
Abstract
This paper investigated the determinants of unhealthy BMI categories, namely underweight, overweight, and obesity, for urban and rural women of childbearing age in Bangladesh. Multilevel nested logistic models were estimated using data from multiple waves (2004–18) of the Demographic and Health Surveys of Bangladesh. After controlling for community and regional effects, the underweight status showed an inverse relationship with years of education for urban and rural women. Conversely, the fitted model estimates revealed a positive association between overweight risk and education for both urban and rural women populations. However, the association between obesity and education was significant for only urban women. Employment status appeared to be negatively associated with the risks of being overweight and obese in both population groups. Moreover, the women were found less likely to be underweight and more likely to be overweight and obese when their household socio-economic status improved. Study findings have the potential to inform a wide range of interventions, policies and programs that simultaneously address the adverse consequences of underweight, overweight, and/obese population health conditions in rural and urban Bangladesh.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The rising prevalence of unhealthy body mass index (BMI) since 1990 is a major population health concern in most of the world countries. Therefore, the double burden of malnutrition, defined as the simultaneous manifestation of both undernutrition and overweight and obesity, continues to pose a continuing major global public health and economics challenge (Tumas & López, 2024). Almost one-third of the global population experiences some form of extreme malnutrition (WHO, 2016a) with more than 30% overweight or obese, and over 600 million underweight adults (WHO, 2016b). The latest estimates show that two-thirds of the global obese population is women residing in developing countries, and their proportion is expected to rise in the future (IHME, 2017). Previous work found unhealthy BMI populations to be predisposed to a host of communicable and non-communicable diseases including COVID-19, cancer, heart disease, mental health disorders, and diabetes (Cammock et al., 2021). Additionally, overweight, and obese women are more prone to many pregnancy-related complications, such as preeclampsia, gestational diabetes and hypertension, postpartum hemorrhage, premature and preterm birth, and perinatal mortality for the newborn (Yan, 2015). Nutritional deficiencies leading to the underweight condition have also adverse consequences for women and children during pregnancy and after delivery (Mishra & Bera, 2023).
Bangladesh, a low-middle income country, has been struggling with the double burden of malnutrition (Biswas et al., 2021). Bangladesh has one of the highest global prevalence of underweight adults. The country’s prevalence of underweight women of childbearing age declined from 52 to 12% while the prevalence of overweight and obesity increased from 3 to 32% from 1996 to 2018 (DHS, 2017–2018; NIPORT, 2018). This is a trend common in low-middle income countries (LMICs) undergoing nutritional transition (see, for example, Mukanu et al., 2023). Moreover, there are disparities in BMI and nutritional status between rural and urban women, as found in many countries. For the current study data (see, Table 5) the rural underweight population proportion (13%) is higher than in urban areas (9%). In contrast, the population proportion of obesity and overweight women is higher in urban (43%) than rural (28%) areas. Rural areas tend to face more challenges in access to a wide range of nutritious foods. Hossain et al. (2023) attributes the higher prevalence of undernutrition in rural than urban Bangladesh mostly to the differential endowment effect. On the other hand, urban residents tend to have wider access to food varieties, including processed and high-calorie options, which raises their risks for overnutrition and obesity (Govindaraj et al., 2017).
This study investigates the socio-economic determinants of unhealthy BMI categories; namely, underweight, overweight and obesity; separately, for childbearing age women in urban and rural Bangladesh using Bangladesh Demographic and Health Surveys (BDHS). Examining the BMI status in this population is crucial for several reasons. First, BMI is a significant indicator of maternal health outcome. Women with underweight or overweight BMI status tend to face increased pregnancy health risks, including complications during labor, preterm birth, and low birth weight (Schneider et al., 2020). Second, Maternal nutrition directly impacts fetal development health. That is, an inadequate nutrition of the underweight expectant mother can portend poor fetal growth, while overweight or obese mothers may face greater risk of gestational diabetes and other complications (Prioreschi et al., 2021). Third, women’s health before and during pregnancy can have long-term consequences for the physical, cognitive, and health development of children (Costa-Font & Jofre-Bonet, 2020). Finally, from a health equity standpoint, evaluating BMI in women of childbearing age residing in rural compared with urban areas is capable of shedding lights on potential policies for addressing health outcome disparities and promoting health equity (Forster et al., 2020).
Country background
Bangladesh is a lower-middle-income country with a population of 171 million and is one of the most populated countries in the world. The country has an overall literacy rate of 75% and the labor force participation stands at 58% (ADB, 2021) and has made noticeable progress in the past 20 years on maternal health. The maternal mortality ratio declined from 550 deaths per 100,000 live births in 1990 to 156 in 2022. Women access to healthcare services remains a big concern in the country, particularly in rural areas where poverty, limited education, and cultural norms tend to hinder women from seeking or receiving adequate healthcare services. Currently, 67% of women aged 15–49 lack adequate access to health care services (Sen et al., 2023).
Urban–rural disparities in Bangladesh are evident across various dimensions, including education, socio-economic indicators, healthcare access, education, and infrastructure. More specifically, urban areas fare better than their rural counterpart in compulsory (secondary) education completion (25 vs. 14%). Surprisingly, rural areas fare better than the urban areas in employment rate (51 vs. 40%) and access to borrowed funds for income generating activities from financial organizations. Finally, rural women have limited access to healthcare due to supply-side (e.g., inadequate health services facilities and healthcare manpower shortages, etc.) and demand-side (e.g., socio-cultural differences in health-seeking behaviors and services utilization) factors. Bangladesh is currently experiencing a double burden of malnutrition in nutritional status (Mahmud et al., 2024). Appendix Table 4 provides some key statistics on socio-economic indicators between rural and urban Bangladesh.
Methods
Data
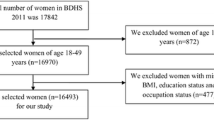
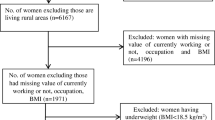
We used data from the latest five rounds (2004, 2007, 2011, 2014, and 2018) of the BDHS. All the five survey rounds are based on the two-stage stratified sampling technique. The sampling process involves stratifying the sample into regions that are further divided into urban and rural areas. For each survey, the enumeration areas (EAs) or communities and the primary sampling units (PSU) are selected in the first stage by employing the probability proportional to the size sampling technique. All clusters are approximately equal geographical area. A household listing prepared for all the selected clusters serves as a sampling framework for identifying households in the second stage. Using an equal probability systematic sampling technique, 30 households, on average, were drawn from each selected community (DHS, 2017–2018; NIPORT, 2018). We excluded pregnant women and those who gave birth within the 2 months preceding the surveyFootnote 1 to avoid selection bias in the estimation sample. Women aged 10–14 years were excluded from the study to be consistent across all the five survey rounds. The final estimation sample contained 63,818 women aged 15–49 (22,571 urban and 41,247 rural).
Variables
The BDHS computes BMI using reported data on the height and weight of individuals by dividing the weight in kilograms by the square of the height in meters. We classify the respondents following the definition of the World Health Organization (WHO) as being underweight \(({\text{BMI}} < 18.5{\text{ kg}}/{\text{m}}^{2} ),\) normal weight (\(18.5{ } \le {\text{ BMI }} \le { }24.9{\text{ kg}}/{\text{m}}^{2}\)), overweight (\(25{ } \le {\text{ BMI }} \le { }29.99{\text{ kg}}/{\text{m}}^{2}\)), and obese (\({\text{BMI }} \ge { }30{\text{ kg}}/{\text{m}}^{2}\)). Asians tend to have higher rates of cardiovascular diseases and diabetes even at lower BMI levels, and the recommended overweight and obesity cutoffs for Asians by WHO are \(23 - 27.49\) \({\text{kg}}/{\text{m}}^{2}\), and \(\ge 27.5\) \({\text{kg}}/{\text{m}}^{2}\), respectively.Footnote 2 Following Khudri et al. (2023), we consider three key economic determinants in our empirical models: women’s years of education, employment status, and household socio-economic status (SES hereafter). The unavailability of household income or consumption expenditures in the BDHS data was overcome using the wealth index variable generated from household assets and housing characteristics (Filmer & Pritchett, 2001).Footnote 3 Household SES was measured based on the wealth index and classified into five groups: poorest, poorer, middle, richer, and richest. Finally, we controlled for women’s age, age squared, current marital status, age at first birth, total number of children ever born, partner’s education (in years), partner’s occupation, media access, and household size in our empirical models.
Statistical analysis
We used two-level and three-level multivariate nested logistic models that account for the hierarchical data structure of the BDHS and estimated random effects along with fixed effects of determinants of unhealthy BMI categories. We began by estimating the following two-level model allowing for random effects due to community:
where \(P_{ijt}^{N} = P(Y_{ijt}^{N} = 1|X, u_{j} )\) is the probability that individual I nested within community j at time t is suffering from a malnutrition indicator N (underweight, overweight and obesity). The conditional distribution of the response \(Y_{ijt}^{N}\) is assumed to be Bernoulli. The vector \(X_{ijt}\) is the vector of covariates, \(\beta\) is the vector of fixed effects regression coefficients, R indicates a vector of region (location) dummies and T denotes a vector of year dummy variables that capture trend effects with the 2004 round as the base (Headey et al., 2015). The community-specific component, \(u_{j}\), a community random effect, presumably follows a normal distribution with mean zero and variance \(\sigma_{{u_{j} }}^{2}\). The significance of \(\sigma_{{u_{j} }}^{2}\) leads to evidence of community effects in the model, implying that two individuals from different communities with the same set of characteristics yield different responses to their malnutrition status.
Next, we extended estimation to the following three-level model allowing for the random effects due to the region and the community nested within the region:
where \(P_{ijkt}^{N} = P(Y_{ijkt}^{N} = 1|X, u_{k} , v_{j\left( k \right)} ,T_{t} )\) is the probability that individual i within community j nested within region k at time t is suffering from a malnutrition indicator N (underweight, overweight, and obesity). The region-specific component \(u_{k}\), a region random effect, is assumed to follow a normal distribution with mean zero and variance \(\sigma_{{u_{k} }}^{2}\). Similarly, the community-specific component nested within the region \(v_{j\left( k \right)}\), a community random effect, presumably follows a normal distribution with mean zero and variance \(\sigma_{{v_{j\left( k \right)} }}^{2}\). The statistical significance of \(\sigma_{u}^{2}\) and \(\sigma_{{v_{j\left( k \right)} }}^{2}\) would suggest evidence of community and region effects. We estimated all the models with adjustments for the sampling weight using STATA 17 (StataCorp, 2021).
Results
Descriptive statistics
Figure 1 shows that the average BMI, and the proportions of overweight and obesity among women gradually increased while the proportion of underweight consistently dropped in urban and rural areas over 2004–2018. There is a consistently higher BMI in urban women compared to their rural counterparts. The prevalence of underweight was substantially higher among rural women than urban ones. In contrast, we noticed the opposite scenario in the proportions of overweight and obese women for both groups.

Average BMI, and the prevalence of underweight, overweight, and obesity in Bangladesh over 2004–2018
Appendix Table 5 presents the descriptive statistics of economic and demographic characteristics and unhealthy BMI categories by residence. The average years of education for urban and rural women were about six and four years, respectively. There were nearly a 40% and 77% increase in the average years of education for urban and rural women during the study period. Compared to the baseline survey, there was a 14-percentage point increase in the percentage of employed urban women at the endline. Unlike urban households, the socio-economic status of rural households appeared to deteriorate during the study period. The average BMI of the sampled women for urban and rural areas were 21.52 kg/m2 and 19.76 kg/m2 at the baseline and they increased to 24.44 kg/m2 and 22.85 kg/m2, respectively. The prevalence of underweight among urban women fell about two-thirds during the study period, while the proportion of overweight more than doubled. There is a threefold rise in obesity. The prevalence of underweight among rural women dropped by about 24-percentage points between 2004 and 2018. On the other hand, the prevalence of overweight increased by about 18-percentage points, and obesity increased by about 4.22 percentage points.
The Mann–Whitney U test result suggested a statistically significant difference in median BMI, indicating that the distribution of BMI is different between urban and rural women. Pooled data regression test results further suggested that the coefficients are statistically significantly different for urban and rural subsamples for all three unhealthy BMI categories.Footnote 4 This implied the need to separately estimate determinants of unhealthy BMI categories for each cohort.
Appendix Table 6 provides the descriptive statistics (mean or %) and bivariate analysis results of nutritional status by characteristics for urban (Panel A) and rural (Panel B) samples. ANOVA results suggest a significant difference in the mean value of each continuous predictor across nutritional status. Additionally, we detected evidence of a significant association between each categorical predictor and nutritional status for both samples. The average year of education was higher for overweight and obese women than for underweight women in both urban and rural samples. Excluding the standard category, unemployed urban women appeared more overweight, while we found unemployed rural women more underweight. Conversely, among employed women, we observed more overweight than underweight in both samples. Women from poor and affluent households, regardless of the area of residence, tend to be more underweight and overweight, respectively.
Determinants of underweight
Table 1 reports the marginal effects for two-level and three-level models evaluating the economic determinants of underweight, separately for urban and rural populations of childbearing age women. We identified statistically significant community and region random effects in both samples from three-level model estimations. Discussions henceforth focus on the estimation results of the three-level model.
There is a statistically significant negative association between education and underweight in both samples, as reported in columns (1) to (4).Footnote 5 Column (2) indicates that urban women who received an additional year of education are 0.6 percentage point less likely to be underweight. The marginal effect of education for rural women is slightly lower compared to that for urban women. An extra year of education was associated with a 0.5 percentage point reduction in rural women’s risk of being underweight.Footnote 6 An insignificant inverse relationship between women’s underweight condition and employment status was observed for both groups.
The association of SES with underweight was negative across all subgroups.Footnote 7 The estimated marginal effect dropped from higher to lower SES for both rural and urban samples. Column (2) shows that urban women from the richest households had 13.2 percentage points lower risks of being underweight than their poorest peers. Column (4) reports that women from the richest households in rural areas had 18.4 percentage points lower risk of being underweight than their poorest peers. Similarly, women from middle-class households were about 6.2 percentage points less likely to be underweight than their poorest peers in urban areas and 7.9 percentage points less likely to be underweight in rural areas. The marginal effects of each SES category for rural women are higher than for the urban women. The significance of year dummy variables suggested that women’s risk of being underweight gradually decreased significantly within the study period.
Determinants of overweight
Table 2 presents results for the overweight indicator separately for urban and rural samples. Unlike in the estimated underweight models, we found women’s education to be significantly positively related to their risk of being overweight in both samples, as seen in Columns (1) to (4). Column (2) indicates that urban women with one more year of education were 0.5 percentage point more likely to be overweight. In contrast, an additional year of education for rural women was associated with 0.3 percentage point greater risk of being overweight.Footnote 8 Column (2) shows that employed urban women were 2.9 percentage point less likely to be overweight than their unemployed peers. The estimates for rural women dropped to 0.9 percentage points, implying that employed rural women were 0.9 percentage point less likely to be overweight than their unemployed peers (Column 4). We found that the positive association between SES and overweight appears to be mostly concentrated among women from middle-class and rich households in the urban sample.Footnote 9 However, for the rural sample, the associations appear to be significantly positive across all subgroups. The significant trend effects suggested that women’s risk of being overweight increased over time.
Determinants of obesity
Table 3 provides the marginal effects of obesity for urban and rural subsamples. Information in column (2) indicates that urban women who received one more year of education were 0.1 percentage points more likely to be obese than their non-obese counterparts. A highly significant negative relationship exists between obesity and employment status only in the urban sample, while it is marginally significant (at a 10% level) for the rural sample. Column (2) reports that employed women in the urban area were 2 percentage points less likely to be obese while the employed women in the rural area were only 0.1 percentage point less likely to be obese compared to their unemployed peers, as reported in Column 4. Our results indicated a much stronger association between obesity and SES in urban areas across all SES categories.Footnote 10 The positive association between SES and obesity is mainly concentrated among women from middle-class and rich households for the urban sample.
However, for the rural sample, the associations are significantly positive across the subgroups. The year dummy variables suggested that women’s risk of being obese gradually rose significantly over the study period.
Robustness checks
To supplement and validate our main set of results, we conducted several heterogeneity analyses across studied subsamples stratified by age group and marital status. In addition, we indirectly tested the robustness of our baseline estimates against susceptibility to endogeneity by eliminating fertility, demographic variables, and partner characteristics on the grounds that these might be potentially endogenous (Headey et al., 2015). Though marginal effects estimates vary to some extent, all our subsamples and specifications hold the robustness of our estimates in terms of direction (sign) and significance. Results are available upon request. The multinomial logistic regressions results did not differ significantly from those in Tables 1, 2, and 3.Footnote 11 Finally, we performed sensitivity analyses for each outcome using normal weight as a reference category and excluding the other two classes from the dataset. The results are reported in Appendix Tables 11, 12, 14. Additionally, we estimated the models for overweight and obesity outcomes using the recommended cutoffs for Asians as mentioned in Sect. “Variables”. These results are in Appendix Tables 13 and 15. All these findings are consistent with our primary results reported in Tables 1, 2, and 3.
Discussion and conclusion
This paper provided robust evidence on the determinants of unhealthy BMI categories (underweight, overweight and obesity) among women of childbearing age in urban and rural Bangladesh. We analyzed multiple waves of the nationally representative BDHS datasets and executed multilevel nested logistic estimation methods. The main variables of interest were three crucial economic determinants of unhealthy BMI: education, employment status, and SES. Our estimation method, not previously used in this line of enquiry, enabled the detection of community and regional effects. The results suggested existence of substantial differences in the association between unhealthy BMI categories and their determinants; namely, education, employment, and SES across rural and urban areas of Bangladesh.
First, our estimates showed that women’s education decreased the likelihood of being underweight and increases the odds of being overweight in urban and rural settings. Education is often correlated with socio-economic status (Mizala et al., 2007). Higher levels of education are generally associated with better economic opportunities and access to resources. Women with higher education levels may have better access to nutritious food, healthcare, and a generally higher standard of living, reducing the likelihood of being underweight (Conti et al., 2010). Our findings on the higher risk of obesity for urban women are compatible with previous studies on Bangladesh, Indonesia, and other developing countries (Biswas et al., 2017; Gertler & Zeitlin, 2002; Hossain et al., 2022; Martorell et al., 2000).
Second, the estimates suggested that employed women were less likely to be overweight and obese than those unemployed. This implies a greater tendency to be overweight or obese for the unemployed, a finding that echoes past studies (Hossain et al., 2022; Lindeboom et al., 2010). The relationship between women’s employment and BMI can be influenced by several factors, including socio-economic, cultural, and lifestyle considerations (Kinge, 2017). The workplace environment, including access to healthy food options, availability of physical activity facilities, and workplace culture, can influence dietary habits and physical activity, ultimately affecting BMI. Also, employment status and income can impact access to resources, including nutritious food and opportunities for physical activity. Differences in societal expectations across rural and urban areas related to appearance and body image may influence how women perceive and manage their weight, potentially impacting BMI.
Finally, childbearing age Bangladeshi women are less likely to be underweight and more likely to be overweight and obese as the household SES improves. This finding accords with several past studies on developing countries (Hashan et al., 2020; Subramanian et al., 2011). As household earnings rise, the likelihood of engaging in sedentary lifestyles and consuming high-caloric foods increases. These tendencies lead to greater risks of being overweight and obese.
Our findings carry important implications regarding the potential for curbing the incidence of unhealthy BMI categories for rural and urban women in Bangladesh. First, this study results suggest that specific programs and initiatives need to be tailored to address the unique challenges and contexts in rural and urban Bangladesh. Typically, these programs should aim to address issues such as undernutrition, micronutrient deficiencies and concerns related to overweight and obesity separately for underserved women population of rural and urban. Second, the findings here on the relationship between women’s education and unhealthy BMI categories are justifiable enough to strengthen employment opportunities in rural areas while promoting workplace wellness programs that improve physical activity, healthy eating, and stress management for employed women at workforce in urban Bangladesh. Third, the estimated associations between SES and unhealthy BMI categories are solid evidence to increase access to nutritious food, improve poor sanitation and expand healthcare services to low-income residents of rural Bangladesh. On the other hand, in urban and wealthier populations, changes in dietary patterns, sedentary lifestyle modification, and increases physical activity associated with urbanization and higher SES contribute to curbing the incidence of overweight and obesity.
This paper departs from the previous studies in at least three ways. First, a few of the past studies used multiple waves of BDHS data to account for trend effects while evaluating the determinants of unhealthy BMI categories (Hossain et al., 2022; Shafique et al., 2007). Second, our methodological approach is novel in this line of research. Past studies used the standard logistic regression model which tends to yield biased estimates, to analyze the survey data. The current study overcomes this limitation by adopting the multilevel nested logistic modeling approach. Moreover, we focus on a unique population or context not extensively covered in past research and it clearly contributes to a more comprehensive understanding of the topic. Lastly, our research has direct policy implications or applications compared to past studies that might not have had as clear a connection to real-world impact (Biswas et al., 2017; Khan & Kraemer, 2009; Mishra & Bera, 2023). Finally, the current study has some limitations. We only explained the statistical associations between women’s nutritional status and socio-economic determinants rather than clarifying the causal effects. BDHS does not collect data on certain important variables (e.g., income, expenditure, food intake, physical health condition, smoking habits, time to commute, sitting time, BMI of respondent’s family member). Absence of these unmeasured data elements could suggest omitted variables bias for the estimated models.
Notes
The number of women excluded from all five waves is 4712.
The WHO and Asian cutoffs for underweight are the same.
We examined all the slope coefficients with and without intercepts (Chow test). Results are available upon request.
The education variable may be biased due to unobserved heterogeneity and therefore, is likely to be endogenous. However, our study is more of a “prediction” framework (although not forecasting), rather than a causal framework; that is, we only observe correlations or associations since the DHS data are cross-sectional. To minimize any bias that may result from omitting variables related to underweight, we considered a large set of controls including the partner’s education and occupation.
We investigated the potential non-linear relationship between education and each of the three outcomes by inclusion of the dummies for different levels of schooling attainment instead of years of education. Results are available upon request. The findings from both urban and rural samples suggest that the likelihood of women being underweight decreases with their increased education level, which is consistent with the results when the year of education is considered. Additionally, the results are significant at the same statistical level from both approaches and the estimated parameters of the remaining determinants in the model remained unchanged. Therefore, for brevity we report the marginal effects on years of education.
An alternative estimated model used the wealth index factor score and its interaction term with education instead of the categorical wealth index variables. The wealth index factor score has a significant negative relationship with the underweight risk; however, the interaction effect is insignificant. Overall, results are similar in terms of the sign and significance of the determinants. These additional results are in Appendix Table 7. The Stata program used does not output the marginal effects for interaction terms, because, mathematically, it is infeasible. A marginal effect is, as suggested by the dydx notation in Stata, a first-order partial derivative of the outcome variable with respect to the explanatory variable. Since interaction terms involve two variables, the closest analogue would be a mixed second-order partial derivative.
Adding dummies for different levels of schooling attainment instead of years of education suggest that women’s risk of being overweight increases with their increased education level and brings a minuscule change in marginal effects of other determinants for both samples. Therefore, years of education is considered for brevity.
Results from the model with the wealth index factor score and the interaction term between the wealth index score and education are quantitatively similar, apart from the insignificant interaction effect. Please see Appendix Table 8.
The findings are consistent with the model including the wealth index factor score and the interaction term between the wealth index score and education. Results are reported in Appendix Table 9.
Please see Table 10 in Appendix 3. For example, compared to individuals with normal weight, an additional year of education is associated with a lower risk of being underweight while an increased risk of being overweight and obese. The marginal effect of education on being underweight is negligible among rural women compared to their urban counterparts. In contrast, the marginal effect on being overweight of education was higher among urban women than rural women. Additionally, we found that the association between obesity and education was only concentrated among urban cohort. Similarly, we found that women’s employment status at the extensive margin lowers the risk of being overweight and obese in both cohorts. Women are less likely to be underweight and more likely to be overweight and obese as their household’s socioeconomic status improves. This association between SES and obesity was mainly concentrated among women from middle-class and wealthy families for the urban sample. In contrast, the associations are significantly positive for the rural sample across all subgroups. All these findings are in line with those of the multilevel model estimates.
References
ADB. (2021). Asian Development Bank, Basic Statistics. https://www.adb.org/
Biswas, T., Garnett, S. P., Pervin, S., & Rawal, L. B. (2017). The prevalence of underweight, overweight and obesity in Bangladeshi adults: Data from a national survey. PLoS ONE, 12(5), e0177395. https://doi.org/10.1371/journal.pone.0177395
Biswas, T., Townsend, N., Magalhaes, R. S., Hasan, M., & Mamun, A. (2021). Patterns and determinants of the double burden of malnutrition at the household level in South and Southeast Asia. European Journal of Clinical Nutrition, 75(2), 385–391. https://doi.org/10.1038/s41430-020-00726-z
Cammock, R., Tonumaipe’a, D., Conn, C., Sa’uLilo, L., Tautolo, E.-S., & Nayar, S. (2021). From individual behaviour strategies to sustainable food systems: countering the obesity and non communicable diseases epidemic in New Zealand. Health Policy, 125(2), 229–238. https://doi.org/10.1016/j.healthpol.2020.12.001
Conti, G., Heckman, J., & Urzua, S. (2010). The education-health gradient. American Economic Review, 100(2), 234–238. https://doi.org/10.1257/aer.100.2.234
Costa-Font, J., & Jofre-Bonet, M. (2020). Is the intergenerational transmission of overweight ‘gender assortative’? Economics & Human Biology, 39, 100907. https://doi.org/10.1016/j.ehb.2020.100907
DHS. (2017–2018). https://dhsprogram.com/publications/publication-FR344-DHS-Final-Reports.cfm
Filmer, D., & Pritchett, L. H. (2001). Estimating wealth effects without expenditure data—or tears: an application to educational enrollments in states of India. Demography, 38(1), 115–132. https://doi.org/10.1353/dem.2001.0003
Foreit, K. (2012). Addressing poverty: a guide for considering poverty-related and other inequities in health. USAID and MEASURE evaluation. http://www.cpc.unc.edu/measure/publications/ms-08-27:70.
Forster, T., Kentikelenis, A. E., Stubbs, T. H., & King, L. P. (2020). Globalization and health equity: The impact of structural adjustment programs on developing countries. Social Science & Medicine, 267, 112496. https://doi.org/10.1016/j.socscimed.2019.112496
Gertler, P., & Zeitlin, J. (2002). Do investments in child education and nutrition improve adult health? Evidence from Indonesia.
Govindaraj, R., Raju, D., Secci, F., Chowdhury, S., & J.-J. Frere. (2017). Health and nutrition in urban bangladesh. Social Determinants and Governance. World Bank Group. Health, Nutrition & Population
Hashan, M. R., Rabbi, M. F., Haider, S. S., & Das Gupta, R. (2020). Prevalence and associated factors of underweight, overweight and obesity among women of reproductive age group in the Maldives: Evidence from a nationally representative study. PLoS ONE, 15(10), e0241621. https://doi.org/10.1371/journal.pone.0241621
Headey, D., Hoddinott, J., Ali, D., Tesfaye, R., & Dereje, M. (2015). The other Asian enigma: Explaining the rapid reduction of undernutrition in Bangladesh. World Development, 66, 749–761. https://doi.org/10.1016/j.worlddev.2014.09.022
Hossain, M. I., Habib, M. J., Zinia, F. A., Rahman, A., Methun, M. I. H., & Haq, I. (2023). Rural–urban disparities in nutritional status among ever-married women in Bangladesh: A Blinder-Oaxaca decomposition approach. PLoS ONE, 18(12), 1–17.
Hossain, S., Khudri, M. M., & Banik, R. (2022). Regional education and wealth-related inequalities in malnutrition among women in Bangladesh. Public Health Nutrition, 25(6), 1639–1657.
IHME. (2017). Health effects of overweight and obesity in 195 countries over 25 years. New England Journal of Medicine, 377(1), 13–27. https://doi.org/10.1056/NEJMoa1614362
Khan, M. M., & Kraemer, A. (2009). Factors associated with being underweight, overweight and obese among ever-married non-pregnant urban women in Bangladesh. Singapore Medical Journal, 50(8), 804.
Khudri, M. M., Rhee, K. K., Hasan, M. S., & Ahsan, K. Z. (2023). Predicting nutritional status for women of childbearing age from their economic, health, and demographic features: A supervised machine learning approach. PLoS ONE, 18(5), e0277738. https://doi.org/10.1371/journal.pone.0277738
Kinge, J. M. (2017). Waist circumference, body mass index, and employment outcomes. The European Journal of Health Economics, 18(6), 787–799. https://doi.org/10.1007/s10198-016-0833-y
Lindeboom, M., Lundborg, P., & Van Der Klaauw, B. (2010). Assessing the impact of obesity on labor market outcomes. Economics & Human Biology, 8(3), 309–319. https://doi.org/10.1016/j.ehb.2010.08.004
Mahmud, H., Shobnom, K., & Rahman, M. M. (2024). Spatial inequality in socio-economic development in Bangladesh: An analysis. Social Indicators Research, 171, 1–23.
Martorell, R., Kettel Khan, L., Hughes, M. L., & Grummer-Strawn, L. M. (2000). Obesity in women from developing countries. European Journal of Clinical Nutrition, 54(3), 247–252. https://doi.org/10.1038/sj.ejcn.1600931
Mishra, R., & Bera, S. (2023). Geospatial and environmental determinants of stunting, wasting, and underweight: Empirical evidence from rural South and Southeast Asia. Nutrition, 120, 112346.
Mizala, A., Romaguera, P., & Urquiola, M. (2007). Socioeconomic status or noise? Tradeoffs in the generation of school quality information. Journal of Development Economics, 84(1), 61–75. https://doi.org/10.1016/j.jdeveco.2006.09.003
Mukanu, M. M., Mchiza, Z.J.-R., Delobelle, P., & Throw, A. M. (2023). Nutrition policy reforms to address the double burden of malnutrition in Zambia: A prospective policy analysis. Health Policy and Planning, 38, 895–906. https://doi.org/10.1093/heapol/czad053
NIPORT. (2018). http://www.mohfw.gov.bd/index.php?option=com_content&view=article&id=51&Itemid=114&lang=en
Park, S., & Lake, E. T. (2005). Multilevel modeling of a clustered continuous outcome: Nurses’ work hours and burnout. Nursing Research, 54(6), 406. https://doi.org/10.1097/00006199-200511000-00007
Pistaferri, L. (2001). Superior information, income shocks, and the permanent income hypothesis. Review of Economics & Statistics, 83, 465–476. https://doi.org/10.1162/00346530152480117
Prioreschi, A., Wrottesley, S. V., Said-Mohamed, R., Nyati, L., Newell, M.-L., & Norris, S. A. (2021). Understanding how maternal social and biological factors are related to fetal growth in an urban South African cohort. Journal of Developmental Origins of Health and Disease, 12(1), 79–87. https://doi.org/10.1017/S2040174420000045
Rutstein, S. (1999). Wealth versus expenditure: Comparison between the DHS wealth index and household expenditures in four departments of Guatemala. ORC Macro.
Rutstein, S. O., Johnson, K., & Measure, O. M. (2004). The DHS wealth index: ORC Macro. MEASURE DHS, 6, 1–77.
Schneider, P., Popkin, B., Shekar, M., Eberwein, J. D., Block, C., & Okamura, K. S. (2020). Health and Economic Impacts of Overweight/Obesity. https://documents1.worldbank.org/curated/en/205611580359927371/pdf/Main-Report.pdf#page=95
Sen, K. K., Nilima, S., Zahura, F.-T., & Bari, W. (2023). Do education and living standard matter in breaking barriers to healthcare access among women in Bangladesh? BMC Public Health, 23(1), 1431. https://doi.org/10.1186/s12889-023-16346-8
Shafique, S., Akhter, N., Stallkamp, G., de Pee, S., Panagides, D., & Bloem, M. W. (2007). Trends of under-and overweight among rural and urban poor women indicate the double burden of malnutrition in Bangladesh. International Journal of Epidemiology, 36(2), 449–457.
StataCorp. (2021). Stata Statistical Software. https://www.stata.com/
Subramanian, S., Perkins, J. M., Özaltin, E., & Davey Smith, G. (2011). Weight of nations: A socioeconomic analysis of women in low-to middle-income countries. The American Journal of Clinical Nutrition, 93(2), 413–421.
Tumas, N., & López, S. R. (2024). Double burden of underweight and obesity: Insights from new global evidence. The Lancet. https://doi.org/10.1016/S0140-6736(24)00051-5, https://ncdrisc.org/
WHO. (2016a). The double burden of malnutrition: Policy Brief. https://www.who.int/publications/i/item/WHO-NMH-NHD-17.3
WHO. (2016b). Prevalence of underweight among adults, BMI< 18.5, crude Estimates by WHO region. https://apps.who.int/gho/data/view.main.NCDBMILT18CREGv
Yan, J. (2015). Maternal pre-pregnancy BMI, gestational weight gain, and infant birth weight: A within-family analysis in the United States. Economics & Human Biology, 18, 1–12. https://doi.org/10.1016/j.ehb.2015.03.002
Funding
Open access funding provided by SCELC, Statewide California Electronic Library Consortium.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendices
Appendix 1
Wealth index
Household wealth is a core determinant of consumption (Pistaferri, 2001). The wealth index used in DHS serves as an indicator of household-level wealth that is consistent with expenditure and income measures (Rutstein, 1999). It is a composite measure of a household’s cumulative living standard. The wealth index places individual households on a continuous scale of relative wealth. It has a mean of zero and a standard deviation of one. The household assets and characteristics selected to create the wealth index were cars, bicycles, TV, usable land, floor type, source of drinking water, type of fuel, electricity, sanitation facilities, and construction materials used. Once the index is computed, national-level wealth quintiles (from lowest to highest) are calculated by assigning the household scores obtained from principal component analysis to each de jure household member, ranking each person in the population by his or her score, and then dividing the ranking into five equal categories, each constituting of 20 percent of the population. The poorest refers to the lowest quintile (the bottommost 20%), middle-class refers to the middle 20% (41–60%) and the richest or wealthiest indicates the highest quintile (the uppermost 20%) in the index (Rutstein et al. 2004; Foreit, 2012) (See Tables
4,
5, and
6).
We used the wealth index as a determinant of malnutrition among women, which relies on the long run as well as current expenditures. The household smooths expenditures on nutrition over time and are unlikely to respond to temporary shocks by changing the malnutrition status of women. See Filmer and Pritchett (2001) for detailed clarifications.
Appendix 2
See Tables
7,
8, and
9.
Appendix 3
See Tables
10,
11,
12,
13,
14, and
15.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Khudri, M.M., Osmani, A.R. & Okunade, A.A. Determinants of unhealthy BMI among women of childbearing age in Bangladesh. J Pop Research 41, 16 (2024). https://doi.org/10.1007/s12546-024-09336-z
Accepted:
Published:
DOI: https://doi.org/10.1007/s12546-024-09336-z