
Abstract
Normative transitions between educational settings can be important life events for young people, having the potential to influence mental health trajectories across the life course. Interventions to target transitions have been used to support children and young people as they transition between school settings, but there is limited synthesis of their effects. Seven databases were searched to identify studies of universal interventions focused on supporting mental health and wellbeing across three main types of educational transition: preschool to elementary school; school to school (including elementary to middle; middle to high and other combinations depending on country); and high school to post-compulsory education. Effect directions for behavioural, psychological/emotional and social measures of mental health were extracted for each study and synthesized using effect direction plot methodology. Searches identified 6494 records for screening. This resulted in 34 papers being included in the review, consisting of 24 different interventions. Social outcomes appeared more amenable to intervention than behavioural outcomes, with mixed findings for psychological measures of mental health. Intervention characteristics shifted based on the age of young person involved in the transition, with greater focus on parenting and school environment during the early transitions, and more focus on social support for the transition to post-compulsory education. A broad range of interventions were identified for supporting mental health and wellbeing across the three types of educational transition with mixed impact and diverse methodologies. More research is needed to identify transferable intervention mechanisms that may hold across different contexts and settings. PROSPERO registration number: CRD42020176336.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Schools are environments that can provide opportunities for, and threats to, optimal social and emotional development (Bonell et al., 2013). Schools have a long history as settings for interventions to improve health and wellbeing (for example, Jacob et al., 2021; Langford et al., 2015; Shackleton et al., 2016), both because of the important role of the school environment for wellbeing and because schools offer a means of accessing large numbers of young people at the same time. A gap however is that most of the school health literature focuses on each type of school (e.g. elementary/middle/high school) as distinct intervention settings, resulting in less robust evaluation or systematic review literature on interventions which connect two or more through a focus on transition. This single setting focus is understandable due to the methodological complexity of longitudinal approaches that follow children between two settings. However, it is also problematic because transition is an important milestone in child development which provides huge opportunities for both adaptive and maladaptive social and emotional development that may result in inequalities that persist across the life course (Gotlib & Blair, 1997; Symonds, 2015). Young people with more social, financial and flexible resources (Phelan et al., 2010; Taylor & Broffman, 2011) are likely to be more resilient to the challenges posed by transition. These resources can be used to mitigate against the stresses of transition and to turn the process from a potential threat to wellbeing into a challenge that they can respond positively to (Sirsch, 2003). One group who may have fewer resources available to them are young people from low socioeconomic (SES) backgrounds (Gallo et al., 2009; Phelan et al., 2010), and their mental health and wellbeing has been shown to be at particular at risk across different types of educational transitions (Aina et al., 2022; Crosnoe & Ansari, 2016; Jindal-Snape et al., 2020).
The transition into school from a pre-school or nursery setting has been viewed as an important point in time for intervention. ‘School readiness’, often described in academic, emotional and behavioural terms (Duncan et al., 2007), is a well-established predictor of future academic outcomes (Pan et al., 2019) and is also increasingly being linked to future child and adolescent wellbeing (Gregory et al., 2021). Mental health problems contribute to, and are inextricably linked to, school readiness. In an Australian sample of 500 young children assessed from 1.5 to 5 years of age, approximately 20% were shown to have a high externalizing problems trajectory; 20% were also shown to have a high internalizing problems trajectory (Bayer et al., 2012). Children from low-income families are more likely to start preschool with emotional and behavioural difficulties (Comeau & Boyle, 2018; Li et al., 2017), although even within this subpopulation, there are differences relating to relative levels of poverty and life experiences (Roy & Raver, 2014).
Transition also occurs between schools as children age. In the UK, this almost universally occurs at ages 11–12, with the transition from primary to secondary school. In the USA, young people may transition from elementary to middle school at age 11 and then to high school at age 14, or go straight from elementary to high school at age 14—and other countries may differ further. The transition out of primary/elementary school can create simultaneous feelings of excitement and worry in young people (Moore et al., 2021). A recent systematic review (Jindal-Snape et al, 2020) suggests a negative relationship between primary to secondary transition and educational outcomes, but more mixed findings for mental health and wellbeing. This may be due to subpopulations of young people who experience transition more or less positively than the average (Gazelle & Faldowski, 2019).
Having completed secondary or high school, many young people will then go on to experience an educational transition from school to post-compulsory education. In some countries this may include a move to further education (at age 16) or higher education—generally university or college (at age 18). It often marks the first time a young person leaves home and has to build a life for themselves that is separate from their family, as well as having to negotiate new academic expectations, increased autonomy and responsibility, and build new friendships (Arnett, 2000). A meta-analysis found that, on average, nearly a third (30.6%) of university students experienced depression at any one time, much higher than the general population (Ibrahim et al., 2013). Having more positive social and emotional adjustment trajectories across the high school to university transition is associated with increased rates of graduation for disadvantaged young people, but not for those from higher income families (Larose et al., 2019). Experiencing chronic stressors in the first year of university is associated with poorer mental health outcomes, and chronic stressors are more common among first-generation students (Kroshus et al., 2021).
Educational transitions offer an important opportunity to target mental health and wellbeing outcomes in young people with the potential to improve quality of life, school adjustment and to have long-lasting academic, emotional and behavioural effects across the life course. Interventions can either be universal or targeted at specific groups of individuals. Rose (2001) argues that public health interventions have the greatest power when they take a preventive approach of shifting the whole normal curve of health outcomes rather than solely focusing on those at the bottom end of the curve. This is in part because of the difficulties of accurately identifying those individuals whose health may deteriorate in future and who would be excluded from a targeted approach. This review will focus on universal interventions, unless the interventions are specifically targeted at young people from low SES backgrounds. Low socioeconomic status (SES) is associated with chronic stress due to poor living and working conditions, discrimination, a sense of powerlessness and financial worries (Baum et al., 1999), and is a powerful determinant of health outcomes (Link & Phelan, 2010; Valles, 2018). Bourdieu (1977) argues that the education system reproduces the structural inequalities of society by requiring individuals to understand a cultural code of what is required in order to succeed. While young people from middle class backgrounds may have been taught this code implicitly, young people from less affluent and less educated families may not have these cultural resources. Research suggests that children within the poorest primary schools already have worse mental wellbeing than those in more affluent primary schools, but transitioning to a secondary schools in which others are better off than them is associated with a further negative impact on wellbeing (Moore et al., 2020). As school transition is the point at which young people first experience their new school culture, interventions that can support this process for children from poorer backgrounds have the potential to positively change the mental health and educational trajectories of young people across the life course, while also reducing inequalities. This might be done, for example, by reducing potential mismatch between home and school cultures and giving young people voice and agency in the transition process (Jindal-Snape, 2016).
This systematic review aims to answer three research questions focusing on the evidence of effectiveness of transition interventions across three educational transitions: pre-school settings into first school; school to school transitions (elementary/middle/high school transitions), as well as transitions from high school into post-compulsory education.
Two additional questions were posed in the review protocol (Donaldson et al., 2020) and will be reported elsewhere in due course.
RQ1. Is there evidence that universal interventions, or those focused on young people with low socioeconomic status, are effective in supporting mental health and wellbeing across normative school transitions?
RQ2. Is there evidence of difference in the effectiveness of transition interventions according to their characteristics?
RQ3. How do characteristics of interventions differ by type of school transition?
Method
Eligibility Criteria
Inclusion and exclusion criteria were developed based on extensive scoping searches and informed by the research questions. The population of interest included school pupils from when they entered school (at approximately 4 years of age) until they left school (at approximately 18 years of age). Cohorts where the majority of students were in this age range and not, for example, repeating years, were included. Interventions had to include a quantitative assessment of outcomes and contain at least one universal component or be focused on students of a low socioeconomic status, either due to targeting these students within a school or because the school itself had a lower socioeconomic intake. Studies were included if they sought to improve mental health and wellbeing across transitions between two education settings, either: into school from nursery or pre-school; between schools (e.g. primary to secondary); or from school to post-compulsory education. Interventions could be either side of transition or both sides, and all types of intervention were included, including those that were school-based and/or home-based. They had to include a control group and baseline data had to be collected prior to transition, and prior to the start of the intervention, and at a follow-up point after transition.
The mental health and wellbeing outcomes included were broad and included those alluding to psychological outcomes linked to positive mental health and mental illness, stress, coping and psychological resilience; behavioural outcomes such as conduct disorder, and social outcomes, including social competence and peer relationships (see protocol on PROSPERO for more details). Parent, teacher, child and observer reports were included. There was no restriction on publication date, but papers had to be available in English. Books, dissertations and conference proceedings were excluded, as were interventions focused on non-normative school transitions (e.g. mid-year transfers).
Information Sources
Seven databases (PsycINFO (OVID); EMBASE (OVID), Medline (OVID), ASSIA (Proquest), ERIC (EBSCO Host), Web of Science Core Collection and Scopus) were searched on 5th June 2019. An updated search was conducted on 11th October 2021.
Search Strategy
Search terms were informed by the research questions and developed in Medline based on a combination of: mental health and wellbeing term AND school type adj4 transition AND intervention type, and then adapted for the other six databases. The intervention types were based on the SIGN RCT search filter with some additional terms from the SIGN observational study filter. SIGN filters are pre-tested strategies that identify higher-quality evidence indexed in medical databases (SIGN, 2020). Mental health outcome terms were developed with reference to terms used in other mental health systematic reviews, including Hughes et al. (2013), Wiley et al. (2017) and Stanescu et al. (2019).
Selection Process
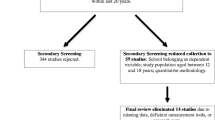
All searches were exported to Endnote (n = 11,531) and deduplicated, leaving 6494 entries. These papers were then exported into Rayyan for title/abstract screening. Title/abstract screening was completed by two reviewers independently of each other, and any disagreements resolved through discussion based on the inclusion criteria. Of the 135 papers put forward for full paper review from database searching, 100 were agreed on by both reviewers independently and a further 35 were identified by just one reviewer and then included following discussion. A further 153 papers that were identified by just one reviewer were excluded from the full paper review following discussion. Therefore of the 135, 74% were identified by both reviewers independently. At this stage of the review, the main reason for papers being excluded was that they were not focused on the right population, either because the population described was not children undergoing an educational transition, or because the intervention presented was not universal but targeted as a subgroup of young people (68.2% of papers excluded). Citation searching was also undertaken to locate additional papers. This resulted in 154 papers for full paper review which was also carried out by two reviewers independently. An additional two papers were added to the systematic review following updated searches in October 2021. In total, 34 papers were included in the review as indicated by the PRISMA flowchart (Page et al., 2021) in Fig. 1.

PRISMA flowchart of study identification, screening and inclusion
Data Collection Process
A data extraction form was developed to capture details of the intervention, sample, mental health measures, data analysis, results, conclusions and limitations from each study. Data were extracted on all follow-up time points post-transition as well as on all measures in each study that fit the inclusion criteria. Where a study presented multiple analyses treating missing data in different ways, data from the model most closely aligned to principles of intention to treat (ITT) were extracted. As-treated data were extracted from papers where no ITT was presented. Due to funding constraints, only one reviewer extracted data from all 34 papers, with a second reviewer independently checking four papers selected at random (12%). There was 100% agreement on the sample checked.
Study Risk of Bias Assessment
The Cochrane Rob2 tool was used to assess risk of bias. The tool includes five domains for RCTs (six for cluster RCTs) that can be used to assess levels of bias (Sterne et al., 2019). The domains are: bias arising from the randomization process; bias due to deviations from intended interventions; bias due to missing outcome data; bias in measurement of the outcome; bias in selection of the reported result, and for cluster RCTs only, bias arising from the timing of identification or recruitment of participants in a cluster-randomized trial. Each domain contains an algorithm based on a series of questions, and the overall rating is based on the highest level of bias in any of the domains. All domains were assessed for the study as a whole, except for in the case of the fourth domain, which assesses bias in the measurement of the outcome, where due to differences in how outcomes were assessed, risk of bias was assessed for each outcome separately.
Study Categorization
Studies were categorized into three ways. Firstly, by type of transition: pre-school to school; school to school; and school to post-compulsory education. Secondly, by length of follow-up period: immediate effects (follow-up < 6 months post-intervention), intermediate effects (follow-up approximately one year post-intervention) and sustained effects (follow-up approximately two or more years post-intervention). Thirdly, studies were categorized by type of intervention. This includes studies with a teacher development component (labelled ‘1’), studies with a parent development component (labelled ‘2’) and those containing ‘other’ activities that were not mediated via teachers or parents (labelled ‘3’). This frequently involved other adults, external to the school or home, facilitating activities directly with the children (including researchers). Within each study, outcomes were categorized as behavioural (including conduct/behavioural problems, aggressive behaviour and externalizing difficulties), emotional/ psychological (including happiness, worry, internalizing behaviour, self-esteem, stress and loneliness), social (including social competence, perceived social support, peer problems and prosocial behaviour) or, where the measure was a combination of these categories, the outcome was categorized as ‘mixed’.
Synthesis of Findings
Due to the heterogeneity in outcome measures and measures of effect, effect direction plots were produced to present intervention effect. In line with recent guidance from Cochrane (Higgins et al., 2021) plots were not based on significance of p-values due to the possibility of underpowered studies being unnecessarily excluded. Firstly, effect directions were calculated for each outcome in each study. Thomson and Thomas (2013) propose that where 70% of outcomes within a study report the same direction of effect, this direction should be reported. Where fewer than 70% of outcomes report the same direction of effect, the results should be stated to be conflicting. The following symbols were used for each paper:
-
▲ Effect direction favours intervention; ▾ Effect direction favours control
-
◄► Effect direction inconsistent or no effect;
-
〇 Insufficient data provided to establish effect direction
The number of assessment measures representing that direction of effect is stated alongside the symbol. Where the insufficient data symbol has been used, this effect direction is not included in the denominator in later discussions about proportions of effect directions operating in a positive or negative direction.
Results
Twenty-four interventions were represented by the 34 included papers. Several interventions had multiple papers relating to them, generally by the same authors or research group, but with different follow-up periods or outcomes. Characteristics of the 34 included studies are presented in Table 1. Tables 2, 3 and 4 provide effect direction plots for each of the interventions, including the types of outcomes assessed in each intervention and the risk of bias assessment. Almost all studies received a risk of bias assessment of high, largely due to missing information about how the interventions were carried out and/or the difficulties of blinding outcome assessors in these types of interventions. Due to lack of power, sign tests (Boon & Thomson, 2021) have not been carried out.
RQ1: Is There Evidence That Universal Interventions, or Those Focused on Young People with Low Socioeconomic Status, are Effective in Supporting Mental Health and Wellbeing Across Normative School Transitions?
Pre-school to Primary School Interventions
This group of papers (n = 21) represented 11 different interventions. All involved children entering school for the first time from a nursery or pre-kindergarten environment at approximately four years of age. Most interventions were based in the USA (n = 9; 82%) and aimed at low SES families (n = 9; 82%). All interventions had a pre-transition component, and five continued post-transition. Interventions were varied in length and scope. Li et al. (2012) focused on preparing children for their new school; over a four-week period children visited their new school, learned how to organise their school bags and participated in a play-based programme to build problem solving, interpersonal and coping skills. Yoshikawa et al. (2015) presented a much more extensive intervention lasting for two years within the school setting involving workshops and in class coaching for teachers in child oral and literacy development, socioemotional development and coordinating education with health services. Six of the 11 interventions (55%) included a component targeting parents—for example, the REDI-P program (Bierman et al., 2015, 2017, 2018, 2019, 2021b) which had children participating in the primarily classroom-focused REDI-C intervention as its control group, involved providing parents with learning materials alongside home visits—and nine out of the 11 (82%) included a component aimed at teachers. Five involved direct interaction with the children from other adults, including research assistants, community volunteers and mental health professionals. For two of the interventions that offered support from mental health professionals, this was a targeted add-on component only for children requiring additional support—the Chicago School Readiness Project (McCoy et al., 2018; Watts et al., 2018; Zhai et al., 2012) and Foundations of Learning (Morris et al., 2010). Follow-up time points ranged from six weeks after the intervention (Li et al., 2012) to 10–11 years later (Watts et al., 2018). Most interventions (n = 10; 91%) had at least an intermediate follow-up period, and four (36%) also had a sustained follow-up. For behavioural outcomes, results were mixed and there is no clear relationship between timing of intervention or intervention type, and direction of effects. For all follow-up timescales, all of the studies that reported a social or mixed outcome reported a positive overall effect direction. The sustained follow-up periods were positive for all reported outcome types.
School to School Transition Interventions
The eight included papers represented seven separate interventions. Four interventions (57%) involved transitions from elementary to middle school at approximately age 11 (Bronstein et al., 1998; Hoglund et al., 2012; Kellam et al., 1994, 1998; Lochman & Wells, 2002); one included an elementary to middle school transition at age 9 (Coelho et al., 2017, 2018) and two included a middle to high school transition at age 14 (Mason et al., 2016). Six of the interventions (86%) had a pre-transition component, and one was solely post-transition. Two interventions (29%)—Coping Power Program (Lochman & Wells, 2002) and Positive Transition (Coelho et al., 2017, 2018)—had pre- and post-transition components. The latter, which look place over a two-year period, included 20*50-min sessions conducted by an educational psychologist. Pre-transition these explored expectations of their the new school, analysis of schedule and evaluation sheets, two sessions conducted by former school colleagues who had already transitioned, and a visit to the middle school. Post-transition, focus was on coping skills and analysing difficulties experienced at transition. Interventions ranged from relatively short in duration—6–8 weeks for Mason et al. (2016)—to WITS which spanned three academic years (Hoglund et al., 2012). WITS was an anti-bullying intervention that provided curricula and online training for teachers, and involved community members, including police officers, emergency service personnel and university athletes, alongside developmental psychologists. Three interventions (43%) aimed to influence teacher behaviour change as a means to influence child mental health outcomes, and four (57%) aimed to help parents to support positive transition. The Coping Power intervention, for example, which had both parent and teacher components included five two-hour teacher training sessions based on identified predictors of substance misuse, including promoting parental involvement in school life and enhancing children’s self-regulation, alongside parent meetings addressing issues relating to their child’s success in school, peer relationships and concerns about the transition to middle school. Of the three interventions with immediate follow-up, all behavioural, emotional and social effect directions were positive except for one which was inconclusive. For the intermediate and sustained follow-ups, the effect directions for the Common Sense Parenting (CSP) and CSP-Plus interventions (Mason et al., 2016) tended to be more negative than those of the other interventions. Overall the pattern seems to show consistent evidence of some immediate effect in the hoped for direction, but less consistent evidence of lasting effect.
Transition to Post-Compulsory Education
Five papers were included in this section and consisted of six interventions. One intervention was for transition from high school to college at age 16 (Vuori et al., 2008) and five (83%) from school to university at age 18. Lamothe et al. (1995), Pratt et al. (2000) and Mattanah et al. (2010) all focused on post-transition interventions based in universities and aimed to increase adolescent social support in order reduce loneliness and increase mental wellbeing. Mattanah et al. (2010), which built on Pratt et al. (2000), included nine weekly peer-led social support groups in the first year of college with discussions on topics related to transition including creating new social ties, peer pressure and residential issues. Quinn et al. (2019) include two (very similar) interventions based in Australian secondary schools. Their primary aim was to target alcohol use and risky party behaviour (such as drug misuse) following school graduation and entry into university. The first intervention was a brief training session on safe partying behaviours, including alcohol harm reduction strategies, mental health and wellbeing tips and the second included similar content but was delivered through a trivia format, informed by social cognitive principles and offered a safe drinking mobile app. Vuori et al. (2008) focused on building career efficacy as young people were leaving Finnish basic education and having to choose vocational or other colleges. It was hypothesized that feeling more in control of their career path would also help reduce depression. None of these interventions had a teacher or parent component. All of these interventions were quite short (ranging from 1.5 h to 9 weeks), and none were aimed at young people from low SES families. None of the interventions were delivered both sides of transition, with three (50%) delivered pre-transition, and three post. For this transition, almost all interventions (n = 5; 83%) had immediate follow-up periods (none had sustained follow-up). Of the four interventions with effect directions available for emotional outcomes, three (75%) had positive effect directions, and of the two with effect directions available for social outcomes, both were positive.
RQ2. Is There Evidence of Difference in the Effectiveness of Transition Interventions According to Their Characteristics?
All studies of interventions using at least a parent and teacher component—coded 1, 2 or 1, 2, 3 in Tables 2, 3 and 4 reported positive overall effect directions, with the exception of intermediate behavioural outcomes in the Parent Corps intervention (Dawson-McClure et al., 2015) which was a school-based intervention providing professional development for teachers in pre-kindergarten and kindergarten on effective behaviour management and positive behaviour support, 13 weekly two-hour sessions for parents and concurrent sessions for pre-kindergarten students led by mental health professionals. However, the findings are too mixed to dismiss or advocate for any intervention type, with many of those with just one intervention component also reporting point estimates in the direction of a positive effect, particularly for school to post-compulsory education transitions. Across all transition types, immediate outcomes were relatively positive overall, particularly for emotional/psychological measures, of which five out of six interventions (83%) reported positive overall effect directions, and for social outcomes, of which four out of five (80%) overall effect directions were positive. For intermediate follow-up, effect directions were more favourable for social outcomes (7/8; 88% are positive) than behavioural (6/12; 50%) or emotional (1/4; 25%). Within the sustained follow-up category, most effect directions were positive for the pre-school to school transition—2/2 (100%) for behavioural outcomes; 2/2 (100%) for emotional outcomes; 2/2 (100%) for social outcomes; and 2/3 (67%) for mixed outcomes. Sustained outcomes for school to school transitions were less favourable, with 1/4 (25%) effect directions positive for behavioural outcomes; 1/1 (100%) positive for emotional outcomes; and 1/3 (33%) for social outcomes.
Across all transition types, very few interventions included in the review were delivered solely post-transition (n = 4; 17%) and there is no clear trend that interventions that run across the transition were more effective than those that were solely pre-transition. There is no clear pattern of effectiveness based on whether interventions were targeted at low SES families or not, although some of the larger interventions, in particular REDI-C and REDI-P (Bierman et al., 2014, 2015, 2017, 2019, 2021a, 2021b; Nix et al., 2013; Welsh et al., 2020), did demonstrate effectiveness across the preschool to school transition for this population. In terms of bias assessment, the larger more extensive interventions also tended to be those more likely to receive a ‘some concerns’ rather than ‘high’ assessment, and there does appear to be a trend that these better quality interventions are more likely to report positive effect estimates.
RQ3. How do Characteristics of Interventions Differ by Type of School Transition?
As children got older, there tended to be a shift from parenting and teacher focused interventions towards those that involved direct interaction with young people and did not rely on behaviour change of parents or teachers to mediate a shift in young people’s outcomes. Pre-school to school interventions were heavily focused on teacher behaviour and moderating the school environment (9/11 interventions; 82%) alongside parenting (5/11; 45%) and child (5/11; 45%) components. The proportion of interventions with a teacher focus had decreased by the primary to secondary transition (3/7; 43%), but more than half of interventions had a parent component (4/7; 57%) and/or a child component (4/7; 57%). By the school to post-compulsory education transition none of the interventions offered parent or teacher components and all focused directly on the adolescent. There was also a shift from focusing on behavioural outcomes at the early transition to more of a focus on psychological outcomes as children age. All but one (91%) of the interventions at the pre-school to school transition included a behavioural outcome and the majority of interventions (64%) included a social outcome; however, only five of the eleven studies (45%) included emotional or psychological outcomes for this age group. For school-to-school transitions, there remained a clear focus on behavioural outcomes, with all interventions bar one (86%) including them as an outcome. Social outcomes were assessed in three of the seven interventions (43%), as were emotional outcomes (43%). At the school to post-compulsory education transition there were no behavioural or mixed outcomes, but five out of six interventions (83%) included emotional/psychological outcomes and three out of six (50%) included social outcomes. Overall, half of interventions were aimed at families with low SES (12/24). This included nearly all pre-school to school transition interventions, but none of the school to post-compulsory education interventions. Just four studies (Hoglund et al., 2012; Kellam et al., 1998; Mason et al., 2016; Watts et al., 2018) looked at SES at either individual or school level as a moderator of intervention impact, with two (Hoglund et al., 2012; Watts et al., 2018), suggesting intervention-generated inequalities may have been introduced.
Discussion
This is the first systematic review to demonstrate the broad scope of mental health and wellbeing interventions across three different educational transitions. Across all types of transition, very few behavioural outcomes were improved by interventions compared to social outcomes, and emotional and psychological outcomes were relatively evenly split between positive and negative effects. Parenting and classroom environment were frequently targeted as a means of improving child outcomes during the earlier transitions, reflecting the important role of parents and teachers in early child development (for example, Daniels & Shumow, 2003; Hernández-Alava & Popli, 2017). Targeting both was generally associated with positive outcomes, consistent with a conclusion that interventions with multiple components are more likely to have positive point estimates. However, the transition to university was associated with more focus on peer relationships, reflecting theoretical perspectives on emerging adulthood and the diminishing role of parents (Arnett, 2000). The aspects of mental health prioritised as intervention outcomes also appeared to shift between different transitions, with greater focus on behavioural outcomes for younger children and psychological outcomes for the transition into post-compulsory education.
Perhaps surprisingly, this review found no evidence that timing of interventions around transition (e.g. pre-transition vs. post-transition vs. pre- and post-transition) was associated with more positive outcomes. It might be expected that interventions that follow children between settings and include components either side of transition would have more positive, sustained outcomes by being able to provide more prolonged targeted support to young people, but this hypothesis was not supported by the evidence available.
Many public health interventions fail to sustain their effects despite initially positive findings (Bailey et al., 2017) and understanding the factors that can reduce fade out is not necessarily straightforward (van Aar et al., 2017). This review found that outcomes assessed two years after the intervention had finished (‘sustained follow-up’) were broadly favourable but fewer in number than those measured within six months of the end of the intervention. While this provides some evidence that fade out was minimized in these interventions, there is also evidence of possible selective reporting as positive outcomes early post-intervention were more frequently followed up in subsequent studies than those that showed no effect.
School readiness at age four, successful transition during adolescence and transition into post-compulsory education are all likely to be more challenging for some children from low socio-economic backgrounds (Camacho et al., 2019; Devlin & McKay, 2014; Jindal-Snape et al., 2020). In line with this established literature on SES differences in school readiness, most pre-school transition interventions targeted low SES families. However, this focus was less apparent for the other two transition types. Few studies assessed socioeconomic gradients in effects within this review, a concern previously reported for school-based health interventions (Moore et al., 2015). Fade out of intervention effects over time may also be more of a concern amongst children from low SES backgrounds, and indicative of the higher number of stressors they experience and lower resources to adapt to them (Pressler et al., 2016). It is therefore important that intervention effects be considered based on child socioeconomic status, both over the short and long term.
This analysis focused on universal interventions, with the exception being interventions focused on children and young people from low SES backgrounds. Many targeted interventions excluded from this review were based on medical diagnoses. Examples of papers that were excluded at the title and abstract screening stage include those focusing on young people with autism (e.g. Mandy et al., 2016; Ong et al., 2012), attention-deficit/hyperactivity disorder (e.g. Sibley et al., 2018), special educational needs (e.g. Bunn & Boesley, 2019; Bunn et al., 2017), developmental disabilities (e.g. McDermott et al., 2018) and diabetes (e.g. Christie et al., 2017). There were also a number of papers with interventions focusing on children in foster care (e.g. Lynch et al., 2017; Pears et al., 2012; Powers et al., 2012). A smaller number of interventions targeted young people based on screening for behavioural and psychological problems (e.g. Bayer et al., 2018; Hart et al., 2016). Future research should consider whether there are particular groups of young people for whom a targeted approach to transition interventions would be more favourable than universal intervention.
Strengths and Limitations
This review has a number of strengths. It fills an important gap in the school health literature by providing systematic, detailed evidence on a broad range of interventions crossing three different educational transitions that have sought to improve mental health outcomes in young people. It highlights the similarities and differences in interventions for transitions at different ages and the important role of parents, teachers and peers in supporting successful transitions.
It also has a number of limitations. It is likely that not all possible papers have been included in this review, not least because some eligible papers are likely not to describe themselves as transition interventions and might therefore have been overlooked by search terms. Of those interventions included, most were based in the USA—just two were in Europe and none were in low-income countries—suggesting limitations to the generalizability of findings and the need for more research into how interventions might support educational transitions in other parts of the world. It was not possible to produce a meta-analysis of findings due to heterogeneity of effect measures used in the interventions (for example, standardized mean difference, Pearson’s r, Cohen’s d, regression coefficients) and insufficient information to convert them to a common measure. The heterogeneity of study designs would also have made a meta-analysis inappropriate. Thus, in order to use quantitative evidence of effectiveness and compare studies with different effect measures, effect direction plots were used in the current study. The use of effect direction plots underlines the move away from the reliance on p values in estimating effects (Wasserstein et al., 2019) and can help to ensure that underpowered studies are not excluded from evidence. However, it may mean that very small changes from the mean may be misidentified as effects rather than noise, and this is particularly an issue when reviews only have a small number of studies because any misidentified effects may not balance out.
Not all of the transitions included, particularly in preschool to school category, necessarily involved a change of school and this was not always clear from the papers. Studies were included irrespective of whether the transition involved a physical move. This broad theme of the difficulties of comparing very different interventions is apparent across the review and makes direct comparison difficult.
Finally, assessing risk of bias was problematic. In interventions where blinding of participants is not possible and where outcomes pertain to the lived experience of mental health, the high risk of bias associated with self-reporting is not fixable. Even where interventions used other outcome assessors and the papers stated that assessors were naïve to treatment group, the RoB2 guidelines states that “if either the participant is blinded and the data collector is not, or the data collector is blinded and the participant is not, then the outcome assessors should be considered to be aware of intervention received unless convincing evidence is available to the contrary” (Higgins et al., 2019, p .52). This resulted in many studies receiving high risk of bias categorization and none receiving low risk.
Future Research and Conclusion
Educational transitions can be important turning points in the lives of young people, and for those young people who experience a poor transition, this can influence their academic and health trajectories for the rest of their lives. Intervening to improve transition experiences can support young people, particularly those at risk of poor transition, and prevent them from disengaging from academic life and support their mental health. Future research should aim to better understand how different intervention theories lead to less or more positive effects to support identification of transferable intervention mechanisms and specifically those that do not exacerbate inequalities for young people from low SES backgrounds. Secondly, many young people, particularly those most vulnerable and from the most disadvantaged backgrounds, will experience a transition to work rather than post-compulsory education when they finish school. Future research should consider young people who move onto work rather than university, and the types of interventions that might be best suited to support this transition. Finally, young people in different countries experience school transitions at different ages and the social and political context of the transition can vary widely. Even within this review, the range of ages included with the school to school transition category ranged from age 9 to 14, and transition is likely to be experienced very differently at these ages (Bagnall et al., 2021). These differences should be further explored in subsequent research to understand how interventions can best address these age differences.
References
Aina, C., Baici, E., Casalone, G., & Pastore, F. (2022). The determinants of university dropout: A review of the socio-economic literature. Socio-Economic Planning Sciences, 79(February), 101102. https://doi.org/10.1016/j.seps.2021.101102
Arnett, J. J. (2000). Emerging adulthood: A theory of development from the late teens through the twenties. American Psychologist, 55(5), 469–480. https://doi.org/10.1037/0003-066X.55.5.469
Bagnall, C. L., Fox, C. L., & Skipper, Y. (2021). When is the ‘optimal’ time for school transition? An insight into provision in the US. Pastoral Care in Education, 39(4), 348–376. https://doi.org/10.1080/02643944.2020.1855669
Bailey, D., Duncan, G. J., Odgers, C. L., & Yu, W. (2017). Persistence and fadeout in the impacts of child and adolescent interventions. Journal of Research on Educational Effectiveness, 10(1), 7–39. https://doi.org/10.1080/19345747.2016.1232459
Baum, A., Garofalo, J. P., & Yali, A. M. (1999). Socioeconomic status and chronic stress. Does stress account for SES effects on health? Annals of the New York Academy of Sciences, 896, 131–144. https://doi.org/10.1111/j.1749-6632.1999.tb08111.x
Bayer, J. K., Beatson, R., Bretherton, L., Hiscock, H., Wake, M., Gilbertson, T., Mihalopoulos, C., Prendergast, L. A., & Rapee, R. M. (2018). Translational delivery of Cool Little Kids to prevent child internalising problems: Randomised controlled trial. Australian and New Zealand Journal of Psychiatry, 52(2), 181–191. https://doi.org/10.1177/0004867417726582
Bayer, J. K., Ukoumunne, O. C., Mathers, M., Wake, M., Abdi, N., & Hiscock, H. (2012). Development of children’s internalising and externalising problems from infancy to five years of age. Australian and New Zealand Journal of Psychiatry, 46(7), 659–668. https://doi.org/10.1177/0004867412450076
Bierman, K. L., Heinrichs, B. S., Welsh, J. A., & Nix, R. L. (2021a). Reducing adolescent psychopathology in socioeconomically disadvantaged children with a preschool intervention: A randomized controlled trial. American Journal of Psychiatry, 178(4), 305–312. https://doi.org/10.1176/appi.ajp.2020.20030343
Bierman, K. L., Heinrichs, B. S., Welsh, J. A., & Nix, R. L. (2021b). Sustained benefits of a preschool home visiting program: Child outcomes in fifth grade. Early Childhood Research Quarterly, 56, 260–271. https://doi.org/10.1016/j.ecresq.2021.03.017
Bierman, K. L., Heinrichs, B. S., Welsh, J. A., Nix, R. L., & Gest, S. D. (2017). Enriching preschool classrooms and home visits with evidence-based programming: Sustained benefits for low-income children. Journal of Child Psychology and Psychiatry and Allied Disciplines, 58(2), 129–137. https://doi.org/10.1111/jcpp.12618
Bierman, K. L., McDoniel, M. E., & Loughlin-Presnal, J. E. (2019). How a preschool parent intervention produced later benefits: A longitudinal mediation analysis. Journal of Applied Developmental Psychology, 64, 101058. https://doi.org/10.1016/j.appdev.2019.101058
Bierman, K. L., Nix, R. L., Heinrichs, B. S., Domitrovich, C. E., Scott, D., Welsh, J. A., & Gill, S. (2014). Effects of head start REDI on children’s outcomes 1 year later in different kindergarten contexts. Child Development, 85(1), 140–159. https://doi.org/10.1111/cdev.12117
Bierman, K. L., Welsh, J., Heinrichs, B. S., & Nix, R. L. (2018). Effect of preschool home visiting on school readiness and need for services in elementary school a randomized clinical trial. JAMA Pediatrics, 172(8), 1–7. https://doi.org/10.1001/jamapediatrics.2018.1029
Bierman, K. L., Welsh, J. A., Heinrichs, B. S., Nix, R. L., & Mathis, E. T. (2015). Helping Head Start parents promote their children’s kindergarten adjustment: The research-based developmentally informed parent program. Child Development, 86(6), 1877–1891. https://doi.org/10.1111/cdev.12448
Bonell, C. P., Fletcher, A., Jamal, F., Wells, H., Harden, A., Murphy, S., & Thomas, J. (2013). Theories of how the school environment impacts on student health: Systematic review and synthesis. Health and Place, 24, 242–249. https://doi.org/10.1016/j.healthplace.2013.09.014
Boon, M. H., & Thomson, H. (2021). The effect direction plot revisited: Application of the 2019 Cochrane Handbook guidance on alternative synthesis methods. Research Synthesis Methods, 12(1), 29–33. https://doi.org/10.1002/jrsm.1458
Bourdieu, P. (1977). Cultural reproduction and social reproduction. In J. Karabel & A. H. Halsey (Eds.), Power and ideology in education (pp. 487–551). Oxford University Press.
Bronstein, P., Duncan, P., Abrams, C. L., Yannett, N., Ginsburg, G., & Milne, M. (1998). Preventing middle school adjustment problems for children from lower-income families: A program for aware parenting. Journal of Applied Developmental Psychology, 19(1), 129–152. https://doi.org/10.1016/S0193-3973(99)80032-X
Brotman, L. M., Dawson-McClure, S., Kamboukos, D., Huang, K. Y., Calzada, E. J., Goldfeld, K., & Petkova, E. (2016). Effects of Parentcorps in prekindergarten on child mental health and academic performance follow-up of a randomized clinical trial through 8 years of age. JAMA Pediatrics, 170(12), 1149–1155. https://doi.org/10.1001/jamapediatrics.2016.1891
Bunn, H., & Boesley, L. (2019). My New School: Transition to high school for children with special educational needs in England—Findings and ideas for practice. Support for Learning, 34(2), 128–147. https://doi.org/10.1111/1467-9604.12244
Bunn, H., Davis, D., & Speed, E. (2017). High school transition—An intervention that empowers children with special educational needs and improves school practice. Support for Learning, 32(3), 231–244. https://doi.org/10.1111/1467-9604.12167
Camacho, C., Straatmann, V. S., Day, J. C., & Taylor-Robinson, D. (2019). Development of a predictive risk model for school readiness at age 3 years using the UK Millennium Cohort Study. British Medical Journal Open, 9(6), 1–11. https://doi.org/10.1136/bmjopen-2018-024851
Christie, D., Ali, S., Flannery, H., & Casdagli, L. (2017). GReaT groups (getting ready for transition): Supporting transition to secondary school for children and parents living with diabetes. Journal of Adolescent Health, 60(2), S39-40. https://doi.org/10.1016/j.jadohealth.2016.10.261
Coelho, V. A., Marchante, M., & Jimerson, S. R. (2017). Promoting a positive middle school transition: A randomized-controlled treatment study examining self-concept and self-esteem. Journal of Youth and Adolescence, 46(3), 558–569. https://doi.org/10.1007/s10964-016-0510-6
Coelho, V. A., Sousa, V., & Marchante, M. (2018). Positive transition to middle school: A multilevel model analysis of a Portuguese school adjustment program. Journal of Positive Behavior Interventions, 20(3), 160–171. https://doi.org/10.1177/1098300717750872
Comeau, J., & Boyle, M. H. (2018). Patterns of poverty exposure and children’s trajectories of externalizing and internalizing behaviors. SSM Population Health, 4, 86–94. https://doi.org/10.1016/j.ssmph.2017.11.012
Crosnoe, R., & Ansari, A. (2016). Family socioeconomic status, immigration, and children’s transitions into school. Family Relations, 65(1), 73–84. https://doi.org/10.1111/fare.12171
Daniels, D. H., & Shumow, L. (2003). Child development and classroom teaching: A review of the literature and implications for educating teachers. Journal of Applied Developmental Psychology, 23(5), 495–526. https://doi.org/10.1016/S0193-3973(02)00139-9
Dawson-McClure, S., Calzada, E., Huang, K. Y., Kamboukos, D., Rhule, D., Kolawole, B., Petkova, E., & Brotman, L. M. (2015). A population-level approach to promoting healthy child development and school success in low-income, urban neighborhoods: Impact on parenting and child conduct problems. Prevention Science, 16(2), 279–290. https://doi.org/10.1007/s11121-014-0473-3
Devlin, M., & McKay, J. (2014). Reframing ‘the problem’: Students from low socio-economic status backgrounds transitioning to university. In H. Brook, D. Fergie, M. Maeorg, & D. Michell (Eds.), Universities in Transition: Foregrounding social contexts of knowledge in the first year experience (pp. 97–125). The University of Adelaide Press.
Donaldson, C., Moore, G., & Hawkins, J. (2020). The effectiveness of universal school transition interventions for mental health and wellbeing outcomes in children and young people: A systematic review. PROSPERO 2020 CRD42020176336. https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020176336
Duncan, G. J., Dowsett, C. J., Claessens, A., Magnuson, K., Huston, A. C., Klebanov, P., Pagani, L. S., Feinstein, L., Engel, M., Brooks-Gunn, J., Sexton, H., Duckworth, K., & Japel, C. (2007). School readiness and later achievement. Developmental Psychology, 43(6), 1428–1446. https://doi.org/10.1037/0012-1649.43.6.1428
Gallo, L. C., De Los, E., Monteros, K., & Shivpuri, S. (2009). Socioeconomic status and health: What is the role of reserve capacity? Current Directions in Psychological Science, 18(5), 269–274. https://doi.org/10.1111/j.1467-8721.2009.01650.x
Gazelle, H., & Faldowski, R. A. (2019). Multiple trajectories in anxious solitary youths: The middle school transition as a turning point in development. Journal of Abnormal Child Psychology, 47(7), 1135–1152. https://doi.org/10.1007/s10802-019-00523-8
Gotlib, I. H., & Blair, W. (1997). Stress and adversity over the life course: trajectories and turning points. Cambridge University Press.
Gregory, T., Dal Grande, E., Brushe, M., Engelhardt, D., Luddy, S., Guhn, M., Gadermann, A., Schonert-Reichl, K. A., & Brinkman, S. (2021). Associations between school readiness and student wellbeing: A six-year follow up study. Child Indicators Research, 14(1), 369–390. https://doi.org/10.1007/s12187-020-09760-6
Hart, K. C., Graziano, P. A., Kent, K. M., Kuriyan, A., Garcia, A., Rodriguez, M., & Pelham, W. E. (2016). Early intervention for children with behavior problems in summer settings. Journal of Early Intervention, 38(2), 92–117. https://doi.org/10.1177/1053815116645923
Hernández-Alava, M., & Popli, G. (2017). Children’s development and parental input: Evidence from the UK Millennium Cohort Study. Demography, 54(2), 485–511. https://doi.org/10.1007/s13524-017-0554-6
Higgins, J., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M., & Welch, V. (Eds.). (2021). Cochrane handbook for systematic reviews of interventions version 6.3 (updated February 2022). Cochrane. www.training.cochrane.org/handbook.
Higgins, J. P., Savovic, J., Page, M. J., & Sterne, J. A. (2019). Revised Cochrane risk-of-bias tool for randomized trials (RoB 2). https://drive.google.com/file/d/19R9savfPdCHC8XLz2iiMvL_71lPJERWK/view
Hoglund, W. L. G., Hosan, N. E., & Leadbeater, B. J. (2012). Using your wits: A 6-year follow-up of a peer victimization prevention program. School Psychology Review, 41(2), 193–214. https://doi.org/10.1080/02796015.2012.12087520
Hughes, L. A., Banks, P., & Terras, M. M. (2013). Secondary school transition for children with special educational needs: A literature review. Support for Learning, 28(1), 24–34. https://doi.org/10.1111/1467-9604.12012
Ibrahim, A. K., Kelly, S. J., Adams, C. E., & Glazebrook, C. (2013). A systematic review of studies of depression prevalence in university students. Journal of Psychiatric Research, 47(3), 391–400. https://doi.org/10.1016/j.jpsychires.2012.11.015
Jacob, C. M., Hardy-Johnson, P. L., Inskip, H. M., Morris, T., Parsons, C. M., Barrett, M., Hanson, M., Woods-Townsend, K., & Baird, J. (2021). A systematic review and meta-analysis of school-based interventions with health education to reduce body mass index in adolescents aged 10 to 19 years. International Journal of Behavioral Nutrition and Physical Activity, 18(1), 1–22. https://doi.org/10.1186/s12966-020-01065-9
Jindal-Snape, D. (2016). A-Z of transitions. Palgrave.
Jindal-Snape, D., Hannah, E. F. S., Cantali, D., Barlow, W., & MacGillivray, S. (2020). Systematic literature review of primary-secondary transitions: International research. Review of Education, 8(2), 526–566. https://doi.org/10.1002/rev3.3197
Kellam, S. G., Rebok, G. W., Ialongo, N., & Mayer, L. S. (1994). The course and malleability of aggressive behavior from early first grade into middle school: Results of a developmental epidemiologically-based preventive trial. Journal of Child Psychology and Psychiatry and Allied Disciplines, 35(2), 259–281. https://doi.org/10.1111/j.1469-7610.1994.tb02308.x
Kellam, S. G., Ling, X., Merisca, R., Brown, C. H., & Ialongo, N. (1998). The effect of the level of aggression in the first grade classroom on the course and malleability of aggressive behavior into middle school. Development and Psychopathology, 10(2), 165–185. https://doi.org/10.1017/s0954579400001073
Kroshus, E., Hawrilenko, M., & Browning, A. (2021). Stress, self-compassion, and well-being during the transition to college. Social Science and Medicine, 269, 113514. https://doi.org/10.1016/j.socscimed.2020.113514
Lamothe, D., Currie, F., Alisat, S., Sullivan, T., Pratt, M., Pancer, S. M., & Hunsberger, B. (1995). Impact of a social support intervention on the transition to university. Canadian Journal of Community, 14(2), 167–180. https://doi.org/10.7870/cjcmh-1995-0023
Langford, R., Bonell, C., Jones, H., Pouliou, T., Murphy, S., Waters, E., Komro, K., Gibbs, L., Magnus, D., & Campbell, R. (2015). The World Health Organization’s Health Promoting Schools framework: A Cochrane systematic review and meta-analysis. BMC Public Health, 15(1), 1–15. https://doi.org/10.1186/s12889-015-1360-y
Larose, S., Duchesne, S., Litalien, D., Denault, A. S., & Boivin, M. (2019). Adjustment trajectories during the college transition: types, personal and family antecedents, and academic outcomes. Research in Higher Education, 60(5), 684–710. https://doi.org/10.1007/s11162-018-9538-7
Li, M., Johnson, S. B., Musci, R. J., & Riley, A. W. (2017). Perceived neighborhood quality, family processes, and trajectories of child and adolescent externalizing behaviors in the United States. Social Science and Medicine, 192, 152–161. https://doi.org/10.1016/j.socscimed.2017.07.027
Li, W. H. C., Mak, Y. W., Chan, S. S. C., Chu, A. K. Y., Lee, E. Y., & Lam, T. H. (2012). Effectiveness of a play-integrated primary one preparatory programme to enhance a smooth transition for children. Journal of Health Psychology, 18(1), 10–25. https://doi.org/10.1177/1359105311434052
Link, B., & Phelan, J. (2010). Social conditions as fundamental causes of health inequalities. In C. E. Bird (Ed.), Handbook of Medical Sociology (pp. 1–17). Vanderbilt University Press.
Lochman, J. E., & Wells, K. C. (2002). The coping power program at the middle-school transition: Universal and indicated prevention effects. Psychology of Addictive Behaviors, 16(4), S40–S54. https://doi.org/10.1037/0893-164x.16.4s.s40
Lynch, F. L., Dickerson, J. F., Pears, K. C., & Fisher, P. A. (2017). Cost effectiveness of a school readiness intervention for foster children. Children and Youth Services Review, 81, 63–71. https://doi.org/10.1016/j.childyouth.2017.07.011
Mandy, W., Murin, M., Baykaner, O., Staunton, S., Cobb, R., Hellriegel, J., Anderson, S., & Skuse, D. (2016). Easing the transition to secondary education for children with autism spectrum disorder: An evaluation of the systemic transition in education programme for autism spectrum disorder (STEP-ASD). Autism, 20(5), 580–590. https://doi.org/10.1177/1362361315598892
Mantzicopoulos, P. (2004). The effects of participation in a head start-public school transition program on kindergarten children’s social competence. Perspectives in Education, 22(2), 51–66.
Mason, W. A., Fleming, C. B., Gross, T. J., Thompson, R. W., Parra, G. R., Haggerty, K. P., & Snyder, J. J. (2016). Randomized trial of parent training to prevent adolescent problem behaviors during the high school transition. Journal of Family Psychology, 30(8), 944–954. https://doi.org/10.1037/fam0000204
Mattanah, J. F., Brooks, L. J., Ayers, J. F., Quimby, J. L., Brand, B. L., & McNary, S. W. (2010). A social support intervention to ease the college transition: Exploring main effects and moderators. Journal of College Student Development, 51(1), 93–108. https://doi.org/10.1353/csd.0.0116
McCoy, D. C., Jones, S., Roy, A., & Raver, C. C. (2018). Classifying trajectories of social-emotional difficulties through elementary school: Impacts of the chicago school readiness project. Developmental Psychology, 54(4), 772–787. https://doi.org/10.1037/dev0000457
McDermott, J. M., Pears, K. C., Bruce, J., Kim, H. K., Roos, L., Yoerger, K. L., & Fisher, P. A. (2018). Improving kindergarten readiness in children with developmental disabilities: Changes in neural correlates of response monitoring. Applied Neuropsychology: Child, 7(3), 187–199. https://doi.org/10.1080/21622965.2017.1286239
Moore, G., Angel, L., Brown, R., van Godwin, J., Hallingberg, B., & Rice, F. (2021). Socio-economic status, mental health difficulties and feelings about transition to secondary school among 10–11 year olds in Wales: Multi-level analysis of a cross sectional survey. Child Indicators Research, 14(4), 1597–1615. https://doi.org/10.1007/s12187-021-09815-2
Moore, G. F., Anthony, R., Hawkins, J., Van Godwin, J., Murphy, S., Hewitt, G., & Melendez-Torres, G. (2020). Socioeconomic status, mental wellbeing and transition to secondary school: Analysis of the School Health Research Network/Health Behaviour in School-aged Children survey in Wales. British Educational Research Journal, 46(5), 1111–1130. https://doi.org/10.1002/berj.3616
Moore, G. F., Littlecott, H. J., Turley, R., Waters, E., & Murphy, S. (2015). Socioeconomic gradients in the effects of universal school-based health behaviour interventions: A systematic review of intervention studies. BMC Public Health, 15, 907. https://doi.org/10.1186/s12889-015-2244-x
Morris, P., Raver, C. C., Millenky, M., & Lloyd, C. M. (2010). Making preschool more productive: How classroom management training can help teachers. MDRC.
Nix, R. L., Bierman, K. L., Domitrovich, C. E., & Gill, S. (2013). Promoting children’s social-emotional skills in preschool can enhance academic and behavioral functioning in kindergarten: Findings from Head Start REDI. Early Education and Development, 24(7), 1–21. https://doi.org/10.1080/10409289.2013.825565
Ong, C., Foo, S., & Chong, S. (2012). Adaptation of children with autism to Singapore mainstream primary schools: A study on the effectiveness of the S.T.A.R.S (successful transition, adaptation, readiness skills) transition program. Neuropsychiatrie De L’enfance Et De L’adolescence, 60(5), S211. https://doi.org/10.1016/J.NEURENF.2012.04.448
Page, M. J., Mckenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., Shamseer, L., Tetzlaff, J. M., Akl, E. A., Brennan, S. E., Chou, R., Glanville, J., Grimshaw, J. M., Hróbjartsson, A., Lalu, M. M., Li, T., Loder, E. W., Mayo-Wilson, E., Mcdonald, S., et al. (2021). The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ, 372, 71. https://doi.org/10.1136/bmj.n71
Pan, Q., Trang, K. T., Love, H. R., & Templin, J. (2019). School readiness profiles and growth in academic achievement. Frontiers in Education, 4, 127. https://doi.org/10.3389/feduc.2019.00127
Pears, K. C., Kim, H. K., & Fisher, P. A. (2012). Effects of a school readiness intervention for children in foster care on oppositional and aggressive behaviors in kindergarten. Child Youth Services Review, 34(12), 2361–2366. https://doi.org/10.1016/j.childyouth.2012.08.015
Phelan, J. C., Link, B. G., & Tehranifar, P. (2010). Social conditions as fundamental causes of health inequalities: Theory, evidence, and policy implications. Journal of Health and Social Behavior, 51(1), S28–S40. https://doi.org/10.1177/0022146510383498
Powers, L. E., Geenen, S., Powers, J., Pommier-Satya, S., Turner, A., Dalton, L. D., Drummond, D., & Swank, P. (2012). My Life: Effects of a longitudinal, randomized study of self-determination enhancement on the transition outcomes of youth in foster care and special education. Children and Youth Services Review, 34(11), 2179–2187. https://doi.org/10.1016/j.childyouth.2012.07.018
Pratt, M. W., Hunsberger, B., Pancer, S. M., Alisat, S., Bowers, C., Mackey, K., Ostaniewicz, A., Rog, E., Terzian, B., & Thomas, N. (2000). Facilitating the transition to university: Evaluation of a social support discussion intervention program. Journal of College Student Development, 41(4), 427–441.
Pressler, E., Raver, C. C., Friedman-Krauss, A. H., & Roy, A. (2016). The roles of school readiness and poverty-related risk for 6th grade outcomes. Journal of Educational and Developmental Psychology, 6(1), 140–156. https://doi.org/10.5539/jedp.v6n1p140
Quinn, C. A., Hides, L., de Andrade, D., Pocuca, N., Wilson, M., & Kavanagh, D. J. (2019). Impact of a brief psychoeducational intervention for reducing alcohol use and related harm in school leavers. Drug and Alcohol Review, 38(4), 339–348. https://doi.org/10.1111/dar.12920
Rose, G. (2001). Sick individuals and sick populations. International Journal of Epidemiology, 30(3), 427–432. https://doi.org/10.1093/ije/30.3.427
Roy, A. L., & Raver, C. C. (2014). Are all risks equal? Early experiences of poverty-related risk and children’s functioning. Journal of Family Psychology, 28(3), 391–400. https://doi.org/10.1037/a0036683.Are
Shackleton, N., Jamal, F., Viner, R. M., Dickson, K., Patton, G., & Bonell, C. (2016). School-based interventions going beyond health education to promote adolescent health: Systematic review of reviews. Journal of Adolescent Health, 58(4), 382–396. https://doi.org/10.1016/j.jadohealth.2015.12.017
Shure, M. B., & Spivack, G. (1982). Interpersonal problem-solving in young children: A cognitive approach to prevention. American Journal of Community, 10(3), 341–356.
Sibley, M. H., Coxe, S. J., Campez, M., Morley, C., Olson, S., Hidalgo-Gato, N., Gnagy, E., Greiner, A., Coles, E. K., Page, T., & Pelham, W. E. (2018). High versus low intensity summer treatment for ADHD delivered at secondary school transitions. Journal of Clinical Child and Adolescent Psychology, 47(2), 248–265. https://doi.org/10.1080/15374416.2018.1426005
SIGN. (2020). SIGN search filters. https://www.sign.ac.uk/what-we-do/methodology/search-filters/
Sirsch, U. (2003). The impending transition from primary to secondary school: Challenge or threat? International Journal of Behavioral Development, 27(5), 385–395. https://doi.org/10.1080/01650250344000082
Stanescu, S., Kirby, S. E., Thomas, M., Yardley, L., & Ainsworth, B. (2019). A systematic review of psychological, physical health factors, and quality of life in adult asthma. Npj Primary Care Respiratory Medicine, 29, 37. https://doi.org/10.1038/s41533-019-0149-3
Sterne, J. A. C., Savović, J., Page, M. J., Elbers, R. G., Blencowe, N. S., Boutron, I., Cates, C. J., Cheng, H. Y., Corbett, M. S., Eldridge, S. M., Emberson, J. R., Hernán, M. A., Hopewell, S., Hróbjartsson, A., Junqueira, D. R., Jüni, P., Kirkham, J. J., Lasserson, T., Li, T., et al. (2019). RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ, 366, I4898. https://doi.org/10.1136/bmj.l4898
Symonds, J. (2015). Understanding school transition: What happens to children and how to help them. Routledge.
Taylor, S. E., & Broffman, J. I. (2011). Psychosocial resources. Functions, origins, and links to mental and physical health. Advances in Experimental Social Psychology, 44, 1–57. https://doi.org/10.1016/B978-0-12-385522-0.00001-9
Thomson, H. J., & Thomas, S. (2013). The effect direction plot: Visual display of non-standardised effects across multiple outcome domains. Research Synthesis Methods, 4(1), 95–101. https://doi.org/10.1002/jrsm.1060
Valles, S. A. (2018). Philosophy of population health: Philosophy for a new public health era. Routledge.
van Aar, J., Leijten, P., Orobio de Castro, B., & Overbeek, G. (2017). Sustained, fade-out or sleeper effects? A systematic review and meta-analysis of parenting interventions for disruptive child behavior. Clinical Psychology Review, 51, 153–163. https://doi.org/10.1016/j.cpr.2016.11.006
Vuori, J., Koivisto, P., Mutanen, P., Jokisaari, M., & Salmela-Aro, K. (2008). Towards working life: Effects of an intervention on mental health and transition to post-basic education. Journal of Vocational Behavior, 72(1), 67–80. https://doi.org/10.1016/j.jvb.2007.10.003
Wasserstein, R. L., Schirm, A. L., & Lazar, N. A. (2019). Moving to a world beyond ‘p<0.05.’ The American Statistician, 73(S1), 1–19. https://doi.org/10.1080/00031305.2019.1583913
Watts, T. W., Gandhi, J., Ibrahim, D. A., Masucci, M. D., & Cybele Raver, C. (2018). The Chicago school readiness project: Examining the long-term impacts of an early childhood intervention. PLoS ONE, 13(7), 1–25. https://doi.org/10.1371/journal.pone.0200144
Webster-Stratton, C. (1998). Preventing conduct problems in head start children: Strengthening parenting competencies. Journal of Consulting and Clinical Psychology, 66(5), 715–730. https://doi.org/10.1037/0022-006X.66.5.715
Webster-Stratton, C., Reid, M. J., Hammond, M., Webster-stratton, C., Reid, M. J., & Hammond, M. (2001). Preventing conduct problems, promoting social competence: A parent and teacher training partnership in Head Start. Journal of Clinical Child & Adolescent Psychology, 30(3), 283–302. https://doi.org/10.1207/S15374424JCCP3003
Welsh, J. A., Bierman, K. L., Nix, R. L., & Heinrichs, B. N. (2020). Sustained effects of a school readiness intervention: 5th grade outcomes of the Head Start REDI program. Early Childhood Research Quarterly, 53, 151–160. https://doi.org/10.1016/j.ecresq.2020.03.009
Wiley, J. F., Bei, B., Bower, J. E., & Stanton, A. L. (2017). Relationship of psychosocial resources with allostatic load: A systematic review. Psychosomatic Medicine, 79(3), 283–292. https://doi.org/10.1097/PSY.0000000000000395
Yoshikawa, H., Leyva, D., Snow, C. E., Treviño, E., Clara Barata, M., Weiland, C., Gomez, C. J., Moreno, L., Rolla, A., D’Sa, N., & Arbour, M. C. (2015). Experimental impacts of a teacher professional development program in Chile on preschool classroom quality and child outcomes. Developmental Psychology, 51(3), 309–322. https://doi.org/10.1037/a0038785
Zhai, F., Raver, C. C., & Jones, S. M. (2012). Academic performance of subsequent schools and impacts of early interventions: Evidence from a randomized controlled trial in Head Start settings. Children and Youth Services Review, 34(5), 946–954. https://doi.org/10.1016/j.childyouth.2012.01.026
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
This work was funded through an Economic and Social Research Council PhD Studentship (C. Donaldson). It was supported by the Centre for Development, Evaluation, Complexity and Implementation in Public Health Improvement, which is funded by Welsh Government through Health and Care Research Wales. The research was also supported by the Wolfson Centre for Young People’s Mental Health, established with a grant from the Wolfson Foundation. No other funding was received to assist with the preparation of this manuscript. All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript. Open Access Statement: No new data was created during this study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Donaldson, C., Moore, G. & Hawkins, J. A Systematic Review of School Transition Interventions to Improve Mental Health and Wellbeing Outcomes in Children and Young People. School Mental Health 15, 19–35 (2023). https://doi.org/10.1007/s12310-022-09539-w
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12310-022-09539-w