
Abstract
Background
The profound health consequences of loneliness are well-established. However, less is known about the protective factors which may alleviate the effects of loneliness on mental health especially among working-age adults amidst the COVID-19 pandemic. We draw on the social ecology of resilience and examine whether resilience factors can buffer the effects of loneliness on mental distress.
Methods
Data came from the National Well-being Survey—a national study of a demographically representative sample of U.S. working-age adults (N = 4014). We used (a) structural equation models with latent variables to examine the main effects of loneliness, psychological resilience, and perceived social support on mental distress, and (b) latent moderated structural equations to estimate the latent interaction effects.
Results
Results revealed that (a) loneliness was positively associated with mental distress and psychological resilience was negatively related to mental distress, and (b) psychological resilience and perceived social support moderated the strength of the relationship between loneliness and mental distress.
Conclusions
Our study highlights the importance of psychological resilience and perceived social support as two protective factors in the relationship between loneliness and mental distress. Given that loneliness significantly predicts worse mental and physical health and higher mortality, identifying protective factors that might disrupt these connections is vital. As such, public health efforts to strengthen and expand familial and community social support networks and foster psychological resilience are urgently needed to support mental health among working-age adults during additional waves of the pandemic or future similar stressors.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Loneliness is an emotionally painful and distressing feeling resulting from a mismatch between the desired and achieved levels of social relationships with others [1, 2] and was recently declared as an “epidemic” in the United States (U.S.) [3,4,5,6] largely because of its high prevalence [7, 8] and profound health consequences [9]. The effects of loneliness on health are well-established and may be as detrimental as smoking 15 cigarettes per day [10]. Loneliness can increase health risks ranging from cardiovascular health to systolic blood pressure and incident coronary heart disease [11]. Loneliness is also associated with a range of adverse mental health outcomes such as depression and anxiety in both pre-pandemic [7, 12, 13] and pandemic studies [14]. A recent systematic review of 24 studies further substantiated that loneliness is associated with mental health symptoms among adults during the COVID-19 pandemic [14]. Mood disorders, such as depression and generalized anxiety, appear to be the most frequently examined outcomes [12].
The COVID-19 pandemic represents a unique opportunity to examine the relationship between loneliness and mental health during a universal stressor considering the significant impacts it has had on loneliness and mental health due to social distancing restrictions [14]. Moreover, given the likelihood of future waves of COVID-19 and that both loneliness and depression impact physical health and mortality [15, 16], another important question concerns the protective factors which may alleviate the effects of loneliness on mental health, especially during such a global stressor. Identifying such protective factors can inform public health and mental health efforts during additional waves of the pandemic. Guided by the social ecology of resilience [17], we examine whether two resilience factors—psychological resilience and perceived social support—would moderate the relationship between loneliness and mental distress using a national sample of U.S. working-age adults (ages 18–64) that was collected in early 2021.
Loneliness and Mental Distress: the Role of Resilience Factors
Adults vary in their degree of susceptibility to the feeling of loneliness, and such susceptibility involves a wide array of interactions between social, psychological, and individual attributes [18,19,20]. Resilience is a potentially significant factor that can help explain why similar experiences of loneliness have different mental health implications for individuals. According to Windle [20, p12], resilience is “the process of effectively negotiating, adapting to, or managing significant sources of stress or trauma. Assets and resources within the individual, their life and environment facilitate this capacity for adaptation and ‘bouncing back’ in the face of adversity.” To understand how resilience influences mental distress in the presence of loneliness, and in line with Windle’s perspective, we draw on the social ecology of resilience [21] and conceptualize resilience as a multilevel construct. Specifically, we include both the positive individual attribute (i.e., psychological resilience) and external social resources (i.e., perceived social support) as potential protective factors that would buffer against the detrimental effect of loneliness on mental distress.
Psychological resilience is a learned capacity that builds developmentally over time and is generally considered as having the ability to “bounce back” from setbacks in life, or the ability to maintain a steady mental state despite acute setbacks or events [22,23,24]. Previous research suggests that psychological resilience is one of the most important personal attributes that is associated with mental health outcomes and can help explain variation in an individual’s vulnerability to stress [24, 25]. Further, it is a key target for depression and anxiety treatment [26]. In general, less resilient individuals are more vulnerable to adversities [27, 28]. Studies conducted during the COVID-19 pandemic also substantiated the main and buffering effect of psychological resilience. For example, less resilient American adults were more likely to experience increases in mental distress in the early months of the pandemic [29]. Using data collected during the acute COVID-19 outbreak in April 2020, Barzilay and colleagues found that psychological resilience moderated the relationships between COVID-19-related worries and anxiety and depression among healthcare and non-healthcare professionals [30]. Likewise, Traunmüller and colleagues found that psychological resilience buffered the psychological impact of COVID-19 on anxiety symptoms among a large sample of Austrian adults [31]. The existing literature has suggested that psychological resilience plays a protective or buffering role in the relationships between stressors and well-being outcomes [30, 31]. Hence, we expand on extant literature by taking the next step to examine the protective role of psychological resilience on the link between loneliness, a prevalent stressor, and mental distress among working-age adults.
Perceived social support refers to an individual’s subjective appraisal of the availability of resources when needed as well as the quality of these resources [32]; it is a proven buffer to reducing stress, depression, and anxiety [33, 34]. The social ecology of resilience suggests that the social environment can have an equally—if not more—important role in shaping overall resilience compared to individual-level factors [21]. Research has empirically documented that perceived social support is not only an independent predictor of mental health problems such as depression in both pre-pandemic [35, 36] and pandemic studies [33, 34], but also a factor that moderates the association between stress and mental distress [37,38,39,40]. For example, adults with higher perceived social support reported significantly lower levels of depression compared to those with lower perceived social support during the COVID-19 pandemic [33]. In light of these findings and the fact that social support is a potentially modifiable factor [41, 42], it is important to empirically examine perceived social support as a protective factor in the link between loneliness and mental distress.
Drawing on data from a demographically representative sample of U.S. working-age adults, this study investigates the moderating effects of two modifiable resilience factors (i.e., psychological resilience and perceived social support) on the link between loneliness and mental distress. We hypothesized that (a) the main effects of loneliness, psychological resilience, and perceived social support on mental distress would be significant and (b) the relationship between loneliness and mental distress would be stronger when adults report lower psychological resilience (vs. higher psychological resilience) or lower perceived social support (vs. higher perceived social support).
Method
Data and Participants
Data were from the National Well-being Survey (NWS; redacted for the peer-reviewing process), a national cross-sectional survey of working-age adults of ages 18–64 in the United States. Data were collected in February and March of 2021 through an online survey. Recruitment of survey participants was done by Qualtrics Panels. To recruit participants, Qualtrics drew from a database of more than a million U.S. adults. Special attention was given to recruiting a sample that was demographically representative based on age and sex as well as race and ethnicity of the working-age population in the U.S. Participants were compensated. Compensation varied in amount and type based on the recruitment strategy used by Qualtrics (e.g., SkyMiles rewards, points to retail outlets, gift cards). The final sample contained 4014 working-age adults (ages 18–64). Post-stratification weights were created by Qualtrics to ensure that the sample approximates the distributions of age, sex, race and ethnicity, and education from the American Community Survey estimates from 2015 to 2019. We applied the sampling weights to all analyses. The NWS completion rate (40.4%) represents the total number of survey respondents (N = 4014) among those who clicked on the survey link and viewed the NWS survey invitation and informed consent page (N = 11,580). NWS data collection was approved by the Institutional Review Board at Syracuse University.
Measures
Mental Distress
In line with other research [29], mental distress was measured using the Patient Health Questionnaire-4 (PHQ-4), which is an ultra-brief screener for core symptoms of depression and anxiety [43]. It is a validated scale which includes two items of PHQ-2: “During the past two weeks, how often have you been bothered by: having little interest or pleasure in doing things; and feeling down, depressed, or hopeless,” and two items of generalized anxiety disorder [44]: “During the past two weeks, how often have you been bothered by: feeling nervous, anxious, or on edge; and not being able to control worrying.” Participants reported on a scale of 0 (not at all) to 3 (nearly every day). To account for measurement error, we included mental distress as a latent variable, composed of four manifest items mentioned earlier.
Loneliness
Loneliness was measured with the three-item UCLA Loneliness Scale Short-Form [45]. Respondents were asked three questions: “How often do you feel left out?” “How often do you feel you lack companionship?” and “How often do you feel isolated from others?” on a scale of 1 (never) to 4 (always). The latent loneliness variable was based on the three manifest items.
Psychological Resilience
The six-item Brief Resilience Scale was used to assess psychological resilience [23]. Responses were on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). Items included three positively worded statements: “I tend to bounce back quickly after hard times,” “It does not take me long to recover from a stressful event,” and “I usually come through difficult times with little trouble,” and three negatively worded statements “I have a hard time making it through stressful events,” “It is hard for me to snap back when something bad happens,” and “I tend to take a long time to get over setbacks in my life.” The three negatively worded items were reverse coded. The latent psychological resilience variable was composed of these six items.
Perceived Social Support
We used three survey questions to capture perceived social support [46]. Two survey questions were about instrumental support: “Is there someone you could count on if you needed a loan for $200 (1 = yes, 0 = no)?” and “Is there someone you could count on if you needed a place to live (1 = yes, 0 = no)?” and another one about emotional support: “How much are friends or relatives willing to listen when you need to talk about your worries or problems (1 [not at all] to 4 [a great deal])?” The latent perceived social support variable was composed of these three items.
Covariates
Given that specific factors, such as gender, age, marital status, and physical health, are related to mental health symptoms [1, 47], participants’ sociodemographic characteristics and health-related factors were included as covariates (see Tables 1 and 2 for detailed coding). These included age, sex, race and ethnicity, marital status, living arrangement, participants’ highest level of education completed, household’s total income from all sources before taxes and deductions in 2019, and self-rated physical health. Given that data were collected during the COVID-19 pandemic, we also controlled for the impact of COVID-19 which was a self-report measure.
Statistical Analysis
We first ran descriptive statistics for the data, then used confirmatory factor analysis (CFA) to test a four-factor measurement model (Fig. 1) and evaluated the convergent and discriminant validity of the four latent constructs (shown as ovals in Fig. 1) [48, 49]. Convergent validity is evaluated based on the factor loadings of their respective hypothesized latent factors while discriminant validity is examined via the correlation between latent constructs [50]. Next, we conducted a structural equation model (SEM) without the latent interaction term to test the main effects of loneliness, perceived social support, and psychological resilience on mental distress with all covariates included in the model. This step allowed us (a) to compare the model fit between the model without the latent interactions and the next model with the latent interactions wherein Mplus does not provide conventional fit indices and (b) to compute the effect size of the interaction effects [51]. As recommended by Dawson [52], we used Cohen’s f2 to report the proportion of residual variance in the latent dependent variable accounted for by the latent interaction, over and above what was accounted for by the main effects and other control variables [53]. Last, we estimated the two hypothesized latent interaction effects one by one using latent moderated structural (LMS) models [54]. When the interaction effect was significant, we used simple slope analyses (one standard deviation [SD] above and below the mean of the moderator) and probed the interaction effect to interpret the latent interaction effect [55]. We chose the latent variable modeling approach for testing interactions mainly because the traditional and standard regression analysis method for interaction estimation—including the product of the sum scores of the independent variable and the moderator—has been limited for several reasons. For example, regression using sum/mean scores does not account for measurement errors of the imperfectly measured psychological constructs which may attenuate the true strength of the interaction effect [56]. We used the full information maximum likelihood estimation method to handle missing data, which enabled the full usage of all available data [57]. All SEM analyses were conducted using Mplus Version 8 [57].

The four-factor measurement model. Note: Ovals correspond to latent variables; rectangles, to observed variables; ɛ, to measurement error; and dashed lines, to latent covariances
Results
Descriptive Analyses
Table 1 displays the demographic characteristics of the participants. The mean age was 40.7 ± 13.8 years old. Of the 4014 participants, 2040 (50.4%) were female. Over one third of the respondents were single or never married (33.6%), and had a bachelor’s degree or higher (31.1%). Nearly 42% reported that COVID-19 had a negative impact on their lives, and 20% reported living alone. Means and percentages were weighted.
Measurement Model Estimation
We tested a four-factor measurement model (Fig. 1), in which the 16 observed indicators loaded on four hypothesized factors. The measurement model fit the data very well: χ2(82) = 189.40, p = 1.71, comparative fit index (CFI) = 0.99, root-mean-square error of approximation (RMSEA) = 0.018 [0.015, 0.021], and standardized root-mean-squared residual (SRMR) = 0.020. All unstandardized factor loadings of indicators on their respective hypothesized latent factors were strong and significant (p < 0.001), and all standardized factor loadings were all greater than the fair factor loading cut-off of 0.45 suggested by Tabachnich and Fidell [58]. The factor loadings of all indicators and Cronbach’s α (above 0.81) are summarized in Electronic Supplemental Material Table 1. The standardized factor loadings ranged from 0.47 to 0.89 (p < 0.001) across variables. Further, the correlation coefficients among all latent variables ranged from |− 0.42| to |0.66|, indicating that these were four distinct variables. Taken together, the CFA results provided support for both convergent and discriminant validity. Thus, we included the configuration of the indicators on these four latent factors established in the measurement model in the subsequent analyses.
Main Effects of Loneliness, Psychological Resilience, and Perceived Social Support on Mental Distress
The structural model had a good fit: χ2(190) = 680.64, p < 0.001, CFI = 0.974, RMSEA = 0.025 [0.023, 0.027], SRMR = 0.023. As hypothesized, we found that the main effects of loneliness (b = 0.46, SE = 0.04, p < 0.001, β = 0.38) and psychological resilience (b = –0.37, SE = 0.04, p < 0.001, β = –0.33) on mental distress were significant after adjusting all covariates (see Table 2 for coefficients for all control variables). However, the main effect of perceived social support (b = − 0.04, SE = 0.06, p = 0.58, β = − 0.02) on mental distress was not significant.
The Buffering Effects of Psychological Resilience and Perceived Social Support
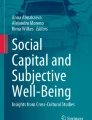
We first evaluated the model fit of the LMS model by comparing the model fit of the models with and without the latent interaction term using the Satorra-Bentler scaled chi-square difference test TRd [54]. The differences in scaled loglikelihood were significant (psychological resilience: TRd (df = 1) = 65.87, p < 0.0001, and perceived social support: TRd (df = 1) = 30.02, p < 0.0001), indicating that LMS models provided better fit to the data than the SEM without the interaction term. Further, we found two significant interaction effects between loneliness and psychological resilience as well as between loneliness and perceived social support on mental distress. Unstandardized interaction coefficients are presented in Table 2. The interaction between loneliness and psychological resilience was also significant: b = − 0.32, SE = 0.04, p < 0.001, β = − 0.17. As shown in Fig. 2, loneliness was more strongly associated with mental distress when psychological resilience was lower (vs. higher). Specifically, the simple slope test revealed that when psychological resilience was one SD below the mean, the effect of loneliness on mental distress was statistically significant (b = 0.66, SE = 0.05, p < 0.001). When psychological resilience was one SD above the mean, the effect of loneliness on mental distress was also statistically significant (b = 0.25, SE = 0.04, p < 0.001), but weaker than that when psychological resilience was one SD below the mean. The inclusion of the latent interaction term (loneliness × psychological resilience) accounted for an additional 6.7% of the variances in mental distress with a medium effect size f2 = 0.19.

Standardized effects of loneliness and mental distress conditional on psychological resilience. Note: When psychological resilience is lower, the positive association between loneliness and mental distress is stronger
There was a significant interaction between loneliness and perceived social support: b = − 0.42, SE = 0.08, p < 0.001, β = − 0.11. As shown in Fig. 3, loneliness was more strongly associated with mental distress when adults’ perceived social support was lower (vs. higher). Specifically, the simple slope test revealed that when perceived social support was one SD below the mean, the effect of loneliness on mental distress was statistically significant (b = 0.60, SE = 0.05, p < 0.001). When perceived social support was one SD above the mean, the effect of loneliness on mental distress was also statistically significant (b = 0.34, SE = 0.04, p < 0.001), but weaker than that when perceived social support was one SD below the mean. The inclusion of the latent interaction term (loneliness × perceived social support) accounted for an additional 1.5% of the variances in mental distress with a small effect size f2 = 0.04.

Standardized effects of loneliness and mental distress conditional on perceived social support. Note: When perceived social support is lower, the positive association between loneliness and mental distress is stronger
Discussion
Loneliness is prevalent among adults and has been conceptually and empirically linked to a myriad of mental health problems, such as depressive symptoms and anxiety [1, 7, 12, 13]. Given that the ongoing pandemic will likely continue to influence feelings of loneliness [4, 59], it is imperative to provide public health professionals and other practitioners with empirical evidence about what factors buffer the relationship between loneliness and mental distress, which can further help them identify and select appropriate intervention and prevention strategies. We drew on the social ecology of resilience [17], and examined working-age adults’ psychological resilience and perceived social support as two types of resilience factors and investigated them as moderators between loneliness and mental distress.
Results supported prior research by demonstrating that loneliness was a risk factor for mental distress among working-age adults [12]. Specifically, we found that higher levels of loneliness were associated with elevated mental distress after controlling for age, gender, race and ethnicity, education, income, marital status, living arrangement, self-reported physical health, and COVID-19 impact as well as the two psychosocial factors: psychological resilience and perceived social support. This finding supports the stress model which posits loneliness as a common stressor is associated with poor mental health outcomes [60].
Our findings also shed light on differences in the relationship between loneliness and distress among working-age adults. We found that, when individuals were more resilient or in the context of high social support, the strength of the relationship between loneliness and mental distress was weaker, suggesting that psychological resilience and perceived social support are protective factors. Prior studies suggest that adults who are psychologically resilient tend to have the ability to perform adaptive functioning when under stress or feeling lonely [22, 61, 62], and this ultimately helps them maintain a steady mental state or healthy process despite adversity [29]. Given that psychological resilience can be learned [27] and the protective role of psychological resilience in well-being and coping in the presence of stress, universal campaigns or interventions that foster psychological resilience are urgently needed to protect the mental health of American adults. These findings highlight the importance of fostering working-age adults’ psychological resilience as it is modifiable and can be enhanced through psychological therapy interventions (e.g., mindfulness-based therapies, tai chi qigong meditation, and visual art discussions) [41, 42, 63], which in turn appear to offer protection against loneliness [64, 65]. A recent comprehensive meta-analysis of 268 studies on the overall efficacy of resilience interventions concluded that “resilience-promoting interventions yielded a small, but statistically significant overall effect” [64].
Our finding that perceived social support is a protective factor further confirms the social support and buffering theory [37] which posits that support protects against the negative effects of loneliness and promotes mental health. However, it is worth noting that the effect size of the perceived social support interaction effect is relatively small, suggesting that it may be of little practical significance. Indeed, effective interventions designed to improve perceived social support are limited despite theory and a large body of literature pointing to the benefits of perceived social support in mental health. Psychoeducation is a common approach used by practitioners or clinicians to improve individual’s perceived social support; however, the effectiveness is mixed [66]. Therefore, further development and testing of interventions of this kind are warranted, and our study findings might have implications for informing these efforts.
Some limitations should be considered when evaluating the implications of the study findings. First, the data used in the current study were collected through an online survey and thus may be subject to selection bias as online surveys require internet access. However, prior research has documented that Qualtrics is a credible platform that can collect representative national data especially when post-stratification weights are used [67]. Moreover, other studies using this dataset have reported comparable univariate estimates to other national representative survey datasets [68]. Second, this is a cross-sectional study. Although the existing literature guided us to make hypotheses regarding the direction of the relationships between study variables, causal implications cannot be assumed. Therefore, future studies using a longitudinal, rather than cross-sectional, design may provide better inferences about the direction of relationships. Third, we used self-reported measures, which were not clinical diagnoses. Given the unfeasibility of conducting clinical diagnoses in a large sample, we used well-established and self-reported measures. Future studies are needed to use multiple measures in addition to self-reported assessment. Finally, although we included the perceived impact of COVID-19 as a covariate, it was assessed using a single-item measure. Future studies should further examine whether the relationship between loneliness and mental distress is conditioned on different life domains impacted by COVID-19.
In conclusion, our study highlights the importance of psychological resilience and perceived social support as two protective factors in the relationship between loneliness and mental distress for U.S. working-age adults amidst the COVID-19 pandemic. Given that loneliness is predictive of mental and physical health and higher mortality [11], identifying protective factors that might disrupt these connections is vital. As such, public health efforts to strengthen and expand familial and community social support networks and foster psychological resilience will be essential to supporting mental health during additional waves of the pandemic or future similar stressors.
Data Availability
The data that support the findings of this study are available from Syracuse University Lerner Center Public Health Promotion and Population Health, but restrictions apply to the availability of these data, which were used under license for the current study.
References
Cacioppo JT, Hughes ME, Waite LJ, Hawkley LC, Thisted RA. Loneliness as a specific risk factor for depressive symptoms: cross-sectional and longitudinal analyses. Psychol Aging. 2006;21(1):140–51.
Perlman D, Peplau LA. Toward a social psychology of loneliness. In: S. Duck & R. Gilmour, editor. Personal relationships in disorder. Eds. London: Academic Press; 1981.
Demarinis S. Loneliness at epidemic levels in America. EXPLORE. 2020;16(5):278–9.
Jeste DV, Lee EE, Cacioppo S. Battling the modern behavioral epidemic of loneliness: suggestions for research and interventions. JAMA Psychiat. 2020;77(6):553.
Palgi Y, Shrira A, Ring L, Bodner E, Avidor S, Bergman Y, et al. The loneliness pandemic: loneliness and other concomitants of depression, anxiety and their comorbidity during the COVID-19 outbreak. J Affect Disord. 2020;275:109.
Trad NK, Wharam JF, Druss B. Addressing loneliness in the era of COVID-19. JAMA Heal Forum. 2020;1(6):e200631–e200631.
Beutel ME, Klein EM, Brähler E, Reiner I, Jünger C, Michal M, et al. Loneliness in the general population: prevalence, determinants and relations to mental health. BMC Psychiatry. 2017;17(1).
Lee EE, Depp C, Palmer BW, Glorioso D, Daly R, Liu J, et al. High prevalence and adverse health effects of loneliness in community-dwelling adults across the lifespan: role of wisdom as a protective factor. Int psychogeriatrics. 2019;31(10):1447–62.
Leigh-Hunt N, Bagguley D, Bash K, Turner V, Turnbull S, Valtorta N, et al. An overview of systematic reviews on the public health consequences of social isolation and loneliness. Public Health. 2017;152:157–71.
Holt-Lunstad J, Robles TF, Sbarra DA. Advancing social connection as a public health priority in the United States. Am Psychol. 2017;72(6):517–30.
Hawkley LC, Cacioppo JT. Loneliness matters: a theoretical and empirical review of consequences and mechanisms. Ann Behav Med. 2010;40(2):218–27.
Erzen E, Çikrikci Ö. The effect of loneliness on depression: a meta-analysis. Int J Soc Psychiatry. 2018;64(5):427–35.
Santini ZI, Koyanagi A, Tyrovolas S, Mason C, Haro JM. The association between social relationships and depression: a systematic review. J Affect Disord. 2015;175:53–65.
Pai N, Vella SL. COVID-19 and loneliness: a rapid systematic review. Aust N Z J Psychiatry. 2021;55(12):1144–56.
Holt-Lunstad J, Smith TB, Baker M, Harris T, Stephenson D. Loneliness and social isolation as risk factors for mortality: a meta-analytic review. Perspect Psychol Sci. 2015;10(2):227–37.
Holwerda TJ, Van Tilburg TG, Deeg DJH, Schutter N, Dekker J, Stek ML, et al. Impact of loneliness and depression on mortality: results from the Longitudinal Ageing Study Amsterdam. Br J Psychiatry. 2016;209(2):127–34.
Ungar M. The social ecology of resilience: addressing contextual and cultural ambiguity of a nascent construct. Am J Orthopsychiatry. 2011;81(1):1–17.
Killgore WDS, Taylor EC, Cloonan SA, Dailey NS. Psychological resilience during the COVID-19 lockdown. Psychiatry Res. 2020;291: 113216.
Weeks DG, Michela JL, Peplau LA, Bragg ME. Relation between loneliness and depression: a structural equation analysis. J Pers Soc Psychol. 1980;39(6):1238–44.
Windle G. What is resilience? A review and concept analysis. Rev Clin Gerontol. 2011;21(2):152–69.
Ungar M, Liebenberg L. Assessing resilience across cultures using mixed methods: construction of the child and youth resilience measure. J Mix Methods Res. 2011;5(2):126–49.
Masten AS. Resilience in developing systems: progress and promise as the fourth wave rises. Dev Psychopathol. 2007;19(3):921–30.
Smith BW, Dalen J, Wiggins K, Tooley E, Christopher P, Bernard J. The brief resilience scale: assessing the ability to bounce back. Int J Behav Med. 2008;15(3):194–200.
Southwick SM, Bonanno GA, Masten AS, Panter-Brick C, Yehuda R. Resilience definitions, theory, and challenges: interdisciplinary perspectives. Eur J Psychotraumatol. 2014;5(1).
Anyan F, Hjemdal O. Adolescent stress and symptoms of anxiety and depression: resilience explains and differentiates the relationships. J Affect Disord. 2016;203:213–20.
Connor KM, Zhang W. Resilience: determinants, measurement, and treatment responsiveness. CNS Spectr. 2006;11(S12):5–12.
PeConga EK, Gauthier GM, Holloway A, Walker RSW, Rosencrans PL, Zoellner LA, et al. Resilience is spreading: mental health within the COVID-19 pandemic. Psychol Trauma Theory, Res Pract Policy. 2020;12(S1):S47.
Smith BW, Dalen J, Wiggins K, Tooley E, Christopher P, Bernard J. The brief resilience scale: assessing the ability to bounce back. Int J Behav Med. 2008;15(3):194–200.
Riehm KE, Brenneke SG, Adams LB, Gilan D, Lieb K, Kunzler AM, et al. Association between psychological resilience and changes in mental distress during the COVID-19 pandemic. J Affect Disord. 2021;282:381–5.
Barzilay R, Moore TM, Greenberg DM, DiDomenico GE, Brown LA, White LK, et al. Resilience, COVID-19-related stress, anxiety and depression during the pandemic in a large population enriched for healthcare providers. Transl Psychiatry. 2020;10(1):1–8.
Traunmüller C, Stefitz R, Schneider M, Schwerdtfeger A. Resilience moderates the relationship between the psychological impact of COVID-19 and anxiety. Psychol Health Med. 2021;1–12.
Pierce G, Sarason IG, Sarason B. Coping and social support. In: Zeidner M, ENDLER N, editors. Handbook of coping : theory, research, applications. Eds. John Wiley & Sons; 1996. pp. 434–51.
Grey I, Arora T, Thomas J, Saneh A, Tomhe P, Abi-Habib R. The role of perceived social support on depression and sleep during the COVID-19 pandemic. Psychiatry Res. 2020;293: 113452.
Mariani R, Renzi A, Di Trani M, Trabucchi G, Danskin K, Tambelli R. The impact of coping strategies and perceived family support on depressive and anxious symptomatology during the coronavirus pandemic (COVID-19) lockdown. Front Psychiatry. 2020;11:1195.
Gariépy G, Honkaniemi H, Quesnel-Vallée A. Social support and protection from depression: systematic review of current findings in western countries. Br J Psychiatry. 2016;209(4):284–93.
Wang J, Mann F, Lloyd-Evans B, Ma R, Johnson S. Associations between loneliness and perceived social support and outcomes of mental health problems: a systematic review. BMC Psychiatry. 2018;18(1):1–16.
Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. Psychol Bull. 1985;98(2):310–57.
Aneshensel CS, Stone JD. Stress and depression: a test of the buffering model of social support. Arch Gen Psychiatry. 1982;39(12):1392–6.
Park CL, Finkelstein-Fox L, Russell BS, Fendrich M, Hutchison M, Becker J. Psychological resilience early in the COVID-19 pandemic: stressors, resources, and coping strategies in a national sample of Americans. Am Psychol. 2021;76(5):715.
Takizawa T, Kondo T, Sakihara S, Ariizumi M, Watanabe N, Oyama H. Stress buffering effects of social support on depressive symptoms in middle age: reciprocity and community mental health. Psychiatry Clin Neurosci. 2006;60(6):652–61.
Chmitorz A, Kunzler A, Helmreich I, Tüscher O, Kalisch R, Kubiak T, et al. Intervention studies to foster resilience – a systematic review and proposal for a resilience framework in future intervention studies. Clin Psychol Rev. 2018;59:78–100.
Helmreich I, Kunzler A, Chmitorz A, König J, Binder H, Wessa M, et al. Psychological interventions for resilience enhancement in adults. Cochrane Database Syst Rev. 2017;2017(2).
Kroenke K, Spitzer RL, Williams JBW, Löwe B. An ultra-brief screening scale for anxiety and depression: the PHQ-4. Psychosomatics. 2009;50(6):613–21.
Löwe B, Wahl I, Rose M, Spitzer C, Glaesmer H, Wingenfeld K, et al. A 4-item measure of depression and anxiety: validation and standardization of the Patient Health Questionnaire-4 (PHQ-4) in the general population. J Affect Disord. 2010;122(1–2):86–95.
Hughes ME, Waite LJ, Hawkley LC, Cacioppo JT. A short scale for measuring loneliness in large surveys results from two population-based studies. Res Aging. 2004;26(6):655–72.
Harknett KS, Hartnett CS. Who lacks support and why? An examination of mothers’ personal safety nets. J Marriage Fam. 2011;73(4):861.
Panzeri A, Bertamini M, Butter S, Levita L, Gibson-Miller J, Vidotto G, et al. Factors impacting resilience as a result of exposure to COVID-19: the ecological resilience model. PLoS ONE. 2021;16(8): e0256041.
Bagozzi RP, Phillips LW, Yi Y. Assessing construct validity in organizational research. Adm Sci Q. 1991;36(3):421–58.
Bollen KA. Structural equations with latent variables. New York: Wiley; 1989.
Cole DA. Utility of confirmatory factor analysis in test validation research. J Consult Clin Psychol. 1987;55(4):584–94.
Cheung GW, Cooper-Thomas HD, Lau RS, Wang LC. Testing moderation in business and psychological studies with latent moderated structural equations. J Bus Psychol. 2021;36(6):1009–33.
Dawson JF. Moderation in management research: what, why, when, and how. J Bus Psychol. 2013;29(1):1–19.
Cohen J. Statistical power analysis for the behavioral sciences. Stat Power Anal Behav Sci. 2013.
Muthén BO. Latent variable interactions. Technical note, 1–9. 2012. Retrieved from: http://www.statmodel.com/download/LVinteraction.pdf.
Aiken LS, West SG. Interactions between categorical and continuous variables. Multiple regression: testing and interpreting interactions. SAGE Publications Inc. 1991.
Lodder P, Denollet J, Emons WHM, Nefs G, Pouwer F, Speight J, et al. Modeling interactions between latent variables in research on type D personality: a Monte Carlo simulation and clinical study of depression and anxiety. Multivariate Behav Res. 2019;54(5):637–65.
Muthén LK, Muthén BO. Mplus user’s guide. Los Angeles, CA: Muthén & Muthén. 1998–2017.
Tabachnick BG, Fidell LS. Using multivariate statistics, vol. 20. London: Allyn & Bacon/Pearson Education; 2007.
Lim MH, Eres R, Vasan S. Understanding loneliness in the twenty-first century: an update on correlates, risk factors, and potential solutions. Soc Psychiatry Psychiatr Epidemiol. 2020;55(7):793–810.
Pearlin LI, Lieberman MA, Menaghan EG, Mullan JT. The stress process. J Health Soc Behav. 1981;22(4):337–56.
Jakobsen IS, Madsen LMR, Mau M, Hjemdal O, Friborg O. The relationship between resilience and loneliness elucidated by a Danish version of the resilience scale for adults. BMC Psychol. 2020;8(1):1–10.
Luthar SS, Cicchetti D. The construct of resilience: implications for interventions and social policies. Dev Psychopathol. 2000;12(4):857–85.
Southwick SM, Pietrzak RH, White G. Interventions to enhance resilience and resilience-related constructs in adults. Resil Ment Heal Challenges Across Lifesp. 2011;289–306.
Liu JJW, Ein N, Gervasio J, Battaion M, Reed M, Vickers K. Comprehensive meta-analysis of resilience interventions. Clin Psychol Rev. 2020;82: 101919.
Williams CYK, Townson AT, Kapur M, Ferreira AF, Nunn R, Galante J, et al. Interventions to reduce social isolation and loneliness during COVID-19 physical distancing measures: a rapid systematic review. PLoS ONE. 2021;16(2): e0247139.
Hogan BE, Linden W, Najarian B. Social support interventions: do they work? Clin Psychol Rev. 2014;22:381–440.
Heen M, Lieberman J, Miethe T. A comparison of different online sampling approaches for generating national samples. 2014. Retrieved from: https://www.unlv.edu/sites/default/files/page_files/27/ComparisonDifferentOnlineSampling.pdf.
Monnat SM. Rural-Urban variation in COVID-19 experiences and impacts among U.S. working-age adults. Ann Am Acad Pol Soc Sci. 2021;698(1):111–36.
Acknowledgements
Dr. Rhubart acknowledges support from the NICHD-funded Population Research Institute at the Pennsylvania State University (P2CHD041025), the Interdisciplinary Network on Rural Population Health and Aging funded by the National Institute on Aging (R24 AG065159), and the USDA Agricultural Experiment Station Multistate Research Project: W4001, Social, Economic and Environmental Causes and Consequences of Demographic Change in Rural America. All authors acknowledge support from the Syracuse University Lerner Center for Public Health Promotion.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Zhang, X., Brown, A.M. & Rhubart, D.C. Can Resilience Buffer the Effects of Loneliness on Mental Distress Among Working-Age Adults in the United States During the COVID-19 Pandemic? A Latent Moderated Structural Modeling Analysis. Int.J. Behav. Med. 30, 790–800 (2023). https://doi.org/10.1007/s12529-022-10151-0
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12529-022-10151-0