (July), 1–29. Retrieved from http://www.gesci.org/assets/files/Rwanda_Vision_2020.pdf
Ministry of Gender and Family Promotion. (2018). Rwanda country strategic review of food and nutrition security. Kigali, Rwanda. Retrieved from https://docs.wfp.org/api/documents/WFP-0000074047/download/
Ministry of Local Government. (2012). National decentralization policy revised. Kigali, Rwanda. Retrieved from http://www.minaloc.gov.rw. Accessed 17 February 2019.
National Institute of Statistics of Rwanda, & Ministry of Finance and Economic Planning. (2014). Rwanda fourth population and housing census. Final results: Publication tables. Retrieved from http://microdata.statistics.gov.rw/index.php/catalog/65/related_materials
NFNP. (2013). National Food and Nutrition Policy 2013-2018. Kigali, Rwanda.
Nilsson, M., & Weitz, N. (2019). Governing trade-offs and building coherence in policy-making for the 2030 agenda. Politics and Governance, 7(4), 254–263.
NISR, NISR MOH Rwanda, & ICF International. (2015). Rwanda demographic and health survey 2014-15. Rockville, Maryland, USA: NISR, MOH, and ICF International.
Okeyo, I., Lehmann, U., & Schneider, H. (2021). Policy adoption and the implementation woes of the intersectoral first 1000 days of childhood initiative in the Western Cape province of South Africa. International Journal of Health Policy and Management, 10(7), 364–375.
Pelletier, D. L., Frongillo, E. A., Gervais, S., Hoey, L., Menon, P., Ngo, T., & Ahmed, T. (2012). Nutrition agenda setting, policy formulation and implementation: Lessons from the Mainstreaming Nutrition Initiative. Health Policy and Planning, 27(1), 19–31. https://doi.org/10.1093/heapol/czr011
Republic of Rwanda. (2012). Rwanda vision 2020 revised 2012. Retrieved from https://www.mindbank.info/item/6266
Republic of Rwanda. (2021). Republic of Rwanda. Retrieved April 13, 2021, from https://www.gov.rw/about
RGB. (2018). Rwanda governance review good governance and decentralization in Rwanda (vol. VI). Kigali, Rwanda.
Ruel, M. T., & Alderman, H. (2013). Nutrition-sensitive interventions and programmes: How can they help to accelerate progress in improving maternal and child nutrition? The Lancet, 382(9891), 536–551. https://doi.org/10.1016/S0140-6736(13)60843-0
Rwanda Ministry of Health. (2013). National community health strategic plan 2013-2018. Kigali, Rwanda
Schneider, H., George, A., Mukinda, F., & Tabana, H. (2020). District governance and improved maternal, neonatal and child health in South Africa: pathways of change. Health Systems & Reform, 6(1), e1669943.
Sumah, A. M., & Baatiema, L. (2019). Decentralisation and management of human resource for health in the health system of Ghana: A decision space analysis. International Journal of Health Policy and Management, 8(1), 28.
Thow, A. M., Apprey, C., Winters, J., Stellmach, D., Alders, R., Aduku, L. N. E., & Annan, R. A. (2020). Understanding the impact of historical policy legacies on nutrition policy space: Economic policy agendas and current food policy paradigms in Ghana. International Journal of Health Policy and Management, 10(12), 909–922.
Victora, C. G., Adair, L., Fall, C., Hallal, P. C., Martorell, R., Richter, L., & Sachdev, H. S. (2008). Maternal and child undernutrition: Consequences for adult health and human capital. The Lancet, 371(9609), 340–357. https://doi.org/10.1016/S0140-6736(07)61692-4
Warren, A. M., & Frongillo, E. A. (2017). Mid-level actors and their operating environments for implementing nutrition-sensitive programming in Ethiopia. Global Food Security, 13, 66–73. https://doi.org/10.1016/j.gfs.2017.01.010
WHO, UNICEF, & World Bank. (2019). Levels and trends in child malnutrition: key findings. 2019 Edition of the Joint Child Malnutrition Estimates. Geneva: World Health Organization.
World Bank. (2015). Project performance assessment report: Republic of Rwanda decentralization and community development project. IEG Public Sector Evaluation. Retrieved from https://ieg.worldbankgroup.org/sites/default/files/Data/reports/Rwanda_Decentralization_Comm_Devt_PPAR.pdf
Funding
This study was funded by the Ministry of Foreign Affairs of Kingdom of Netherlands through the Voice for Change Partnership project (V4CP) implemented by a consortium led by SNV Netherlands Development Organization together with the International Food Policy Research Institute (IFPRI) and the CGIAR Research Program on Agriculture for Nutrition and Health (A4NH) led by IFPRI.
Author information
Authors and Affiliations
Contributions
EI, DKO, and EAF conceptualized the study. Material preparation, data collection, and analysis were performed by EI with the guidance of DKO and EAF. The first draft of the manuscript was written by EI and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
This study received approval from the institutional review boards of the University of South Carolina, the International Food Policy Research Institute, and the Rwanda National Ethics Committee.
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Consent for publication
Not applicable.
Conflicts of interest or financial interests
The authors have no relevant financial or non-financial interests to disclose.
Additional information
The information of this document expresses Dr. Simeon Nanama’s personal views and opinions and does not necessarily represent UNICEF’s position.
This article belongs to the Topical Collection: Stories of Change in Nutrition: Lessons from Africa and Asia
Guest Editors: Stuart Gillespie, Nicholas Nisbett, Mara van de Bold, Jody Harris
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Iruhiriye, E., Olney, D.K., Frongillo, E.A. et al. Translation of policy for reducing undernutrition from national to sub-national levels in Rwanda. Food Sec. 14, 977–993 (2022). https://doi.org/10.1007/s12571-022-01271-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12571-022-01271-2