
Abstract
Background and objective
Hepatitis B virus (HBV) infection is still prevalent in Asia, including Thailand. HBV can archive in hepatocytes for life and can reactivate after immunosuppression and chemotherapy administration. Use of immunosuppressive agents is recommended in many rheumatologic diseases and reactivation of HBV can occur. Data regarding the effect of methotrexate (MTX) on HBV reactivation is scanty. MTX is a well known cause of hepatic fibrosis but its effect on HBV reactivation is not clearly understood. There is no specific recommendation for HBV prophylaxis for patients using MTX. This study aimed to determine the prevalence of HBV seromarkers in rheumatologic patients who were treated with long-term MTX and to evaluate the hepatitis outcome in the patients with positive HBV markers.
Methods
This was a cross-sectional study at the Rheumatology Clinic, Siriraj Hospital, Bangkok, Thailand. Patients aged 15 years or older treated with MTX more than 24 weeks were invited in the study. Review of medical history, MTX prescription and dosage during the last 52 weeks, blood tests for liver function tests, HBV serology, and HBV DNA viral load were performed. The exclusion criteria included patients who were treated with biological DMARDs, drugs active against HBV, known co-infection with HCV or HIV and previous diagnosis of cirrhosis from any causes or presence of hepatocellular carcinoma.
Results
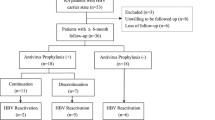
A total of 173 patients were enrolled (153 females, 20 males, mean age of 52.6 ± 13.6 years). The majority of patients were diagnosed with rheumatoid arthritis (67.0 %), SLE (13.9 %), spondyloarthopathies (8.7 %) and others (10.4 %). Thirty percent of them (55/173) had no previous data for HBV seromarkers. Among 118 patients who had baseline data, only one patient (0.8 %) had HBsAg positive. Average duration of treatment was 9.9 years and MTX dose prescribed was 571.6 ± 240.4 mg during the last 52 weeks. Out of 173 patients, only two had clinically significant hepatitis (1.16 %) and one was HBsAg positive (0.58 %). Ninety-six patients (55.5 %) were negative for all HBV seromarkers, 67/173 (38.7 %) positive for anti-HBs antibody and 65/173 (37.6 %) positive for anti-HBc IgG. Only one in 65 patients (1.5 %) who had any positive HBV seromarkers had HBV DNA detectable.
Conclusion
Prevalence of HBsAg positive rheumatologic patients treated with MTX in Thailand was only 0.58 %, which was lower than the general Thai population. About one-third of the patients had exposure to HBV as demonstrated by presence of anti-HBc IgG (37.6 %), but none of them had hepatitis B reactivation during 9.9 years of MTX treatment. Moreover, one case with HBsAg positive had been receiving MTX without HBV prophylaxis for 5 years but had no evidence of HBV flare and evidence of fibrosis. From our study, long-term MTX in patients exposed to HBV was safe and not associated with hepatitis flare. However, more study is needed as to whether HBV prophylaxis is required.


Similar content being viewed by others


References
Fattovich G. Natural history and prognosis of hepatitis B. Semin Liver Dis 2003;23:47–58
McMahon BJ. The natural history of chronic hepatitis B virus infection. Semin Liver Dis 2004;24:17–21
Hadziyannis SJ, Papatheodoridis GV. Hepatitis B e antigen-negative chronic hepatitis B: natural history and treatment. Semin Liver Dis 2006;26:130–141
Fattovich G, Bortolotti F, Donato F. Natural history of chronic hepatitis B: special emphasis on disease progression and prognostic factors. J Hepatol 2008;48:335–352
Fattovich G, Olivari N, Pasino M, D’Onofrio M, Martone E, Donato F. Long-term outcome of chronic hepatitis B in Caucasian patients: mortality after 25 years. Gut 2008;57:84–90
Fattovich G, Stroffolini T, Zagni I, Donato F. Hepatocellular carcinoma in cirrhosis: incidence and risk factors. Gastroenterology 2004;127:535–550
Raimondo G, Allain JP, Brunetto MR, Buendia MA, Chen DS, Colombo M, et al. Statements from the Taormina expert meeting on occult hepatitis B virus infection. J Hepatol 2008;49:652–657
Knoll A, Pietrzyk M, Loss M, Goetz WA, Jilq W. Solid-organ transplantation in HBsAg-negative patients with antibodies to HBV core antigen: low risk of HBV reactivation. Transplantation 2005;79:1631–1633
Marcellin P, Giostra E, Martinot-Peignoux M, Loriot MA, Jaegle ML, Wolf P, et al. Redevelopment of hepatitis-B surface-antigen after renal-transplantation. Gastroenterology 1991;28:231–236
Lok AS, Liang RH, Chiu EK, Wong KL, Chan TK, Todd D. Reactivation of hepatitis B virus replication in patients receiving cytotoxic therapy, report of a prospective study. Gastroenterology 1991;100:182–188
Mindikoglu AL, Regev A, Schiff ER. Hepatitis B virus reactivation after cytotoxic chemotherapy: the disease and its prevention. Clin Gastroenterol Hepatol 2006;4:1076–1081
Saag KG, Teng GG, Patkar NM, Anuntiyo J, Finney C, Curtis JR, et al. American College of Rheumatology 2008 recommendations for the use of nonbiologic and biologic disease modifying antirheumatic drugs in rheumatoid arthritis. Arthritis Rheum 2008;59:762–784
Flowers MA, Heathcote J, Wanless IR, Sherman M, Reynolds WJ, Cameron RG, et al. Fulminant hepatitis as a consequence of reactivation of hepatitis B virus infection after discontinuation of low dose methotrexate therapy. Ann Intern Med 1990;112:381–382
Narvaéz J, Rodriguez-Moreno J, Martinez-Aguila MD, Clavaguera MT. Severe hepatitis linked to B virus infection after withdrawal of low dose methotrexate therapy. J Rheumatol 1998;25:2037–2038
Ito S, Nakazono K, Murasawa A, Mita Y, Hata K, Saito N, et al. Development of fulminant hepatitis B (precore variant mutant type) after the discontinuation of low-dose methotrexate therapy in a rheumatoid arthritis patient. Arthritis Rheum 2001;44:339–342
Hagiyama H, Kubota T, Komano Y, Kurosaki M, Watanabe M, Miyasaka N. Fulminant hepatitis in an asymptomatic chronic carrier of hepatitis B virus mutant after withdrawal of low-dose methotrexate therapy for rheumatoid arthritis. Clin Exp Rheumatol 2004;22:375–376
Watanabe K, Takase K, Ohno S, Ideguchi H, Nozaki A, Ishigatsubo Y. Reactivation of hepatitis B virus in a hepatitis B surface antigen-negative patient with rheumatoid arthritis treated with methotrexate. Mod Rheumatol 2012;22:470–473
Chimparlee N, Oota S, Phikulsod S, Tangkijvanich P, Poovorawan Y. Hepatitis B and hepatitis C virus in Thai blood donors. Southeast Asian J Trop Med Public Health 2011;42:609–615
Srisupanant M, Wiwanitkit V. Prevalence of hepatitis B seropositivity among Thai workers in screening program before going abroad. Ann Hepatol. 2008;7:389
Chongsrisawat V, Yoocharoen P, Theamboonlers A, Tharmaphornpilas P, Warinsathien P, Sinlaparatsamee S, et al. Hepatitis B seroprevalence in Thailand: 12 years after hepatitis B vaccine integration into the national expanded programme on immunization. Trop Med Int Health 2006;11:1496–1502
Luksamijarulkul P, Kaepan W, Klamphakorn S. Hepatitis B virus sero-markers, hepatitis C virus antibody and risk behaviors among middle age and older Thai males. Southeast Asian J Trop Med Public Health 2007;38:45–52
Marignani M, Canzoni M, D’Amelio R, Santis ED, Pecchioli A, Fave GD. Should we routinely treat patients with autoimmune/rheumatic diseases and chronic hepatitis B virus infection starting biologic therapies with antiviral agents? No. Eur J Intern Med 2011;22:576–581
Acknowledgements
The authors gratefully acknowledge the health care personnel of the studied areas. We also wish to extend our deep appreciation to all the participants in this study. This study is supported by Siriraj routine to research management fund.
Compliance with ethical requirements and Conflict of interest
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. Informed consent was obtained from all patients for being included in the study. Charlie Laohapand, Tawesak Tanwandee and Emvalee Arromdee declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Laohapand, C., Arromdee, E. & Tanwandee, T. Long-term use of methotrexate does not result in hepatitis B reactivation in rheumatologic patients. Hepatol Int 9, 202–208 (2015). https://doi.org/10.1007/s12072-014-9597-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12072-014-9597-6