
Abstract
Extracorporeal cardiopulmonary resuscitation (ECPR) is a salvage procedure in which extracorporeal membrane oxygenation (ECMO) is initiated emergently on patients who have had cardiac arrest (CA) and on whom the conventional cardiopulmonary resuscitation (CCPR) has failed. Awareness and usage of ECPR are increasing all over the world. Significant advancements have taken place in the ECPR initiation techniques, in its device and in its post-procedure care. ECPR is a team work requiring multidisciplinary experts, highly skilled health care workers and adequate infrastructure with appropriate devices. Perfect coordination and communication among team members play a vital role in the outcome of the ECPR patients. Ethical, legal and financial issues need to be considered before initiation of ECPR and while withdrawing the support when the ECPR is futile. Numerous studies about ECPR are being published more frequently in the last few years. Hence, keeping updated about the ECPR is very important for proper selection of cases and its management. This article reviews various aspects of ECPR and relevant literature to date.
Similar content being viewed by others


Introduction
If the return of spontaneous circulation (ROSC) is not possible following cardiac arrest (CA) in spite of adequate conventional cardiopulmonary resuscitation (CCPR), the recovery chance is very poor. Over a period of time, various pharmacological and mechanical methods have been tried to improve survival. One of the methods is by initiating venoarterial extracorporeal membrane oxygenation (VA-ECMO) on these patients. VA-ECMO is a mechanical device in which blood is drained from the right atrium directly or through a cannula in the femoral vein and returned back to the arterial system of the patient more commonly through the femoral artery or directly into the aorta after adequate oxygenation. Initiating VA-ECMO on patients who were not salvageable by conventional cardiopulmonary resuscitation (CPR) is termed as extracorporeal cardiopulmonary resuscitation (ECPR). The aim of ECPR is to provide adequate perfusion to the end-organs when the potentially “reversible” conditions were managed. CCPR can provide only 25 to 30% of cardiac output [1], adequate end-organ perfusion, including brain perfusion, can be achieved with ECPR and low flow duration can be reduced [2]. ECPR is a resource-intensive therapy requiring specialized equipment and highly trained multidisciplinary experts which has usually limited to large centres with adequate facility [3, 4].
Resuscitating very sick patients using portable cardiopulmonary bypass is not new. It was reported as early as 1976 by Mattox et al. [5]. Recent advancements in cardiopulmonary bypass technology such as portable and miniaturized extracorporeal machines, preassembled heparin-coated circuits and percutaneous cannulation techniques helped in the widespread usage of ECMO in various clinical situations including CA. It is well known that as the duration of time since onset of CA increases, the mortality increases [6, 7]. Success of ECPR depends on the time of initiation since cardiac arrest, proper equipment, personnel and team work. Ideally, all required health care providers should be available in the hospital 24/7. If that is not possible, there should be a protocol to get the ECPR team to the bedside as soon as possible. Even though successes have been recorded with the longer duration of no ROSC before ECPR initiation, the shortest possible time is preferable [8].
Inclusion and exclusion criteria
ECPR is an emergency procedure. Well-defined criteria to help in selection of ideal patients for ECPR are mandatory to save the deserving CA patients and to differentiate from the patients on whom the ECPR’s outcome is unacceptably low. Unfortunately, there is no uniform consensus on those criteria [10,11,12,13,14,15,16]. Selection criteria accepted by most of the centres are given in Table 1.
ECPR procedure
ECPR cannulation should ensure complete mechanical support to provide adequate circulation and gas exchange. A routine ECMO cannulation selection criterion applies to ECPR also. The ECPR team should ensure the availability of various sizes of the cannulas in the emergency situation. The choice between percutaneous or surgical approach to the femoral vessels mostly depends on the skill and preference of the clinician. A percutaneous technique can be done quickly for which surgical skills are not required, but vessel identification can be challenging in CA situation with higher failure rates. Surgical cannulation needs surgical expertise for which appropriate instruments and setup are needed but vessels can be visualized and handled with care. Ultrasound-guided cannula placement adds to the time but certainly useful in expert hands. The surgical approach is also the only option for failed percutaneous cannulation [17]. Cannulation is usually done in the femoral vessels, because of easy accessibility with ongoing CPR. Alternative approaches include jugulo-femoral, femoro-subclavian or jugulo-subclavian routes [10]. Central cannulation outside the operating theatre requires proper planning with adequate equipment and resources [17].
Pre-primed circuits help to reduce the down time in ECPR. Primed circuits with only crystalloid (free of protein, glucose and blood products) have been found to be free of infection for 14 days and can be used up to 30 days [18, 19]. Preassembled ECMO circuits are available for which setup time is only a few minutes, reducing the need for pre-primed circuits.
Echocardiography offers advantage of cardiac function assessment. In case of severe left ventricular dysfunction as evidenced by poor or non-opening aortic valve, left ventricular decompression is essential to prevent pulmonary oedema, pulmonary haemorrhage, left ventricular distension and clot formation. It can be done by placement of the left atrial catheter via blade septectomy or transthoracic direct left atrial or left ventricular venting [8, 20]. Other mechanical devices are also used along with VA-ECMO. The most commonly used device is the intra-aortic balloon pump (IABP). Other devices include Impella (ABIOMED) or TandemHeart (Cardiac Assist, Inc.) to decompress the left ventricle which also helps in cardiac recovery. Further studies are needed to prove their role [20].
During ECPR, the following parameters guide us to assess the adequacy of the CPR. Quantitative waveform capnography and intra-arterial pressure are very useful. If end-tidal carbon dioxide (EtCO2) is less than 10 mmHg or if diastolic blood pressure is less than 20 mmHg, then CPR quality has to be improved (class IIb, LOE C-EO) [21].
Appropriate transport facility should be available to transfer the patients connected to ECMO during ECPR to the intensive care unit (ICU), especially those who had out-of-hospital cardiac arrest (OHCA).
Post-ECPR management
Post-ECPR management plays a vital role in the outcome of the patient. Apart from the routine post-ECMO management, certain precautions are to be taken for ECPR patients. Targeted temperature management (TTM) influences neurological outcome. Nagao et al., in 2010, reported 171 patients who had unsuccessful CCPR. All underwent ECPR with IABP insertion followed by percutaneous coronary intervention (PCI) if needed. They were maintained on hypothermia of 34 °C for 3 days. Twenty-one patients out of 171 (12.3%) had a good neurological recovery during hospital discharge. Neurologically favourable accuracy of 85.4% and 89.5% was reported in patients with CA to cardiopulmonary bypass (CPB) interval of 55.5 min and CPB to 34 °C interval of 21.5 min respectively [22]. Generally, patient’s core body temperature of 33 to 35 °C is maintained for 24–48 h [8]. Therapeutic hypothermia when compared with normothermia after ECPR is associated with lesser survival with good neurobehavioural outcome at 1-year follow-up [23].
The guidelines of the American Heart Association (AHA) recommend the use of physical examination, electrophysiological modalities, imaging modalities and blood markers to predict neurologic outcomes following CA [24]. Physical examination (pupil diameter and brain stem reflexes), imaging (brain computerized tomography (CT), grey white matter ratio (GWR) and magnetic resonance imaging (MRI), electrophysiological studies (electroencephalogram, bispectral index (BIS) and near-infrared spectroscopy (NIRS)) and laboratory investigations (arterial pH value and serum lactate levels) help in the identification of prognosis of those patients undergoing ECPR [8, 20].
Complications
Most of the complications following ECPR are common to routine ECMO, even though the incidence of those complications can be higher and vary from centre to centre. Vascular injury during cannulation, aberrant placement of the cannula and unsuccessful cannulation (as high as 51.2%) are remarkably higher in ECPR compared with routine ECMO [25, 26]. This may be attributed to time constraint and accessing vessels in pulseless state. The most common complication after initiation of ECPR is bleeding (8.2% to70%) [25, 27]. Bleeding can be from the cannulation site, intracranial bleed, gut bleed, nasal bleed or alveolar haemorrhage [27]. Leg ischaemia can happen in 3% to 15.4% of the ECPR patients [14, 28]. Maekawa et al. reported infection incidence of 7.7% in 2013 whereas Lee et al. reported 21.7% sepsis incidence in 2016 in their post-ECPR patients [14, 29]. Incidence of intracerebral haemorrhage (ICH)/stroke can vary from 2.3 to 17.4% [29, 30].
Results
After ECPR, few factors predict poor outcomes. They are acidosis, serum lactate, renal failure and liver failure not normalizing in 24 h. Following ECPR in small group of patients, “myocardial stunning” can be seen in the first few hours of its initiation. While the exact cause is unknown, the presumed mechanism is imbalance in the cellular calcium concentration. Usually, it is self-limiting. Serum ionized calcium should be normalized. Some patients may need vasodilators to reduce after load, cardiac pacing and left ventricular decompression [8]. Severe neurological injury following CPR can be predicted using serial neurospecific enolase after 48 h of CA [31]. Cesana et al. in 2017 compared ECPR and CCPR, and reported total CA time as the independent predictor of survival in their 148 patients [32].
Holmberg et al., in 2018, in their systematic review of 25 observational studies for the International Liaison Committee on Resuscitation’s (ILCOR) Advanced Life Support and Paediatric Task Forces concluded that there is no conclusive evidence for or against the use of ECPR in in-hospital cardiac arrest (IHCA) and OHCA. The studies in the systematic review had very low quality of evidence [33].
There are two main mechanisms by which brain injury can occur following ECPR. The first mechanism is reduced oxygen delivery to the brain because of poor oxygenation of blood and reduced or no blood flow to the brain. The second mechanism is due to reperfusion injury after establishing adequate oxygenation and blood flow [34]. According to the American Heart Association focussed update in 2019, most of the studies showed improved short-term and long-term neurological outcomes. However, all the studies analysed showed increased risk of bias and they were not randomized [4]. Cesana et al. in 2017 reported cardiac recovery and neurological recovery were similar in ECPR and CCPR groups [32].
Richardson et al., in 2017, reported 29% survival to hospital discharge in their study on 1796 ECPR patients. It is an international multicentre study done comparing ECPR patient’s outcome between 2003 and 2006 vs 2007 and 2010 vs 2011 and 2014. Risk-adjusted survival in all the three groups is the same even though the comorbidities are higher over a period of time and also there are significant advancements in ECMO technology [35]. The CHEER trial in 2015 showed a survival of 45% and 60% in OHCA and IHCA respectively following ECPR with reasonable neurological outcome [36]. In the same year, Siao et al. studied various factors comparing conventional CPR (40 patients) and ECPR (20 patients). The overall survival at discharge with good neurological recovery was 35% and 18.3% in the ECPR and CCPR groups respectively. The mean duration was longer in the ECPR group (69.90 ± 49.6 min) when compared with the CCPR group (34.3 ± 17.7 min) with a p value of 0.0001. About 95% in the ECPR group had more sustained ROSC, whereas the CCPR group had sustained ROSC only in 47.5% of their patients (p = 0.0009). Also, good neurological outcome reported was 40% vs 7.5% in the ECPR vs CCPR groups (p = 0.0067) respectively [16].
Matsuok et al. in their population-based study in 2019 reported an overall survival of 46.3% (87/188) and 20.3% (67/330) in the ECPR and CCPR groups, respectively, out of 518 patients studied. They also reported a favourable neurological outcome of 22.9% (43/188) in the ECPR group as against 8.5% (28/330) in the CCPR group [37]. Dalia et al. reported his single-centre experience in 2020. They reported a hospital survival of 33.8% in their 71 patients who underwent ECPR. Another important observation they made is that those patients requiring renal replacement therapy after ECPR had the highest mortality with only 5.3% surviving discharge from the hospital [38]. In the same year, MacLaren et al. compared outcomes of various ECPR studies. In their comparison, the survival to hospital discharge of ECPR patients following OHCA ranged from 8 to 33%. In IHCA, it ranges between 19 and 60% [39]. Various other studies also showed improved neurological outcome and survival following ECPR compared with CCPR [14, 15, 30, 40]. Gross variation in the outcomes can be seen between the studies mentioned above. This may be due to various factors influencing the outcomes including the patient factors, quality of CCPR, centre’s experience, type of mechanical device used, resource availability and the indices used to determine the outcome. As the available evidences were non-randomized, the outcomes of the studies should be considered only as an association and should not be considered as the result of ECPR intervention [4].
ECPR in children
Most of the ECPR managements are similar in paediatric and adult population. ECPR in the postoperative period following corrective or palliative surgery for congenital heart disease (CHD) is the most common indication for ECPR in the paediatric age group. This condition has better prognosis than other conditions. Cardiac arrhythmias, tamponade, pulmonary hypertension, hypoxemia due to pulmonary blood flow obstruction, myocardial dysfunction and residual lesions are the frequent causes for cardiac arrest in the postoperative period following surgery for CHD. Due to higher risk of neurological injury, ECPRs following bidirectional Glenn and Fontan circulations carry poor prognosis. ECPR is also indicated in the complex intervention for CHD in cathlab. Acute fulminant myocarditis leading to cardiac arrest has a very good prognosis following ECPR [10].
In the postoperative period following sternotomy, ECPR cannulation is through the right atrium and aorta. In other conditions, the right internal jugular vein and carotid artery are cannulated. Rarely peripheral cannulation is through femoral vessels especially in relatively older children [10]. Outcomes following ECPR in neonatal and paediatric age groups are better than those in the adult population. According to the Extracorporeal Life Support Organization (ELSO) registry, survival to discharge in neonatal and paediatric age group was 42% compared to 29% in adult population [41].
Our experience
As success of ECMO patients depends on the team effort, we formed a group called Interdisciplinary Clinical Group of Extracorporeal Life Support (ICE Group) in 2013. This group consists of intensivists, cardiothoracic surgeons, anaesthetists, cardiologists, pulmonologists, nephrologists, infectious disease specialists, gastroenterologists, vascular surgeons, interventional radiologists, psychiatrists, perfusionists, dieticians, physiotherapists and nurses. In this group, cardiothoracic surgeons and intensivists take the role of ECMO specialists. We work as a team to achieve results on par with the international standards. We have dedicated intensive care unit to manage these patients. We developed an ECPR kit which contains all the essential materials that can be wheeled into the ECPR site for rapid ECPR initiation. The ECPR kit contains a preassembled ECMO circuit, serial dilators, cannulas of various sizes, antiseptic solutions, surgical drapes, surgical aprons, gloves, a surgical tray for vascular access, surgical blades, suture materials and ECMO consent forms. Proper planning and standard operating protocol (SOP) are very essential for the improved survival of ECPR patients. As there is no universally accepted SOP, each centre should have their own depending on the available resources and expertise. We have developed a SOP which was devised by our team (Fig. 1) to reduce the down time of ECPR.

Algorithm followed in our centre for ECPR. CCPR, conventional CPR; ABG, arterial blood gas; ROSB, return of spontaneous beating; LV, left ventricle. Step 3: ECMO team arrival in less than 5 min. Percutaneous vascular access in 5 to 10 min. If not proceed with surgical vascular access. Step 4: ECMO initiation is followed by a distal limb perfusion cannula if femoral artery is cannulated. Aim for a down time of less than 45 min from CA. Step 7: LV decompression by direct LV venting surgically or through the right superior pulmonary vein if ECPR is initiated via central cannulation
Out of 186 ECMOs done by our team since 2011, 11 were ECPRs (5.9%). The cause of CA and configuration of ECMO in these eleven patients are listed in Table 2. All instances were witnessed IHCA. Six (54.5%) patients were successfully separated from ECMO and 5 (45.5%) survived to discharge from the hospital. Our down time ranges from 36 to 84 min with a mean duration of 52 min. Our cannulation strategy is to proceed with peripheral VA-ECMO, percutaneously if vascular access is possible in less than 5 min. If not, we will proceed with the semi-Seldinger technique by exposing the vessels. All of our patients had peripheral cannulation except three patients who had central cannulation after emergency sternotomy. The emergency sternotomy during ECPR is expeditiously performed when cardiac compressions are withheld very briefly (only few seconds at a time) to allow sternotomy. By allowing periods of external cardiac compressions to maintain adequate cerebral perfusion, sternotomy can be safely performed in the few seconds when the chest compressions are stopped. One patient had a high body mass index of 48 kg/m2, necessitating a central cannulation for providing adequate flow. The other two patients had severe spasm of the groin vessels, due to high vasopressor doses, precluding peripheral cannulation. Hence, central cannulation was done via emergency sternotomy as described above.
One patient had limb ischaemia despite placing a distal limb perfusion cannula which was managed successfully by fasciotomy. A patient on VA-ECMO had re-exploration for bleeding. Out of the 5 patients who could not be saved, one patient was awaiting heart transplantation post-coronary artery bypass grafting (CABG) (7 years ago) with atheromatous femoral artery dissected during cannulation. Two patients had irreversible cerebral hypoxia. One patient had multiorgan failure with very poor prognosis for which next of kin opted for death not to escalate/resuscitate (DNE/DNR). The last patient had significant irreparable intracerebral bleed. Of the six patients who were successfully separated from ECMO, one patient succumbed to sepsis, while the remaining five patients were discharged from the hospital. Our good results can be attributed to the fact that all the patients had witnessed IHCA. Except for 2 patients, the remaining 9 patients had IHCA in the ICU where trained personnel were available to give adequate CPR and well monitored avoiding low flow state. The two patients who suffered a CA in the ward had prompt CPR which was quickly taken over by the medical emergency team (MET) health care workers within few minutes.
ELSO registry
According to the international summary in ELSO registry updated until January 2020, a total of 15,055 ECPRs were reported all over the world [41]. The survival following ECPR in neonatal and paediatric population is better than that in the adult as shown in Table 3.
Financial considerations
ECPR is a labour-intensive and resource-consuming procedure. Hence, the cost of the procedure can be considerably higher. Financial burden should be considered wisely and judicially used. Dennis et al. in 2019 reported cost-effectiveness in ECPR along with the quality of life analysis. In their study, consecutive 62 ECPR patients were studied. IHCA were 38 (61%) patients with survival of 40% (25 patients) to hospital discharge. All had cerebral performance category (CPC) of 1 or 2. Their study concluded cost-effectiveness in favour of ECPR [42]. In the same year, Gravesteijn et al. also showed ECPR on IHCA patients to be cost-effective using the Markov model [43]. Financial discussion with the family members before initiating ECPR is to be done in developing countries especially when the patients sponsor themselves. This is in contrast to some developed countries where financial aspects would be taken care by the government. Due to time constraint and ethical consideration, financial discussion before ECPR is not easy. If possible, every effort should be made to identify patients prone for cardiac arrest and brief the family members about the ECPR, including its risks and benefits along with the approximate cost involved. This will make the ECPR decision process easier and quicker if CA happens. However, this is applicable only to the patients in the hospital showing worsening haemodynamic parameters.
Ethical and legal considerations
ECPR is done as a bridge to recovery or decision-making or to plan some other modalities like transplantation or assist devices. Decision-making to stop the unsuccessful CCPR is easy. But that is not the case in ECPR especially when the patient is “bridged to nowhere”, haemodynamically stable, neurologically intact but not a candidate for transplant or permanent mechanical circulatory support system. Morbidity and mortality increases with increasing length of ECMO support [44]. In VA-ECMO, there is no survival benefit after 4 weeks in patients with primary cardiac failure [45]. It is advisable to consider other forms of cardiac support if there is no recovery in 2-week duration [46].
Steven A. Conrad states that “The basic principles of autonomy, beneficence, non-maleficence and justice become more complex during extracorporeal resuscitation efforts. These issues influence decisions while initiating or terminating the support” [17]. Despite daily updates, it is usually very difficult to convince the patient’s relatives regarding futility of care especially when the patient is awake and stable. Every “precious moment spent on ECMO” is translated to the love and care towards their loved one. On the other hand, medical ethics and effective resource management will not permit the health care workers to prolong the care indefinitely. There are always three possible outcomes following ECPR: Patient can die due to complication, patient may recover or patient may have irreversible damage of the organ for which the ECMO was initiated. In the first two, the decision is straightforward. In the last group, if there is no option of transplantation or permanent mechanical support, then end-of-life care should be suggested. End of life on ECMO can be the end of the patient’s biologic life or the end of artificial life support like oxygenator or pump failure. Most often, patients and their relatives can be counselled for do not resuscitate (DNR)/do not escalate (DNE) treatment and wait for end of artificial life support. This is legally and ethically acceptable in most of the countries. The patient’s family should be counselled daily regarding the possible outcomes along with the current status of the patient. Explaining everything in detail before ECPR is a challenge due to time constraint [47]. At the earliest possible time after the ECPR, detailed counselling of the family members regarding various aspects of ECPR is mandatory. This will help the family members to make appropriate decision if the patient reaches a point of no return. The legal implication for the end-of-life care varies among different countries. Legal consideration should be given before the family discussion about the end-of-life support care.
ECPR and organ donation
Like ECMO, organ transplantation is also a rapidly evolving field. Organs like the kidney, liver and lungs were being successfully transplanted from brain-dead (BD) patients following ECPR. Casadio et al. in a single-centre observational study reported organ donation following ECPR. Between 2011 and 2016, 112 patients received ECPR, out of which 25 patients (22.3%) were declared as BD patients. The rate of donation in BD patients was 56%, with 39 donated organs: 4 lungs, 12 livers and 23 kidneys. About 89.74% of the transplanted organs reached an early good functional recovery [48]. This opens up the possibility of ECPR even in patients with contraindication for ECPR, for the purpose of organ donation after detailed consideration of ethical and legal issues.
ECPR in COVID patients
So far, the Extracorporeal Life Support Organization (ELSO) does not recommend ECPR usage in centres with lesser experience or in centres which do not have E-CPR program before this Coronavirus Disease 19 (COVID-19) pandemic. OHCA ECPR is not recommended due to rising incidence of COVID-19 patients along with shortage of health care workers. ECPR in IHCA can be considered in carefully selected group of non-COVID-19 patients in experienced centres subjected to the availability of the resources. In COVID-19 patients, ECPR can be considered only after ensuring stringent measures to prevent cross-contamination among the health care workers and also ensure the availability of personal protective equipment (PPE) for various health care providers. CCPR results are poor in COVID-19 patients. Venovenous ECMO to VA-ECMO conversion is not advisable due to poor prognosis [49]. According to the ELSO registry until now, out of a total of 1447 suspected or confirmed COVID-19 patients, 17 (1%) patients underwent ECPR [50].
Future
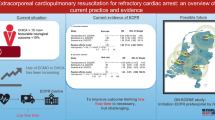
Even though the ECPR practice is several years old, various unanswered questions need to be answered by structured studies. Several randomized control trials are currently in progress to answer some of the questions. At present, Austria is conducting ECPB4OHCA (Emergency Cardiopulmonary Bypass for CA) TRIAL (NCT01605409 ClinicalTrials.gov) to identify the incidence of ROSC in 48 h following CCPR vs ECPR in a study population of 40 patients. In Netherlands, the INCEPTION (Early Initiation of Extracorporeal Life Support in Refractory OHCA) Trial (NCT03101787 ClinicalTrials.gov) is studying the 30-day survival rate with improved neurological recovery in OHCA between CCPR and ECPR. A total of 110 patients were planned and the cerebral performance category scale of 1 to 3 indicates good outcome. The EROCA Study (NCT03065647 ClinicalTrials.gov) in the USA is looking at the efficiency of emergency transport to the possible ECPR centre. The sample size of the study is 30 patients [20]. Further studies need to clarify patient selection, brain protection strategies, resource allocation, effectiveness of hypothermia, usage along with IABP/Impella/TandemHeart, cost-effectiveness and ethical issues [4]. Most of the management issues following ECPR are handled like patients who were successfully revived by CCPR even though adding ECMO to the CPR has its own advantages and disadvantages. This type of management needs modification after proper trials in the concerned field of interest. In short, further studies are needed to formulate protocols which will help in the management of patients before, during and after ECPR procedure [44].
Ethical issues remain to be addressed in countries where brain death is not recognized especially when brain death happens after ECPR and circulation can be prolonged with artificial support [17]. At present, ECPRs are mostly done in tertiary care centre. It should be made available for a wider population. Spreading awareness about ECPR is mandatory for its wider usage. Emergency department doctors should also be trained to initiate ECPR [51]. Legal and ethical issues around organ donation following ECPR need more clarification. Clear-cut differentiation between ECPR and initiation of ECMO on dead patients to protect the organs is important for ethical and legal purposes.
Conclusion
So far, data supporting the routine use of ECPR in cardiac arrest patients is not sufficient. When CCPR fails, ECPR can be considered for a selected group of patients when the expertise is available to rapidly initiate ECPR (class2b; level of evidence C-LD). Further studies are needed to clarify pre-procedural, intra-procedural and post-procedural management of ECPR and its outcomes [44]. Ethical, Legal and financial issues are to be considered in ECPR. A more formalized approach is needed in ECPR while considering organ donation [4, 52].
References
Barsan WG, Levy RC. Experimental design for study of cardiopulmonary resuscitation in dogs. Ann Emerg Med. 1981;10:135–7.
Belohlavek J, Mlcek M, Huptych M, et al. Coronary versus carotid blood flow and coronary perfusion pressure in a pig model of prolonged cardiac arrest treated by different modes of venoarterial ECMO and intraaortic balloon counterpulsation. Crit Care. 2012;16:R50.
Duff JP, Topjian CAA, Berg MD, et al. AHA focused update: 2019 American Heart Association focused update on pediatric advanced life support: an update to the American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2019;140:e904–14. https://doi.org/10.1161/CIR.0000000000000731.
Panchal AR, Berg CKM, Hirsch KG, et al. AHA focused update: 2019 American Heart Association focused update on advanced cardiovascular life support: use of advanced airways, vasopressors, and extracorporeal cardiopulmonary resuscitation during cardiac arrest: an update to the American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2019;140:e881–94. https://doi.org/10.1161/CIR.0000000000000732.
Mattox KL, Beall AC Jr. Resusctation of the moribund patient using portable cardiopulmonary bypass. Ann Thorac Surg. 1976;22 436–442.
Grasselli G, Pesenti A, Marcolin R, et al. Percutaneous vascular cannulation for extracorporeal life support(ECLS): a modified technique. Int J Artif Organs. 2010;33:553–7.
Shih CL, Lu TC, Jerng JS, et al. A web-based Utstein style registry system of in-hospital cardiopulmonary resuscitation in Taiwan. Resuscitation. 2007;72:394–403.
Short BL, Williams L. ECMO specialist training manual. 3rd ed. Ann Arbor: Extracorporeal Life Support Organisation; 2010. p. 181–7.
Pappalardo F, Montisci A. What is extracorporeal cardiopulmonary resuscitation? J Thorac Dis. 2017;9:1415–9.
Brogan TV, Lequier L, Lorusso R, MacLaren G, Peek G. Extracorporeal life support: the ELSO red book. 5th ed. Ann Arbor: Extracorporeal Life Support Organisation; 2017. p. 505.
Chen YS, Lin JW, Yu HY, et al. Cardiopulmonary resuscitation with assisted extracorporeal life-support versus conventional cardiopulmonary resuscitation in adults with in-hospital cardiac arrest: an observational study and propensity analysis. Lancet. 2008; 372: 554–561.
Shin TG, Chio JH, Jo IJ, et al. Extracorporeal cardiopulmonary resuscitation in patients with in hospital cardiac arrest: a comparison with conventional cardiopulmonary resuscitation. Crit Care Med. 2011;39:1–7.
Lin JW, Wang MJ, Yu HY, et al. Comparing the survival between extracorporeal rescue and conventional resuscitation in adult in-hospital cardiac arrests: propensity analysis of three-year data. Resuscitation. 2010;81:796–803.
Maekawa K, Tanno K, Hase M, Mori K, Asai Y. Extracorporeal cardiopulmonary resuscitation for patients with out-of –hospital cardiac arrest of cardiac origin: a propensity matched study and predictor analysis. Crit Care Med. 2013;41:1186–96.
Sakamoto T, Morimura N, Nagao K, et al. Extracorporeal cardiopulmonary resuscitation versus conventional cardiopulmonary resuscitation in adults with out-of-hospital cardiac arrest: a prospective observational study. Resuscitation. 2014;85:762–8.
Siaoa F-Y, Chiua C-C, Chiua C-W, et al. Managing cardiac arrest with refractory ventricular fibrillation in the emergency department: conventional cardiopulmonary resuscitation versus extracorporeal cardiopulmonary resuscitation. Resuscitation. 2015;92:70–6.
Conrad SA. Extracorporeal cardiopulmonary resuscitation. Egypt J Crit Care MeD. 2016;4:11–5.
Bistrussu S, Beeton A, Castaldo G, et al. An extracorporeal membrane oxygenation circuits that are primed with plasmalyte and stored a likely source of infection? J Clin Microbiol. 2004;42:3906.
Weinberg A, Miko B, Beck J, Bacchetta M, Mongero L. Is it safe to leave an ECMO circuit primed? Perfusion. 2015;30:47–49.
Inoue A, Hifumi T, Sakamoto T, Kuroda Y. Extracorporeal cardiopulmonary resuscitation for out-of-hospital cardiac arrest in adult patients. J Am Heart Assoc. 2020;9:e015291. https://doi.org/10.1161/JAHA.119.015291.
Link MS, Berkow LC, Kudenchuk PJ. et al. Part 7: Adult advanced cardiovascular life support :2015 American Heart Association Guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2015; 132:S444–S464. https://doi.org/10.1161/CIR.0000000000000261.
Nagao K, Kikushima K, Watanabe K, et al. Early induction of hypothermia during cardiac arrest improves neurological outcomes in patients with out-of hospital cardiac arrest who undergo emergency cardiopulmonary bypass and percutaneous coronary intervention. Circ J.2010; 74: 77–85.
Meert KL, Guerguerian AM, Barbaro R, et al. Therapeutic Hypothermia After Pediatric Cardiac Arrest (THAPCA) Trial Investigators. Extracorporeal cardiopulmonary resuscitation: one-year survival and neurobehavioral outcome among infants and children with in-hospital cardiac arrest. Crit Care Med. 2019;47:393–402. https://doi.org/10.1097/CCM.0000000000003545.
Callaway CW, Donnino MW, Fink EL, et al. Part 8: post-cardiac arrest care: 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2015;132:S465–82.
Kashiura M, Sugiyama K, Tanabe T, Akashi A, Hamabe Y. Effect of ultrasonography and fluoroscopic guidance on the incidence of complications of cannulation in extracorporeal cardiopulmonary resuscitation in out-of-hospital cardiac arrest: a retrospective observational study. BMC Anesthesiol. 2017;17:4.
Champigneulle B, Bellenfant-Zegdi F, Follin A, et al. Extracorporeal life support(ECLS) for refractory cardiac arrest after drowning: an 11-year experience. Resuscitation. 2015;88:126–31.
Otani T, Sawano H, Natsukawa T, et al. D-dimer predicts bleeding complication in out-of-hospital cardiac arrest resuscitated with ECMO. Am J Emerg Med. 2018;36:1003–8.
Ha TS, Yang JH, Cho YH, et al. Clinical outcomes after rescue extracorporeal cardiopulmonary resuscitation for out-of- hospital cardiac arrest. Emerg Med J. 2017;34:107–11.
Lee JJ, Han SJ, Kim HS, et al. Out-of-hospital cardiac arrest patients treated with cardiopulmonary resuscitation using extracorporeal membrane oxygenation: focus on survival rate and neurologic outcome. Scand J Trauma Resusc Emerg Med. 2016;24:74.
Kim SJ, Jung JS, Park JH, Park JS, Hong YS, Lee SW. An optimal transition time to extracorporeal cardiopulmonary resuscitation for predicting good neurological outcome in patients with out-of-hospital cardiac arrest: a propensity-matched study. Crit Care. 2014;18:535.
Schrage B, Ruebsamen N, Becher PM, et al. Neuron-specific-enolase as a predictor of the neurologic outcome after cardiopulmonary resuscitation in patients on ECMO. Resuscitation. 2019;136:14–20.
Cesana F, Avalli L, Garatti L, et al. Effects of extracorporeal cardiopulmonary resuscitation on neurological and cardiac outcome after ischaemic refractory cardiac arrest. Eur Heart J Acute Cardiovasc Care.2018; 7:432–441.
Holmberg MJ, Geri G, Wiberg S, et al. Extracorporeal cardiopulmonary resuscitation for cardiac arrest: A systematic review. Resuscitation. 2018; 131: 91–100.
Sekhon MS, Ainslie PN, Griesdale DE. Clinical pathophysiology of hypoxic ischemic brain injury after cardiac arrest: a “two-hit” model. Crit Care. 2017;21:90.
Richardson ASC, Schmidt M, Bailey M, Pellegrino VA, Rycus PT, Pilcher DV. ECMO Cardio-Pulmonary Resuscitation (ECPR), trends in survival from an international multicentre cohort study over 12-years: Resuscitation.2017; 112: 34–40.
Stub D, Bernard S, Pellegrino V, et al. Refractory cardiac arrest treated with mechanical CPR, hypothermia, ECMO and early reperfusion(the CHEER trial). Resuscitation. 2015;86:88–94.
Matsuok Y, Ikenoue T, Hata N, et al. Hospital’s extracorporeal cardiopulmonary resuscitation capabilities and outcomes in out-of-hospital cardiac arrest: a population-based study. Resuscitation. 2019;136:85–92.
Dalia AA, Lu SY, Villavicencio M, et al. Extracorporeal cardiopulmonary resuscitation: Outcomes and complications at a quaternary referral centre. J Cardiothorac Vasc Anesth. 2020;34:1191–94.
MacLaren G, Masoumi A, Brodie D. ECPR for out-of-hospital cardiac arrest: more evidence is needed. Crit Care. 2020;24:7. https://doi.org/10.1186/s13054-019-2722-0.
Tanno K, Itoh Y, Takeyama Y, Nara S, Mori K, Asai Y. Utstein style study of cardiopulmonary bypass after cardiac arrest. Am J Emerg Med. 2008;26:649–54.
Extracorporeal Life Support Organization. www.elso.org. ECLS Registry Report: International Summary; Jan2020.
Dennis M, Zmudzki F, Burns B, et al. Cost effectiveness and quality of life analysis of extracorporeal cardiopulmonary resuscitation (ECPR) for refractory cardiac arrest. Resuscitation. 2019;139:49–56.
Gravesteijn BY, Schluep M, Voormolen DC, et al. Cost-effectiveness of extracorporeal cardiopulmonary resuscitation after in-hospital cardiac arrest: a Markov decision model. Resuscitation. 2019;143:150–7.
Kratzert WB, Gudzenko V. ECPR or do not ECPR—who and how to choose. J Cardiothorac Vasc Anesth. 2020;34:1195–7.
Rajagopal SK, Almond CS, Laussen PC, Rycus PT, Wypij D, Thiagarajan RR. Extracorporeal membrane oxygenation for the support of infants, children, and young adults with acute myocarditis: a review of the Extracorporeal Life Support Organization registry. Crit Care Med. 2010;38:382–7.
d'Udekem Y, Shime N, Lou S, MacLaren G. Recurrent or prolonged mechanical circulatory support: bridge to recovery or road to nowhere? Pediatr Crit Care Med. 2013;14:S69–72.
Ramanathan K, Cove ME, Caleb MG, Teoh KLK, Maclaren G. Ethical dilemmas of adult ECMO: emerging conceptual challenges. J Cardiothorac Vasc Anaesth. 2015;29:229–233.
Casadio MC, Coppo A, Vargiolu A, et al. Organ donation in cardiac arrest patients treated with extracorporeal CPR: a single centre observational study. Resuscitation. 2017;118:133–9.
Shao F, Xu S, Ma X, et al. In hospital cardiac arrest outcomes among patients with COVID-19 pneumonia in Wuhan, China. Resuscitation. 2020;151:18–23. https://doi.org/10.1016/j.resuscitation.2020.04.005.
Extracorporeal Life Support Organization COVID-19 interim guidelines: a consensus document from an international group of interdisciplinary ECMO providers. 14th, June, 2020. www.elso.org: Guidelines for ECMO in COVID-19.
Bellezzo JM, Shinar Z, Davis DP, et al. Emergency physician-initiated extracorporeal cardiopulmonary resuscitation. Resuscitation. 2012;83:966–70.
Brooks SC, Anderson ML, Bruder E, et al. Part 6: Alternative techniques and ancillary devices for cardiopulmonary resuscitation: 2015 American Heart Association Guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2015;132:S436–S443. https://doi.org/10.1161/CIR.0000000000000260.
Funding
Nil.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Nil.
Ethical committee approval
Not applicable.
Informed consent
Not applicable.
Statement of human and animal rights
Human and animal rights were not violated.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kumar, K.M. ECPR—extracorporeal cardiopulmonary resuscitation. Indian J Thorac Cardiovasc Surg 37 (Suppl 2), 294–302 (2021). https://doi.org/10.1007/s12055-020-01072-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12055-020-01072-2