
Abstract
Depression and anxiety are common mental health problems that negatively affect the quality of life. Functioning, social relationships, daily activities, and physical health are negatively affected. Therefore, it is very important to manage these problems and to investigate effective treatments for individuals to lead a healthy life. This study aims to evaluate the effect of hydrotherapy and balneotherapy on anxiety and depression. Randomized controlled trials published in the last 20 years comparing hydrotherapy and balneotherapy with active control or waiting lists in adults with anxiety and depressive symptoms were included. Pubmed, Cochrane, Scopus, Web of Science, and CINAHL databases were searched until August 2023. The random effects model and fixed effects model were used for data analysis. The heterogeneity of the study was assessed using the I2 index, and publication bias was assessed using Egger and Begg tests and funnel plots. Seventeen eligible studies with a sample size of 977 participants were selected. After data analysis, the results showed that hydrotherapy and balneotherapy led to a statistically significant reduction in anxiety scores (SMD: 0.46 95% CI: 0.27, 0.65), depression scores (SMD: 0.53 95% CI: 0.38, 0.67). Subgroup analysis based on intervention type showed that balneotherapy reduced anxiety scores (SMD: 0.46, 95% CI: 0.27, 0.65) but not depression scores. Evidence suggests that hydrotherapy and balneotherapy can reduce anxiety and depression in adults. Based on these findings, hydrotherapy and balneotherapy can be applied as an adjunct to standard treatments to improve the mental health of adults.
Registration: The study protocol was registered in the International Register of Prospective Systematic Reviews (PROSPERO) with accession number CRD42023448993.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Mental disorders are leading determinants of global health. According to The Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2019 data, depression and anxiety are the most common mental disorders that cause disability (GBD 2019 Diseases and Injuries Collaborators, 2020; GBD 2019 Fracture Collaborators, 2021). Depression and anxiety lead to decreased quality of life, increased suicide risk, and worsening physical health (Ribeiro et al., 2020; Zhang et al., 2019). Anxiety and depression have been a major concern due to their negative effects and the focus has been on their effective treatment. Treatment options such as pharmacotherapy, psychotherapy, and a combination of psychotherapy and medication are available to improve symptoms of anxiety and depression (Bandelow et al., 2017). An important limitation of psychotherapy is the insufficient number of psychotherapists and high treatment costs in low-income countries (Bernhardt et al., 2019). Psychotherapies can create stigmatization, and prejudice or increase client self-hatred (Dimidjian & Hollon, 2010). Anxiolytics and antidepressants cause physical effects such as weight gain, gastrointestinal and sexual difficulties, insomnia, severe headaches, and drowsiness, which negatively affect patient compliance with treatment (Uzbay & Yüksel, 2002). However, hydrotherapy and balneotherapy applications are very attractive because they do not require chemicals or drugs. These treatments, which have minimal side effects, have low risks for the general health and well-being of patients (Cacciapuoti et al., 2020).
Hydrotherapy aims to treat by utilizing the physical properties of water such as temperature, hydrostatic pressure, viscosity, and electrical conductivity. In hydrotherapy, plain water is used internally and externally. (Reger et al., 2022). Hydrotherapy is used to protect and improve physical and mental health. Applications such as sitting baths, whirlpool baths, irrigation systems, butterfly baths (hubbarda tank), aqua therapy, halliwick, bad ragaz ring method, and watsu are considered within the scope of hydrotherapy (Genç & Deveci, 2023). Immersion in warm water reduces sympathetic nervous system activation and increases parasympathetic nervous system activation. This effect elicits a relaxation response and reduces anxiety (Becker, 2009). Castro-Sánchez et al. revealed that 40 sessions of Ai-Chi exercise showed significant improvements in depression scores of multiple sclerosis patients (Castro-Sánchez et al., 2012). In studies examining the effect of hydrotherapy on anxiety and depression for different diseases in the literature, it was determined that it reduced anxiety and depression (Latorre-Román et al., 2015; Dinç Yavaş et al., 2021).
Another therapy that affects the level of anxiety and depression of individuals is balneotherapy. There are many balneological applications in spas. Balneotherapy is among the most commonly used treatment methods. Balneotherapy is defined as the use of baths (in bathtubs or pools) containing thermal mineral water from natural sources, with a temperature of at least 20 °C and mineral content of at least 1 g/L, and is applied as a cure (Fioravanti et al., 2017; Karagülle & Karagülle, 2015). The fact that balneotherapy is applied in the form of a cure makes hot springs an ideal environment not only for physical health but also for mental health by getting away from the stress and fatigue of daily life. It is used not only for the treatment of diseases but also by many people who want to live a healthy life and slow down aging (Özkuk et al., 2018). Dubois et al. investigated the efficacy of balneotherapy against paroxetine, a selective serotonin reuptake inhibitor, in patients with a generalized anxiety disorder (GAD). As a result of the study, it was found that the change in anxiety scores of balneotherapy patients was more advantageous (Dubois et al., 2010). The effect of spa treatments on salivary cortisol levels, which is considered as a stress marker, was examined, and it was reported that spa treatments have the potential to affect salivary cortisol levels in healthy or diseased individuals (Antonelli & Donelli, 2018). It was found that pain, mood, sleep, and depression symptoms improved after the balneotherapy cure was applied to healthy older adults (Latorre-Román et al., 2015). Özkuk et al. also found a more significant decrease in anxiety after balneotherapy and reported that this may be due to the interaction between pain and anxiety (Özkuk et al., 2018).
This study aims to provide a synthesis of evidence from randomized controlled trials published over the last two decades to determine the effectiveness of hydrotherapy and balneotherapy on anxiety and depression.
Method
This research is a systematic review and meta-analysis. The preparation of the study protocol and reporting of the manuscript were carried out according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (Page et al., 2021). Before the review, the study protocol was registered in the International Register of Prospective Systematic Reviews (PROSPERO) with accession number CRD42023448993.
Research question
In the current systematic review and meta-analysis, the PICOS tool was applied to develop a search strategy by PRISMA recommendations: (P) Population: Adult individuals aged 18 years and older; (I) Intervention: Hydrotherapy and balneotherapy; (C) Comparison: Active control or waiting list; (O) Outcome: Depression and anxiety (S) Study design: Randomized controlled trials.
Search strategy
The literature was searched in PubMed (MEDLINE), Cochrane, Scopus, Web of Science, and CINAHL databases for the last 20 years (2003–2023) between 15 October and 15 November 2023. The following Medical Subject Headings (Mesh) and free text terms were used to search the databases: (“anxi*” OR “panic disorder” OR “phobia” OR “depression” OR “depressive symptoms” OR “depressive disorder” or “major depressive disorder” OR “depressive syndrome”) AND (“hydrotherapy” OR “balneotherapy” OR “thalassotherapy” OR “spa therapy” OR “thermotherapy” OR “phytothermotherapy” OR “aquatic” OR “hydrogalvanic” OR “cryo” OR “pool exercise” OR “water-based” OR “pool-based” OR “stanger” OR “mud” OR “thermal water” OR “bath” OR “peloid” OR “natural therapeutic gas” OR “radon”). Only articles in English are included.
Eligibility criteria
Inclusion criteria for the analyses were 1) articles in English, 2) randomized controlled trials, 3) a sample of adults aged 18 years and older, 4) a sample diagnosed with anxiety or depression according to DSM-V, 5) a sample of healthy/patient individuals in whom anxiety or depression symptoms were measured, 6) studies describing balneotherapy or hydrotherapy as interventions, 7) studies reporting anxiety and depression severity assessed by a valid and reliable scale, 8) studies reporting anxiety and depression severity as mean, standard deviation, 9) studies published in 2003 or later. Control groups may include any form of intervention, including a control intervention (therapy, education) or usual care. The exclusion criteria for this analysis were 1) qualitative studies, correlation studies, cross-sectional studies, case–control studies, and cohort studies 2) studies with a population of children or adolescents.
Study selection
All references obtained through the search strategy were exported with the reference management software Endnote X9 and duplicate references were removed. The identification of the studies to be included in this review was carried out independently by the researchers according to the inclusion and exclusion criteria. Firstly, title/abstract screening was carried out by two independent authors. Studies with titles/summaries that did not meet the inclusion criteria were excluded at this step. Eligible studies were saved in a template created in Excel so that the full text could be read and evaluated. This template consisted of study details (author, publication year, country), inclusion or exclusion status, and reasons for exclusion. Full-text reviews of data extraction, methodological quality assessment, and analysis of included studies were performed by two independent authors. Any disagreements were resolved by discussing the full text of the article. The PRISMA Flow Diagram of the study selection process is given in Fig. 1.

Diagram of selection of studies
Data extraction
Data extraction was carried out by two independent authors to obtain the research data. The information extracted included first author, year of publication, country, sample size and characteristics, intervention type, intervention, and control group, measurement tools used, and results.
To minimize the risk of bias, the literature search, selection of articles, data extraction, and quality assessment of the articles were carried out separately by two researchers. Any disagreement was resolved by discussing the full text of the article.
Quality assessment
The quality assessment of the studies was performed independently by two authors using the Joanna Briggs Institute critical appraisal tools. The “JBI Critical Appraisal Checklist for Randomized Controlled Trials” consisting of 13 items was used for the quality assessment of randomized controlled trials (Barker et al., 2023). Each item in the checklists was coded as yes, no, uncertain, or not applicable. In the checklist, items with “no” and “uncertain” answers received 0 points, while items with “yes” answers received 1 point. The full text of all included studies were analyzed and the studies were scored as a result of the review. Quality scores were given by two independent authors (SK and MY). There was 91.5% inter-rater agreement for quality scores. All discrepancies were discussed and reconciled by the reviewers.
Meta-analytical method
Stata 16.0 software was used for meta-analysis. Heterogeneity between the included studies was evaluated with I2. If the I2 statistic was below 0.50, it was accepted as low heterogeneity and a fixed effects model was used. Mean difference (MD) and standardized mean difference (SMD) were calculated for continuous variables. All tests were calculated with two-tailed tests and a p-value less than 0.05 was considered statistically significant. Begg’s test and Egger’s test were used to assess publication bias, and when the result of the test was p < 0.05, publication bias was considered to be present.
Results
Included studies
As a result of the search in electronic databases, 6,261 articles were found. After removing duplications, 5.431 articles remained. After title/abstract screening, 195 articles were identified as review articles. Of these studies, 178 were excluded from the meta-analysis because they were not randomized controlled trials (n = 73), did not report depression and anxiety outcomes with mean and standard deviation, or were ongoing randomized controlled trials (n = 23), the sample did not consist of adults (n = 8), did not report depression and anxiety (n = 26), and the intervention was not hydrotherapy or balneotherapy (n = 48) (Fig. 1). Seventeen studies were included in the meta-analysis.
Characterization of studies
The studies included in the meta-analysis included six countries. Brazil (Aidar et al., 2018; Assis et al., 2006; Britto et al., 2020; Cavalcanti et al., 2019; Fonseca et al., 2021; Taglietti et al., 2018), Turkey (Ardiç et al., 2007; Bağdatlı et al., 2015; Kurt et al., 2016; Taşkın & Ergin, 2022; Yolgösteren & Külekçioğlu, 2021), Spain (Acosta-Gallego et al., 2018; Pérez-de la Cruz, 2019; Tomas-Carus et al., 2008), Sweden (Hägglund et al., 2017), South Korea (Kim et al., 2012) and Germany (Naumann et al., 2020). There were a total of 977 participants, 455 participants were in the mind–body therapy group and 522 participants were in the control group. The largest sample studied 128 participants (Cavalcanti et al., 2019) and the smallest sample studied 21 participants (Ardiç et al., 2007). Among the 17 eligible studies, 12 included hydrotherapy (Acosta-Gallego et al., 2018; Aidar et al., 2018; Assis et al., 2006; Britto et al., 2020; Cavalcanti et al., 2019; Fonseca et al., 2021; Hägglund et al., 2017; Kim et al., 2012; Pérez-de la Cruz, 2019; Taglietti et al., 2018; Taşkın & Ergin, 2022; Tomas-Carus et al., 2008), 5 (Ardiç et al., 2007; Bağdatlı et al., 2015; Kurt et al., 2016; Naumann et al., 2020; Yolgösteren & Külekçioğlu, 2021) involved balneotherapy (Table 1).
Effect sizes
Anxiety symptoms
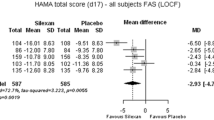
We included 8 studies reporting anxiety as a mental health outcome. The analysis revealed a significant effect and moderate heterogeneity (effect size of [SMD = 0.46 (95% CI 0.27 to 0.65), p = 0.00; I2 = 40.64%]). Hydrotherapy and balneotherapy interventions had a medium effect on reducing anxiety scores (Fig. 2).

Forest plots of the relationship between hydrotherapy/ balneotherapy and depression, anxiety
Depression symptoms
We included 15 studies reporting depression as a mental health outcome. The analysis revealed a significant effect and low heterogeneity (effect size of [SMD = 0.53 (95% CI 0.38 to 0.67), p = 0.00; I2 = 0.00%]). Hydrotherapy and balneotherapy interventions had a medium effect on reducing depression scores (Fig. 2).
Subgroup analysis
All eligible articles were categorized by intervention type for anxiety and depression as shown in Fig. 3. In the subgroup analyses by intervention type for depression, a fixed effects model was used in the analysis due to small heterogeneity between studies (p = 0.69, I2 < 50%). It was found that applying hydrotherapy or balneotherapy intervention did not make a difference in reducing depression scores [SMD = 0.53, 95%CI (0.38, 0.67), p = 0.23]. In the subgroup analyses by intervention type for anxiety, the fixed effects model was used in the analysis since there was medium heterogeneity between the studies (p = 0.11, I2 = 40.64%). Balneotherapy intervention was found to be effective and statistically significant in reducing anxiety scores [SMD = 0.46, 95%CI (0.27, 0.65), p = 0.01].

Forest plots of the relationship between the number of intervention type and depression, anxiety. 1: Hydrotherapy, 2: Balneotherapy
Publication bias
Funnel plot, Begg test, and Egger test were used to evaluate publication bias. No publication bias was found as a result of the Begg test (p = 1.000) and Egger test (p = 0.561) for anxiety. For depression, no publication bias was found as a result of the Begg test (p = 0.620) and Egger test (p = 0.539). According to the funnel plot graph, it was observed that the studies were symmetrically distributed (Fig. 4).

Funnel plots
Reporting quality
The scores for the methodological quality of all studies included in the systematic review ranged from 5 to 12 (Table 2). The methodological quality of 5 studies was below 50% (Aidar et al., 2018; Ardiç et al., 2007; Kim et al., 2012; Taşkın & Ergin, 2022; Yolgösteren & Külekçioğlu, 2021). In 8 of the eligible studies, blinding of outcome assessors (Bağdatlı et al., 2015; Britto et al., 2020; Fonseca et al., 2021; Kurt et al., 2016; Pérez-de la Cruz, 2019; Taglietti et al., 2018; Tomas-Carus et al., 2008; Yolgösteren & Külekçioğlu, 2021) and blinding of outcome assessors and participants in 1 study (Assis et al., 2006).
Discussion
This systematic review and meta-analysis examined the relationship between hydrotherapy and balneotherapy and anxiety and depression symptoms in adults. The results showed that hydrotherapy and balneotherapy were significantly associated with lower anxiety and depression symptoms.
The results of this study suggest that hydrotherapy and balneotherapy interventions provide a significant improvement in depressive symptoms of adult individuals. Castro-Sánchez et al. revealed that 40 sessions of Ai-Chi exercise showed significant improvements in depression scores of multiple sclerosis patients (Castro-Sánchez et al., 2012). In a study conducted by Evcik et al. with 63 patients with fibromyalgia syndrome, water therapy was found to be effective in improving depression (Evcik et al., 2008). Latorre-Román et al. reported that balneotherapy was effective in the severity of depression in healthy adults (Latorre-Román et al., 2015). Dinç Yavaş et al. showed that standard balneotherapy and exercise programs had a positive effect on depression (Dinç Yavaş et al., 2021).
The results of the current study support our findings. Most of the studies that reported depression as a mental health outcome (14 out of 15 studies) did not report any concurrent intervention. This provides an important opportunity to evaluate the unique effects of hydrotherapy and balneotherapy. While 14 of the studies reporting depression as a mental health outcome described depressive symptoms associated with chronic diseases, only 1 evaluated the effectiveness of interventions in patients with depression. Therefore, it should be carefully considered whether existing interventions reduce depression by affecting the clinical picture of chronic diseases or whether they are directly effective on depression. Subgroup analysis showed that the type of intervention did not differ in improving depressive symptoms of adult individuals. Although balneotherapy utilizes the chemical content of water, it is based on similar mechanisms as hydrotherapy. Since both interventions may benefit from similar physical properties of water (temperature, pressure), they may have similar effects on depression (Fritsch et al., 2022).
The results of this study show that hydrotherapy and balneotherapy interventions provide a significant improvement in anxiety symptoms of adult individuals. Dubois et al. reported that balneotherapy provided a significant improvement in the anxiety scores of patients with generalized anxiety disorder compared to paroxetine (Dubois et al., 2010). A review of the literature on the effectiveness of balneotherapy reported that balneotherapy improved depression and anxiety (Clark-Kennedy et al., 2021). In the study by Im and Han, whirlpool hydrotherapy was found to reduce anxiety significantly more than hot compresses (Im & Han, 2013). In a systematic review of the effectiveness of hydrotherapy during labor, it was found that hydrotherapy reduced maternal anxiety (Shaw-Battista, 2017). The results of the current study support our findings. In a systematic review and meta-analysis investigating the effectiveness of hydrotherapy and balneotherapy in fibromyalgia syndrome, it was found that both intervention types did not show a significant effect on depressive symptoms (Naumann & Sadaghiani, 2014).
The current finding contradicts our study result. Most of the studies that reported anxiety as a mental health outcome (7 out of 8 studies) did not report any concurrent intervention. This provides an important opportunity to evaluate the unique effects of hydrotherapy and balneotherapy in reducing anxiety. Subgroup analysis showed that balneotherapy was more effective in improving anxiety symptoms in adults. Since balneotherapy (n = 35) was evaluated with a smaller sample size than hydrotherapy (n = 185), the results of the study on the effectiveness of balneotherapy should be evaluated with caution.
Limitations
This meta-analysis has some limitations. Firstly, the methodological quality of the studies included in the meta-analysis differs from each other. Only 8 studies reported that outcome assessors and 1 study reported that outcome assessors and participants were blinded. In some studies, the randomization method was not explained. In addition, some studies did not provide adequate explanations about the participants who dropped out of the study or did not examine whether the dropouts made a difference in the analyses. These methodological quality problems limit the interpretation of the results. Secondly, the meta-analysis is limited to studies involving the adult population with depression and anxiety symptoms. Except for 1 study including a sample followed up with a diagnosis of depression, the other studies were limited to studies that determined the level of anxiety and depression with self-report scales. The results should be interpreted with caution due to studies conducted with different patient populations. Third, there is a diversity of interventions in the control groups compared. Different interventions make it difficult to generalize and interpret the results; it makes it difficult to determine the true effect of hydrotherapy and balneotherapy.
Conclusion
This study shows that hydrotherapy and balneotherapy reduce depression and anxiety scores in adult individuals. It was found that the type of intervention did not make a difference in improving depression scores of adult individuals, and balneotherapy was a more effective intervention in reducing anxiety scores.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Acosta-Gallego, A., Ruiz-Montero, P. J., & Castillo-Rodríguez, A. (2018). Land- and pool-based intervention in female fibromyalgia patients: A randomized-controlled trial. Turkish Journal of Physical Medicine and Rehabilitation, 64(4), 337–343. https://doi.org/10.5606/tftrd.2018.2314
Aidar, F. J., Jacó de Oliveira, R., Gama de Matos, D., Chilibeck, P. D., de Souza, R. F., Carneiro, A. L., & Machado Reis, V. (2018). A randomized trial of the effects of an aquatic exercise program on depression, anxiety levels, and functional capacity of people who suffered an ischemic stroke. The Journal Of Sports Medicine and Physical Fitness, 58(7–8), 1171–1177. https://doi.org/10.23736/S0022-4707.17.07284-X
Antonelli, M., & Donelli, D. (2018). Effects of balneotherapy and spa therapy on levels of cortisol as a stress biomarker: A systematic review. International Journal of Biometeorology, 62(6), 913–924. https://doi.org/10.1007/s00484-018-1504-8
Ardiç, F., Ozgen, M., Aybek, H., Rota, S., Cubukçu, D., & Gökgöz, A. (2007). Effects of balneotherapy on serum IL-1, PGE2 and LTB4 levels in fibromyalgia patients. Rheumatology International, 27(5), 441–446. https://doi.org/10.1007/s00296-006-0237-x
Assis, M. R., Silva, L. E., Alves, A. M., Pessanha, A. P., Valim, V., Feldman, D., Neto, T. L., & Natour, J. (2006). A randomized controlled trial of deep water running: Clinical effectiveness of aquatic exercise to treat fibromyalgia. Arthritis and Rheumatism, 55(1), 57–65. https://doi.org/10.1002/art.21693
Bağdatlı, A. O., Donmez, A., Eröksüz, R., Bahadır, G., Turan, M., & Erdoğan, N. (2015). Does addition of ‘mud-pack and hot pool treatment’ to patient education make a difference in fibromyalgia patients? A randomized controlled single blind study. International Journal of Biometeorology, 59(12), 1905–1911. https://doi.org/10.1007/s00484-015-0997-7
Bandelow, B., Michaelis, S., & Wedekind, D. (2017). Treatment of anxiety disorders. Dialogues in Clinical Neuroscience, 19(2), 93–107. https://doi.org/10.31887/DCNS.2017.19.2/bbandelow
Barker, T. H., Stone, J. C., Sears, K., Klugar, M., Tufanaru, C., Leonardi-Bee, J., Aromataris, E., & Munn, Z. (2023). The revised JBI critical appraisal tool for the assessment of risk of bias for randomized controlled trials. JBI Evidence Synthesis, 21(3), 494–506.
Becker, B. E. (2009). Aquatic therapy: Scientific foundations and clinical rehabilitation applications. PM & R: The Journal of İnjury, Function, and Rehabilitation, 1(9), 859–872. https://doi.org/10.1016/j.pmrj.2009.05.017
Bernhardt, I. S., Nissen-Lie, H., Moltu, C., McLeod, J., & Råbu, M. (2019). “It’s both a strength and a drawback.” How therapists’ personal qualities are experienced in their professional work. Psychotherapy Research: Journal of the Society for Psychotherapy Research, 29(7), 959–970. https://doi.org/10.1080/10503307.2018.1490972
Britto, A., Rodrigues, V., Dos Santos, A. M., Rizzini, M., Britto, P., Britto, L., & Garcia, J. B. S. (2020). Effects of water- and land-based exercises on quality of life and physical aspects in women with fibromyalgia: A randomized clinical trial. Musculoskeletal Care, 18(4), 459–466. https://doi.org/10.1002/msc.1481
Cacciapuoti, S., Luciano, M. A., Megna, M., Annunziata, M. C., Napolitano, M., Patruno, C., Scala, E., Colicchio, R., Pagliuca, C., Salvatore, P., & Fabbrocini, G. (2020). The role of thermal water in chronic skin diseases management: A review of the literature. Journal of Clinical Medicine, 9(9), 3047. https://doi.org/10.3390/jcm9093047
Castro-Sánchez, A. M., Matarán-Peñarrocha, G. A., Lara-Palomo, I., Saavedra-Hernández, M., Arroyo-Morales, M., & Moreno-Lorenzo, C. (2012). Hydrotherapy for the treatment of pain in people with multiple sclerosis: A randomized controlled trial. Evidence-Based Complementary and Alternative Medicine: Ecam, 2012, 473963. https://doi.org/10.1155/2012/473963
Cavalcanti, A. C. V., Henrique, A. J., Brasil, C. M., Gabrielloni, M. C., & Barbieri, M. (2019). Complementary therapies in labor: randomized clinical trial. Terapias complementares no trabalho de parto: ensaio clínico randomizado. Revista Gaucha de Enfermagem, 40, e20190026. https://doi.org/10.1590/1983-1447.2019.20190026
Clark-Kennedy, J., Kennedy, G., Cohen, M., & Conduit, R. (2021). Mental health outcomes of balneotherapy: A systematic review. International Journal of Spa and Wellness, 4(1), 69–92. https://doi.org/10.1080/24721735.2021.1913368
Dimidjian, S., & Hollon, S. D. (2010). How would we know if psychotherapy were harmful? The American Psychologist, 65(1), 21–33. https://doi.org/10.1037/a0017299
Dinç Yavaş, A., Umay, E., & Tezelli, M. (2021). Osteoartritli hastalarda balneoterapinin depresyon ve anksiyete ölçeği puanlarına etkisi. İmmünoloji Ve Klinik Mikrobiyoloji Dergisi, 6(3), 148–155.
Dubois, O., Salamon, R., Germain, C., Poirier, M. F., Vaugeois, C., Banwarth, B., Mouaffak, F., Galinowski, A., & Olié, J. P. (2010). Balneotherapy versus paroxetine in the treatment of generalized anxiety disorder. Complementary Therapies in Medicine, 18(1), 1–7. https://doi.org/10.1016/j.ctim.2009.11.003
Evcik, D., Yigit, I., Pusak, H., & Kavuncu, V. (2008). Effectiveness of aquatic therapy in the treatment of fibromyalgia syndrome: A randomized controlled open study. Rheumatology International, 28(9), 885–890. https://doi.org/10.1007/s00296-008-0538-3
Fioravanti, A., Karagülle, M., Bender, T., & Karagülle, M. Z. (2017). Balneotherapy in osteoarthritis: Facts, fiction and gaps in knowledge. European Journal of Integrative Medicine, 1(9), 148–150. https://doi.org/10.1016/j.eujim.2017.01.001
Fonseca, A. C. S., Faria, P. C., Alcântara, M. A., Pinto, W. D., De Carvalho, L. G., Lopes, F. G., & Pernambuco, A. P. (2021). Effects of aquatic physiotherapy or health education program in women with fibromyalgia: A randomized clinical trial. Physiotherapy Theory and Practice, 37(5), 620–632. https://doi.org/10.1080/09593985.2019.1639229
Fritsch, K., Nagy, G., Szekanecz, Z., Szűcs, G., Kovács, L., & Bender, T. (2022). Balneotherapy, a complementary non-pharmacological approach for non-inflammatory complaints in systemic lupus erythematosus: A pilot study. In Vivo, 36(6), 3010–3017. https://doi.org/10.21873/invivo.13046
GBD 2019 Diseases and Injuries Collaborators (2020). Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet (London, England), 396(10258), 1204–1222. https://doi.org/10.1016/S0140-6736(20)30925-9
GBD 2019 Fracture Collaborators (2021). Global, regional, and national burden of bone fractures in 204 countries and territories, 1990-2019: a systematic analysis from the Global Burden of Disease Study 2019. The Lancet. Healthy Longevity, 2(9), e580–e592.https://doi.org/10.1016/S2666-7568(21)00172-0
Genç, E. & Deveci, S. E. (2023). Suyun tedavi amaçlı kullanımı: Balneoterapi ve hidroterapi. Bütünleyici ve Anadolu Tıbbı Dergisi, 4(2), 62–86. https://doi.org/10.53445/batd.1245432
Hägglund, E., Hagerman, I., Dencker, K., & Strömberg, A. (2017). Effects of yoga versus hydrotherapy training on health-related quality of life and exercise capacity in patients with heart failure: A randomized controlled study. European Journal of Cardiovascular Nursing, 16(5), 381–389. https://doi.org/10.1177/1474515117690297
Im, S. H., & Han, E. Y. (2013). Improvement in anxiety and pain after whole body whirlpool hydrotherapy among patients with myofascial pain syndrome. Annals of Rehabilitation Medicine, 37(4), 534–540. https://doi.org/10.5535/arm.2013.37.4.534
Karagülle, M., & Karagülle, M. Z. (2015). Effectiveness of balneotherapy and spa therapy for the treatment of chronic low back pain: A review on latest evidence. Clinical Rheumatology, 34(2), 207–214. https://doi.org/10.1007/s10067-014-2845-2
Kim, I. S., Chung, S. H., Park, Y. J., & Kang, H. Y. (2012). The effectiveness of an aquarobic exercise program for patients with osteoarthritis. Applied Nursing Research: ANR, 25(3), 181–189. https://doi.org/10.1016/j.apnr.2010.10.001
Kurt, E. E., Koçak, F. A., Erdem, H. R., Tuncay, F., & Kelez, F. (2016). Which non-pharmacological treatment is more effective on clinical parameters in patients with fibromyalgia: Balneotherapy or aerobic exercise? Archives of Rheumatology, 31(2), 162–169. https://doi.org/10.5606/ArchRheumatol.2016.5751
Latorre-Román, P. Á., Rentero-Blanco, M., Laredo-Aguilera, J. A., & García-Pinillos, F. (2015). Effect of a 12-day balneotherapy programme on pain, mood, sleep, and depression in healthy elderly people. Psychogeriatrics: The Official Journal of the Japanese Psychogeriatric Society, 15(1), 14–19. https://doi.org/10.1111/psyg.12068
Naumann, J., & Sadaghiani, C. (2014). Therapeutic benefit of balneotherapy and hydrotherapy in the management of fibromyalgia syndrome: A qualitative systematic review and meta-analysis of randomized controlled trials. Arthritis Research & Therapy, 16, R141. https://doi.org/10.1186/ar4603
Naumann, J., Kruza, I., Denkel, L., Kienle, G., & Huber, R. (2020). Effects and feasibility of hyperthermic baths in comparison to exercise as add-on treatment to usual care in depression: A randomised, controlled pilot study. BMC Psychiatry, 20(1), 536. https://doi.org/10.1186/s12888-020-02941-1
Özkuk, K., Uysal, B., Ateş, Z., Ökmen, B. M., Sezer, R., & Dilek, G. (2018). The effects of inpatient versus outpatient spa therapy on pain, anxiety, and quality of life in elderly patients with generalized osteoarthritis: A pilot study. International Journal of Biometeorology, 62(10), 1823–1832. https://doi.org/10.1007/s00484-018-1584-5
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., Shamseer, L., Tetzlaff, J. M., Akl, E. A., Brennan, S. E., Chou, R., Glanville, J., Grimshaw, J. M., Hróbjartsson, A., Lalu, M. M., Li, T., Loder, E. W., Mayo-Wilson, E., McDonald, S., McGuinness, L. A.,…, Moher, D. (2021). The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ (Clinical Research Ed.), 372, n71. https://doi.org/10.1136/bmj.n71
Pérez-de la Cruz, S. (2019). Mental health in Parkinson’s disease after receiving aquatic therapy: A clinical trial. Acta Neurologica Belgica, 119(2), 193–200. https://doi.org/10.1007/s13760-018-1034-5
Reger, M., Kutschan, S., Freuding, M., Schmidt, T., Josfeld, L., & Huebner, J. (2022). Water therapies (hydrotherapy, balneotherapy or aqua therapy) for patients with cancer: A systematic review. Journal of Cancer Research and Clinical Oncology, 148(6), 1277–1297. https://doi.org/10.1007/s00432-022-03947-w
Ribeiro, O., Teixeira, L., Araújo, L., Rodríguez-Blázquez, C., Calderón-Larrañaga, A., & Forjaz, M. J. (2020). Anxiety, depression and quality of life in older adults: Trajectories of influence across age. International Journal of Environmental Research and Public Health, 17(23), 9039. https://doi.org/10.3390/ijerph17239039
Shaw-Battista, J. (2017). Systematic review of hydrotherapy research: Does a warm bath in labor promote normal physiologic childbirth? The Journal of Perinatal & Neonatal Nursing, 31(4), 303–316. https://doi.org/10.1097/JPN.0000000000000260
Taglietti, M., Facci, L. M., Trelha, C. S., de Melo, F. C., da Silva, D. W., Sawczuk, G., Ruivo, T. M., de Souza, T. B., Sforza, C., & Cardoso, J. R. (2018). Effectiveness of aquatic exercises compared to patient-education on health status in individuals with knee osteoarthritis: A randomized controlled trial. Clinical Rehabilitation, 32(6), 766–776. https://doi.org/10.1177/0269215517754240
Taşkın, A., & Ergin, A. (2022). Effect of hot shower application on pain anxiety and comfort in the first stage of labor: A randomized controlled study. Health Care for Women International, 43(5), 431–447. https://doi.org/10.1080/07399332.2021.1925282
Tomas-Carus, P., Gusi, N., Häkkinen, A., Häkkinen, K., Leal, A., & Ortega-Alonso, A. (2008). Eight months of physical training in warm water improves physical and mental health in women with fibromyalgia: A randomized controlled trial. Journal of Rehabilitation Medicine, 40(4), 248–252. https://doi.org/10.2340/16501977-0168
Uzbay, T., & Yüksel, N. (2002). Anksiyete tedavisinde kullanılan ilaçların farmakolojisi ve kullanım güvenliği. Klinik Psikiyatri, 5(1), 14–26.
Yolgösteren, E., & Külekçioğlu, S. (2021). The effectiveness of balneotherapy and thermal aquatic exercise in postoperative persistent lumbar pain syndrome. International Journal of Biometeorology, 65(12), 2137–2145. https://doi.org/10.1007/s00484-021-02176-z
Zhang, J., Liu, X., & Fang, L. (2019). Combined effects of depression and anxiety on suicide: A case-control psychological autopsy study in rural China. Psychiatry Research, 271, 370–373. https://doi.org/10.1016/j.psychres.2018.11.010
Funding
Open access funding provided by the Scientific and Technological Research Council of Türkiye (TÜBİTAK).
Author information
Authors and Affiliations
Contributions
SK: Conceptualisation, Methodology, Software, Validation, Formal analysis, Investigation, Data curation, Writing– Original Draft, Visualisation. MY: Methodology, Validation, Writing– Original Draft, Writing– Reviewing & Editing, Supervision, Project administration.
Corresponding author
Ethics declarations
Ethics approval
Not applicable.
Conflicts of interest
The authors have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Koroglu, S., Yıldız, M. Effectiveness of hydrotherapy and balneotherapy for anxiety and depression symptoms: a meta-analysis. Curr Psychol (2024). https://doi.org/10.1007/s12144-024-06062-w
Accepted:
Published:
DOI: https://doi.org/10.1007/s12144-024-06062-w