
Abstract
Background
The World Federation of Neurosurgical Societies (WFNS) scale is widely accepted for predicting outcomes for subarachnoid hemorrhage (SAH) patients. However, it is difficult to definitely predict outcomes for the most poor grade, WFNS grade 5. The present study aimed to investigate the prognostic ability of a novel classification using computed tomography perfusion (CTP) findings, called the cortical blood flow insufficiency (CBFI) scores.
Methods
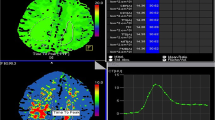
CTP was performed on admission for aneurysmal SAH followed by radical treatments within 72 hours of onset. Twenty-four cerebral cortex regions of interest (ROIs) were defined. CBFI was defined as Tmax > 4 s in each ROI, and CBFI scores were calculated based on the total number of ROIs with CBFI. Using the optimal cutoff value based on receiver operating characteristics (ROC) analysis to predict patient functional outcomes, CBFI scores were divided into “high” or “low” CBFI scores. Patient functional outcomes at 90 days were categorized based on modified Rankin Scale scores (0–3, favorable group; 4–6 unfavorable group) (0–4, non-catastrophic group; 5–6, catastrophic group).
Results
Fifty-seven patients were included in this study, of whom 21 (36.8%) and 13 (22.8%) were in the unfavorable and the catastrophic groups, respectively. A factor predicting unfavorable and catastrophic outcomes was CBFI score cutoff value of 7 points (area under the curve, 0.73 and 0.81, respectively). In multivariable logistic regression analysis for unfavorable outcome, high CBFI scores (odds ratio (OR), 8.6; 95% confidence interval (CI), 1.1–65.4; P = 0.04) and WFNS grade 5 (OR, 30.0; 95% CI, 4.5–201.0; P < 0.001) remained as independent predictors, while for catastrophic outcome, high CBFI scores (OR, 25.3; 95% CI, 3.3–194.0; P = 0.002) and age (OR, 1.1; 95% CI, 1.0–1.2; P = 0.02) remained as independent predictors. Conversely, WFNS grade 5 was not an independent predictor of catastrophic outcomes (OR, 3.8; 95% CI, 0.6–24.0; P = 0.15). In high CBFI scores, the OR of the delayed cerebral ischemia (DCI) occurrence was 9.6 (95% CI, 1.5–61.4; P = 0.02) after adjusting for age.
Conclusion
High CBFI scores could predict unfavorable and catastrophic outcomes for aneurysmal SAH patients and DCI occurrence.





Similar content being viewed by others

References
Connolly ES, Rabinstein AA, Carhuapoma JR, Derdeyn CP, Dion J, Higashida RT, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a guideline for healthcare professionals from the american heart association/american stroke association. Stroke. 2012;43:1711–37.
Steiner T, Juvela S, Unterberg A, Jung C, Forsting M, Rinkel G. European stroke organization guidelines for the management of intracranial aneurysms and subarachnoid haemorrhage. Cerebrovasc Dis. 2013;35:93–112.
de Oliveira Manoel AL, Goffi A, Marotta TR, Schweizer TA, Abrahamson S, Macdonald RL. The critical care management of poor-grade subarachnoid haemorrhage. Crit Care. 2016;20:21.
Frontera JA, Ahmed W, Zach V, Jovine M, Tanenbaum L, Sehba F, et al. Acute ischaemia after subarachnoid haemorrhage, relationship with early brain injury and impact on outcome: a prospective quantitative MRI study. J Neurol Neurosurg Psychiatry. 2015;86:71–8.
Cahill WJ, Calvert JH, Zhang JH. Mechanisms of early brain injury after subarachnoid hemorrhage. J Cereb Blood Flow Metab. 2006;26:1341–53.
Drake C. Report of world federation of neurological surgeons committee on a universal subarachnoid hemorrhage grading scale. J Neurosurg. 1988;68:985–6.
Haley EC, Kassell NF, Torner JC. The international cooperative study on the timing of aneurysm surgery: the North American experience. Stroke. 1992;23:205–14.
Wostrack M, Sandow N, Vajkoczy P, Schatlo B, Bijlenga P, Schaller K, et al. Subarachnoid haemorrhage WFNS grade V: is maximal treatment worthwhile? Acta Neurochir. 2013;155:579–86.
de Oliveira Manoel AL, Mansur A, Silva GS, Germans MR, Jaja BNR, Kouzmina E, et al. Functional outcome after poor-grade subarachnoid hemorrhage: a single-center study and systematic literature review. Neurocrit Care. 2016;25:338–50.
Hoogmoed J, van den Berg R, Coert BA, Rinkel GJE, Vandertop WP, Verbaan D. A strategy to expeditious invasive treatment improves clinical outcome in comatose patients with aneurysmal subarachnoid haemorrhage. Eur J Neurol. 2017;24:82–9.
Ahn S-H, Savarraj JP, Pervez M, Jones W, Park J, Jeon S-B, et al. The subarachnoid hemorrhage early brain edema score predicts delayed cerebral ischemia and clinical outcomes. Neurosurgery. 2018;83:137–45.
Malinova V, Iliev B, Tsogkas I, Rohde V, Psychogios M-N, Mielke D. Assessment of tissue permeability by early CT perfusion as a surrogate parameter for early brain injury after subarachnoid hemorrhage. J Neurosurg. 2019;1:1–6.
Duan Y, Xu H, Li R, Zheng K, Hu Z, Wu N, et al. Computed tomography perfusion deficits during the baseline period in aneurysmal subarachnoid hemorrhage are predictive of delayed cerebral ischemia. J Stroke Cerebrovasc Dis. 2017;26:162–8.
Sasahara A, Suzuki K, Takahashi Y, Koseki H, Hirota K, Ohbuchi H, et al. Prognostic assessment of aneurysmal subarachnoid patients with WFNS grade v by CT perfusion on arrival. World Neurosurg. 2016;92:1–6.
Boulouis G, Labeyrie MA, Raymond J, Rodriguez-Régent C, Lukaszewicz AC, Bresson D, et al. Treatment of cerebral vasospasm following aneurysmal subarachnoid haemorrhage: a systematic review and meta-analysis. Eur Radiol. 2017;27:3333–42.
Vergouwen MDI, Vermeulen M, van Gijn J, Rinkel GJE, Wijdicks EF, Muizelaar JP, et al. Definition of delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage as an outcome event in clinical trials and observational studies: proposal of a multidisciplinary research group. Stroke. 2010;41:2391–5.
van Swieten JC, Koudstaal PJ, Visser MC, Schouten HJ, van Gijn J. Interobserver agreement for the assessment of handicap in stroke patients. Strok. 1988;19:604–7.
Murayama K, Katada K, Hayakawa M, Toyama H. Shortened mean transit time in ct perfusion with singular value decomposition analysis in acute cerebral infarction: quantitative evaluation and comparison with various ct perfusion parameters. J Comput Assist Tomogr. 2017;41:173–80.
Barber PA, Demchuk AM, Zhang J, Buchan AM. Validity and reliability of a quantitative computed tomography score in predicting outcome of hyperacute stroke before thrombolytic therapy. Lancet. 2000;355:1670–4.
Olivot JM, Mlynash M, Thijs VN, Kemp S, Lansberg MG, Wechsler L, et al. Optimal tmax threshold for predicting penumbral tissue in acute stroke. Stroke. 2009;40:469–75.
Kanda Y. Investigation of the freely available easy-to-use software “EZR” for medical statistics. Bone Marrow Transpl. 2013;48:452–8.
Jaja BNR, Saposnik G, Lingsma HF, Macdonald E, Thorpe KE, Mamdani M, et al. Development and validation of outcome prediction models for aneurysmal subarachnoid haemorrhage: the SAHIT multinational cohort study. BMJ. 2018;360:j5745.
Hadeishi H, Suzuki A, Yasui N, Hatazawa J, Shimosegawa E, Awad IA, et al. Diffusion-weighted magnetic resonance imaging in patients with subarachnoid hemorrhage. Neurosurgery. 2002;50:741–8.
Satomi J, Hadeishi H, Yoshida Y, Suzuki A, Nagahiro S. Histopathological findings in brains of patients who died in the acute stage of poor-grade subarachnoid hemorrhage. Neurol Med Chir. 2016;56:766–70.
Ransom ER, Mocco J, Komotar RJ, Sahni D, Chang J, Hahn DK, et al. External ventricular drainage response in poor grade aneurysmal subarachnoid hemorrhage: effect on preoperative grading and prognosis. Neurocrit Care. 2007;6:174–80.
Fung C, Inglin F, Murek M, Balmer M, Abuisa J, Zgraggen WJ, et al. Reconsidering the logic of World Federation of Neurosurgical Societies grading in patients with severe subarachnoid hemorrhage. J Neurosurg. 2016;124:299–304.
Zeiler FA, Lo BWY, Akoth E, Silvaggio J, Kaufmann AM, Teitelbaum J, et al. Predicting Outcome in Subarachnoid Hemorrhage (SAH) Utilizing the full outline of unresponsiveness (FOUR) Score. Neurocrit Care. 2017;27:381–91.
Acknowledgments
The authors would like to thank Akio Katakata, Radiological Technologist, Fujita Health University School of Medicine for his invaluable support in the radiological study.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
JT, IN, SM and YH contributed conception and design of the study; JT organized the database; JT, YS, JM, JO, AH, TS, SW and KS contributed to the acquisition and analysis of the data; JT wrote the first draft of the manuscript; JT, IN, SM, TO and KM wrote sections of the manuscript. All authors contributed to manuscript revision, read and approved the submitted version.
Corresponding author
Ethics declarations
Conflict of interest
The author declares that they have no conflict of interest.
Ethical Approval/Informed Consent
The study protocol was approved by the institutional ethics committee (approval HM19-130), and written informed consent for participation was waived for this study in accordance with the national legislation and the institutional requirements.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Tanabe, J., Nakahara, I., Matsumoto, S. et al. Cortical Blood Flow Insufficiency Scores with Computed Tomography Perfusion can Predict Outcomes in Aneurysmal Subarachnoid Hemorrhage Patients: A Cohort Study. Neurocrit Care 34, 946–955 (2021). https://doi.org/10.1007/s12028-020-01108-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-020-01108-w