
Abstract
Background
The monitoring of intracranial pressure (ICP) and detection of increased ICP are crucial because such increases may cause secondary brain injury and a poor prognosis. Although numerous ultrasound parameters, including optic nerve sheath diameter (ONSD), width of the crural cistern (WCC), and the flow velocities of the central retinal artery and middle cerebral artery, can be measured in patients after hemicraniectomy, researchers have yet to determine which of these is better for evaluating ICP. This study aimed to analyze the correlation between ICP and ultrasound parameters and investigate the best noninvasive estimator of ICP.
Methods
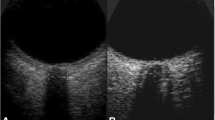
This observational study enrolled 50 patients with brain injury after hemicraniectomy from January 2021 to December 2021. All patients underwent invasive ICP monitoring with microsensor, transcranial, and ocular ultrasound postoperatively. We measured the ONSD including the dura mater (ONSDI), the ONSD excluding the dura mater, the optic nerve diameter (OND), the eyeball transverse diameter (ETD), the WCC, and the flow velocities in the central retinal artery and middle cerebral artery. Then, we calculated the ONSDI-OND (the difference between ONSDI and OND) and ONSDI/ETD (the ratio of ONSDI to ETD). Patients were divided into a normal ICP group (n = 35) and an increased ICP group (≥ 20 mm Hg, n = 15) according to the ICP measurements. Correlations were then assessed between the values of the ultrasound parameters and ICP.
Results
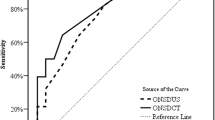
The ONSDI, ONSDI-OND, and ONSDI/ETD were positively associated with ICP (r = 0.455, 0.482, 0.423 and p = 0.001, < 0.001, 0.002, respectively), whereas the WCC was negatively associated with ICP (r = − 0.586, p < 0.001). The WCC showed the highest predictive power for increased ICP (area under the receiver operating characteristic curve [AUC] = 0.904), whereas the ONSDI-OND and ONSDI also presented with acceptable predictive power among the ONSD-related parameters (AUC = 0.831, 0.803, respectively). The cutoff values for increased ICP prediction for ONSDI, ONSDI-OND, and WCC were 6.29, 3.03, and 3.68 mm, respectively. The AUC of the combination of ONSDI-OND and WCC was 0.952 (95% confidence interval 0.896–1.0, p < 0.001).
Conclusions
The ONSDI, ONSDI-OND, and WCC were correlated with ICP and had acceptable accuracy levels in estimating ICP in patients after hemicraniectomy. Furthermore, WCC showed a higher diagnostic value than ONSD-related parameters, and the combination of ONSDI-OND and WCC was a satisfactory predictor of increased ICP.




Similar content being viewed by others

Abbreviations
- ICP:
-
Intracranial pressure
- ONSD:
-
Optic nerve sheath diameter
- WCC:
-
Width of crural cistern
- CRA:
-
Central retinal artery
- MCA:
-
Middle cerebral artery
- ONSDI:
-
ONSD including the dura mater
- ONSDE:
-
ONSD excluding the dura mater
- OND:
-
Optic nerve diameter
- ETD:
-
Eyeball transverse diameter
- AUC:
-
Area under the curve
- ROC:
-
Receiver operating characteristic
- PSV:
-
Peak systolic velocity
- EDV:
-
End-diastolic velocity
- MFV:
-
Mean flow velocity
- RI:
-
Resistance index
- PI:
-
Pulsatility index
- MDC:
-
Minimal detectable changes
- ICC:
-
Intraclass correlation coefficient
References
Sahuquillo J, Dennis JA. Decompressive craniectomy for the treatment of high intracranial pressure in closed traumatic brain injury. Cochrane Datab Syst Rev. 2019;12(12):003983.
Aarabi B, Hesdorffer DC, Ahn ES, Aresco C, Scalea TM, Eisenberg HM. Outcome following decompressive craniectomy for malignant swelling due to severe head injury. J Neursurg. 2006;104(4):469–79.
Vik A, Nag T, Fredriksli OA, et al. Relationship of “dose” of intracranial hypertension to outcome in severe traumatic brain injury. J Neursurg. 2008;109(4):678–84.
Hawryluk GWJ, Rubiano AM, Totten AM, et al. Guidelines for the management of severe traumatic brain injury: 2020 update of the decompressive craniectomy recommendations. Neurosurgery. 2020;87(3):427–34.
Walek KW, Leary OP, Sastry R, et al. Risk factors and outcomes associated with external ventricular drain infections. Infect Control Hosp Epidemiol. 2022;43(12):1859–66.
Dasic D, Hanna SJ, Bojanic S, Kerr RSC. External ventricular drain infection: the effect of a strict protocol on infection rates and a review of the literature. Br J Neurosurg. 2006;20(5):296–300.
Robba C, Santori G, Czosnyka M, et al. Optic nerve sheath diameter measured sonographically as non-invasive estimator of intracranial pressure: a systematic review and meta-analysis. Intensive Care Med. 2018;44(8):1284–94.
Jeub M, Schlapakow E, Ratz M, et al. Sonographic assessment of the optic nerve and the central retinal artery in idiopathic intracranial hypertension. J Clin Neurosci. 2020;72:292–7.
Czosnyka M. Post-traumatic hydrocephalus: influence of craniectomy on the CSF circulation. J Neurol Neurosurg Psychiatry. 2000;68(2):246–8.
Jacobs B, Beems T, van der Vliet TM, Borm GF, Vos PE. The status of the fourth ventricle and ambient cisterns predict outcome in moderate and severe traumatic brain injury. J Neurotrauma. 2010;27(2):331–40.
Mancall EL, Brock DG, Gray H. Gray’s clinical neuroanatomy: the anatomic basis WAfor clinical neuroscience. Philadelphia, PA: Elsevier; 2011.
Hong JH, Jeon I, Seo Y, Kim SH, Yu D. Radiographic predictors of clinical outcome in traumatic brain injury after decompressive craniectomy. Acta Neurochir (Wien). 2021;163(5):1371–81.
Wang Y, Duan Y-Y, Zhou H-Y, et al. Middle cerebral arterial flow changes on transcranial color and spectral Doppler sonography in patients with increased intracranial pressure. J Ultrasound Med. 2014;33(12):2131–6.
Stevens RRF, Gommer ED, Aries MJH, et al. Optic nerve sheath diameter assessment by neurosonology: a review of methodologic discrepancies. J Neuroimaging. 2021;31(5):814–25.
Toms DA. The mechanical index, ultrasound practices, and the ALARA principle. J Ultrasound Med. 2006;25(4):560–1.
Badri S, Chen J, Barber J, et al. Mortality and long-term functional outcome associated with intracranial pressure after traumatic brain injury. Intensive Care Med. 2012;38(11):1800–9.
Calviello L, Donnelly J, Cardim D, et al. Compensatory-reserve-weighted intracranial pressure and its association with outcome after traumatic brain injury. Neurocrit Care. 2018;28(2):212–20.
Lochner P, Czosnyka M, Naldi A, et al. Optic nerve sheath diameter: present and future perspectives for neurologists and critical care physicians. Neurol Sci. 2019;40(12):2447–57.
Youm JY, Lee JH, Park HS. Comparison of transorbital ultrasound measurements to predict intracranial pressure in brain-injured patients requiring external ventricular drainage. J Neurosurg. 2022;136(1):257–63.
Klinzing S, Hilty MP, Bechtel-Grosch U, Schuepbach RA, Bühler P, Brandi G. Dynamic optic nerve sheath diameter changes upon moderate hyperventilation in patients with traumatic brain injury. J Crit Care. 2020;56:229–35.
Wang J, Li K, Li H, et al. Ultrasonographic optic nerve sheath diameter correlation with ICP and accuracy as a tool for noninvasive surrogate ICP measurement in patients with decompressive craniotomy. J Neurosurg. 2020;133(2):514–20.
Gao Y, Li Q, Wu C, Liu S, Zhang M. Diagnostic and prognostic value of the optic nerve sheath diameter with respect to the intracranial pressure and neurological outcome of patients following hemicraniectomy. BMC Neurol. 2018;18(1):199.
Shapiro K, Fried A, Takei F, Kohn I. Effect of the skull and dura on neural axis pressure-volume relationships and CSF hydrodynamics. J Neurosurg. 1985;63(1):76–81.
Hansen H-C, Lagrèze W, Krueger O, Helmke K. Dependence of the optic nerve sheath diameter on acutely applied subarachnoidal pressure—an experimental ultrasound study. Acta Ophthalmol. 2011;89(6):e528–32.
Rajajee V, Fletcher J, Rochlen L, Jacobs T. Comparison of accuracy of optic nerve ultrasound for the detection of intracranial hypertension in the setting of acutely fluctuating vs stable intracranial pressure: post-hoc analysis of data from a prospective, blinded single center study. Crit Care. 2012;16(3):R79.
Chen H, Ding G-S, Zhao Y-C, Yu R-G, Zhou J-X. Ultrasound measurement of optic nerve diameter and optic nerve sheath diameter in healthy Chinese adults. BMC Neurol. 2015;15(1):106.
Maas AIR, Steyerberg EW, Butcher I, et al. Prognostic value of computerized tomography scan characteristics in traumatic brain injury: results from the IMPACT study. J Neurotrauma. 2007;24(2):303–14.
Miller MT, Pasquale M, Kurek S, et al. Initial head computed tomographic scan characteristics have a linear relationship with initial intracranial pressure after trauma. J Trauma. 2004;56(5):967–73.
Avanali R, Bhadran B, Panchal S, et al. Formulation of a three-tier cisternal grade as a predictor of in-hospital outcome from a prospective study of patients with traumatic intracranial hematoma. World Neurosurg. 2017;104:848–55.
Kouvarellis AJ, Rohlwink UK, Sood V, Van Breda D, Gowen MJ, Figaji AA. The relationship between basal cisterns on CT and time-linked intracranial pressure in paediatric head injury. Childs Nerv Syst. 2011;27(7):1139–44.
Zhang X, Medow JE, Iskandar BJ, et al. Invasive and noninvasive means of measuring intracranial pressure: a review. Physiol Meas. 2017;38(8):R143–82.
Fernando SM, Tran A, Cheng W, et al. Diagnosis of elevated intracranial pressure in critically ill adults: systematic review and meta-analysis. BMJ. 2019;366:l4225.
Gao Y, Li Q, Wu C, Liu S, Zhang M. Use of a Doppler-based pulsatility index to evaluate cerebral hemodynamics in neurocritical patients after hemicraniectomy. J Ultrasound Med. 2019;38(9):2469–75.
Ahmad M, Legrand M, Lukaszewicz A-C, Charlier P, Mateo J, Payen D. Transcranial Doppler monitoring may be misleading in prediction of elevated ICP in brain-injured patients. Intensive Care Med. 2013;39(6):1150–1.
Funding
There was no funding associated with this study.
Author information
Authors and Affiliations
Contributions
XX, KZ, and AT conceived and designed the study. YL and JL performed the experiments and analyzed the data. XX wrote the article. XX, RX, and AT reviewed and edited the manuscript. All authors discussed the results and approved the final manuscript.
Corresponding author
Ethics declarations
Conflicts of Interest
The authors declare that they have no conflicts of interest to this work.
Ethical Approval
This study was approved by the research ethics boards of Tongji Hospital Affiliated with Huazhong University of Science and Technology. According to the ethics standards of the institutional committee, the caregivers of all enrolled patients signed informed consent forms.
Informed Consent
We confirmed that this manuscript complies with all instructions to authors. All authors discussed the results and approved the manuscript. I would like to declare on behalf of my co-authors that the work described was original research that has not been published previously and not under consideration for publication elsewhere, in whole or in part.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Xu, X., Lu, Y., Liu, J. et al. Diagnostic Value of the Combination of Ultrasonographic Optic Nerve Sheath Diameter and Width of Crural Cistern with Respect to the Intracranial Pressure in Patients Treated with Decompressive Craniotomy. Neurocrit Care 39, 436–444 (2023). https://doi.org/10.1007/s12028-023-01711-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-023-01711-7