
Abstract
Background
Anterior cruciate ligament (ACL) injures incur over USD 2 billion in annual medical costs and prevention has become a topic of interest in biomechanics. However, literature conflicts persist over how knee rotations contribute to ACL strain and ligament injury. To maximize the efficacy of ACL injury prevention, the effects of underlying mechanics need to be better understood.
Questions/purposes
We applied robotically controlled, in vivo-derived kinematic stimuli to the knee to assess ligament biomechanics in a cadaver model. We asked: (1) Does the application of abduction rotation increase ACL and medial collateral ligament (MCL) strain relative to the normal condition? (2) Does the application of internal tibial rotation impact ACL strain relative to the neutral condition? (3) Does combined abduction and internal tibial rotation increase ligament strain more than either individual contribution?
Methods
A six-degree-of-freedom robotic manipulator was used to position 17 cadaveric specimens free from knee pathology outside of low-grade osteoarthritis (age, 47 ± 8 years; 13 males, four females) into orientations that mimic initial contact recorded from in vivo male and female drop vertical jump and sidestep cutting activities. Four-degree rotational perturbations were applied in both directions from the neutral alignment position (creating an 8° range) for each frontal, transverse, and combined planes while ACL and MCL strains were continuously recorded with DVRT strain gauges implanted directly on each ligament. Analysis of variance models with least significant difference post hoc analysis were used to assess differences in ligament strain and joint loading between sex, ligament condition, or motion task and rotation type.
Results
For the female drop vertical jump simulation in the intact knee, isolated abduction and combined abduction/internal rotational stimuli produced the greatest change in strain from the neutral position as compared with all other stimuli within the ACL (1.5% ± 1.0%, p ≤ 0.035; 1.8% ± 1.3%, p ≤ 0.005) and MCL (1.8% ± 1.0%, p < 0.001; 1.6% ± 1.3%, p < 0.001) compared with all other applied stimuli. There were no differences in mean peak ACL strain between any rotational stimuli (largest mean difference = 2.0%; 95% confidence interval [CI], −0.9% to 5.0%; p = 0.070). These trends were consistent for all four simulated tasks. Peak ACL strain in the intact knee was larger than peak MCL strain for all applied rotational stimuli in the drop vertical jump simulations (smallest mean difference = 2.1%; 95% CI, −0.4% to 4.5%; p = 0.047).
Conclusions
Kinematically constrained cadaveric knee models using peak strain as an outcome variable require greater than 4° rotational perturbations to elicit changes in intraarticular ligaments.
Clinical Relevance
Because combined rotations and isolated abduction produced greater change in strain relative to the neutral position for the ACL and MCL than any other rotational stimuli in this cadaver study, hypotheses for in vivo investigations aimed toward injury prevention that focuses on the reduction of frontal plane knee motion should be considered. Furthermore, reduced strain in the MCL versus the ACL may help explain why only 30% of ACL ruptures exhibit concomitant MCL injuries.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
In the knee, the anterior cruciate ligament (ACL) serves as the primary soft tissue restraint to anterior tibial translation and a secondary restraint to motion in additional degrees of freedom, whereas the medial collateral ligament (MCL) is aligned to primarily resist abduction [12, 14, 39]. Within the past 20 years, robotic methods of joint articulation have allowed investigators to examine the underlying mechanical behaviors through more physiologic simulations of activities of daily living on cadaveric specimens [12, 23, 26, 39]. These in vitro data would be unobtainable in vivo as a result of the invasive nature of biomechanical testing. Much of this work has evaluated and improved the efficaciousness of surgical methods and graft material selections used in ACL reconstructions with respect to native ACL biomechanics [12, 15, 19, 20, 28, 35, 43, 49, 51, 56,57,58]. These simulations have also gathered data on the mechanical contributions of the intact ACL in response to Lachman’s and pivot shift tests [15, 19, 20, 28, 35, 43, 49, 51, 56,57,58], gait cycles [23, 39], and landing impact forces [32, 40, 41, 46, 52, 53]. The accrued data have advanced the knowledge of ACL function and provided a baseline of comparison by which to evaluate the effectiveness of ACL injury treatments.
One goal of in vitro knee simulations has been identification of primary mechanical precursors to ACL injury. Unfortunately, data extracted from various experimental methods of mechanical knee simulations lack consistency [6, 32, 40, 41, 45]. Impact simulators and robotic articulation models have documented that combined knee abduction and internal rotations place the greatest mechanical demand on the ACL [41, 45, 50]. Robotic manipulators capable of force-torque and position control have demonstrated that knee abduction has a greater impact on the mechanical loading of the ACL than internal tibial rotation [5], whereas some simulations driven by pulse loads and torque transformers have indicated the opposite [40, 41]. This disparity may be caused by fundamental differences in simulation methods that lead to varying degrees of physiological accuracy [5]. It is important to accurately identify the underlying contributors to ACL loading during physiologic tasks because this knowledge could be extrapolated to improve the efficacy of injury prevention and rehabilitation techniques. Most models that have quantified mechanical contributions to ligament load and strain are constrained via a combination of force, torsional, and anatomic restrictions [5, 15, 19, 20, 28, 32, 35, 40, 41, 43, 46, 49, 51,52,53, 56,57,58]. Only limited literature is available pertaining to models of dynamic tasks that are precision constrained relative to in vivo kinematics [6,7,8,9, 23]. Accordingly, there is a gap in knowledge regarding the quantification of how a precise, physiologically relevant kinematic perturbation influences change on these in vitro models.
The purpose of this study was to apply robotically controlled kinematic stimuli to joint orientations derived from in vivo-recorded athletic activities to determine the effects of abduction, internal, and combined rotations on knee ligament biomechanics. We asked: (1) Does the application of abduction rotation increase ACL and MCL strain relative to the normal condition? (2) Does the application of internal tibial rotation impact ACL strain relative to the neutral condition? (3) Does combined abduction and internal tibial rotation increase ligament strain more than either individual contribution?
Patients and Methods
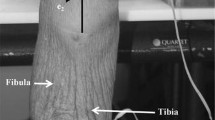
Twenty-one lower extremity cadaver specimens from 13 unique subjects (age, 48 ± 7 years; mass, 85 ± 20 kg; nine males, four females) were acquired from an anatomic donations program (Anatomical Gifts Registry, Hanover, MD, USA). Four specimens were excluded as a result of specimen failure during testing, preexisting ACL damage, or a nonfunctional ACL, leaving 17 specimens from 11 unique donors for data analysis. Specimens were then randomized into either an ACL (N = 9; age, 47 ± 8 years; mass, 86 ± 22 kg) or MCL group (N = 8; age, 48 ± 8 years; mass, 87 ± 20 kg) while ensuring that contralateral pairs were separated such that the right and left legs from a single donor would be placed into opposite groups. Using a six-degree-of-freedom (6-DOF) robotic manipulator (KR 210; KUKA Robotics Corp, Clinton Township, MI, USA) mounted with a six-axis load cell (Theta Model; ATI Industrial Automation, Apex, NC, USA), specimens were positioned in orientations associated with initial ground contact during athletic tasks. These orientations were derived from three-dimensional (3-D), in vivo motion capture kinematics. From this baseline orientation, each limb was articulated through rotational kinematics that have been associated with ACL injury risk or ACL deficiency (ACLD). Specimens were simulated through this protocol in the intact condition and then in an isolated ACL or isolated MCL condition, dependent on group randomization. During testing, the load cell recorded joint forces and torques while 3-mm microminiature differential variable strain transducers (DVRT®, LORD; MicroStrain Inc, Williston, VT, USA) recorded ACL and MCL strain. DVRTs were implanted on the proximal third of the anteromedial bundle of the ACL and across the joint line in the midsubstance of the MCL as specified in previous literature [6, 7, 32]. Explicit details of the robotics model utilized were previously published and are briefly conceptually described subsequently [6].
Kinematic Model
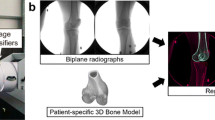
The acquisition of 3-D motion data and its conversion into input for in vitro robotic simulations have been previously documented [6, 16]. Briefly, 3-D motion capture was performed at 240 Hz by a 10-camera system (Eagle Cameras; Motion Analysis Corp, Santa Rosa, CA, USA) on a male (age, 24 years; height, 175 cm; mass, 69 kg) and female (age, 25 years; height, 170 cm; mass, 64 kg) subject that were matched for age, mass, height, and level of athletic activity. These positional data were truncated to landing phase [2] and then filtered at 6 Hz and processed through an established biomechanical model in Visual3D (Version 4.0; C-Motion, Inc, Germantown, MD, USA) to calculate joint kinematics [16]. Resultant kinematics from the knee were mathematically adjusted to minimize the impact of skin-marker artifact errors during the execution of robotic simulations [6]. These adjusted kinematics represent the input that was used to direct joint positioning in our robotic simulation. Previous literature has demonstrated that athletes can be classified into tertiles of relative risk for injury based on the joint mechanics they demonstrate while performing drop vertical jump (DVJ) tasks. This classification is largely based on the peak knee abduction moment calculated in Visual3D during landing, which has been directly associated with risk for ACL rupture [3, 24, 36]. Based on these tertiles of injury risk classification, the male subject used for kinematic model development exhibited low potential of injury risk, whereas the female subject used for kinematic model development exhibited high potential for injury risk.
An explicit account of specimen preparation procedures was previously documented [6, 23]. Specimen criteria were defined as no history of knee trauma, knee surgery, bone cancer, or ankle or shin implants. The limbs were kept frozen at −20° C and allowed to thaw the day before testing. The specimen was resected of all soft tissue down to the knee capsule, leaving the collateral and cruciate ligaments and menisci intact. Anatomic landmarks were marked and used to define the tibial joint coordinate system [21]. Using this system, custom biomechanical fixtures were affixed around the tibia, which was then rigidly mounted to the load cell on the robot end effector such that the tibia, load cell, and robot axes were all aligned. The tibial joint center point was digitized with a coordinate measuring machine (Faro Digitizer F04L2; FARO Technologies Inc, Lake Mary, FL, USA) and all rotations, translations, forces, and torques were applied or recorded about this point. Mounted specimens were articulated to 45°, because the ACL is likely minimally loaded in this position [47], and DVRTs were implanted on the ACL and MCL using previously described techniques [10, 32]. For the initial position of each simulated task, the in vitro limb orientation of all three rotational DOFs was verified to be within 0.5° of the initial contact limb orientation that was respectively recorded from both of the in vivo subjects. At this point, the limbs were cycled through the simulation kinematics beginning with no initial compressive force applied to the joint. The initial compressive force was then incrementally increased between cycles until a six-axis load cell mounted on the end effector of the robotic manipulator measured an overall peak compressive force of 2.0 to 2.5 body weight during the simulated DVJ tasks. This force range represents the peak single-leg vertical ground reaction force generated in vivo when landing from a DVJ [2]. Similarly, a peak force of 1.5 to 2.0 body weight was attained for sidestep cut tasks.
Robot Simulation
All tests were performed at room temperature and the joint was consistently hydrated with saline. Initial contact orientation for four athletic tasks (male DVJ, male sidestep cut, female DVJ, female sidestep cut) was simulated on each specimen in a randomized order, regardless of specimen sex. The initial position was used as a starting orientation to cycle a series of rotational adjustments (± 4° isolated knee abduction, ± 4° isolated internal tibial rotation, ± 4° combined abduction and internal rotations). These kinematic adjustments were selected because they represent DOFs where the ACL resists knee motion and are associated with either ACL injury risk or ACLD [1, 12, 24, 37, 38, 45, 52]. A ± 4° rotational shift will create an 8° range for knee abduction angles at initial contact, which has been reported as the mean difference between athletes who went on to ACL injury and healthy control subjects [24]. A ± 4° change in internal rotation is representative of the additional tibial motion observed in ACL-deficient subjects during gait [1]. Finally, valgus collapse, defined as the combination of knee abduction and internal rotation of the tibia [44], is cited in most retrospective video analyses of noncontact ACL ruptures [11, 25, 42]. These rotational adjustments were cycled from initial contact orientation because pilot testing revealed that is where peak ACL strain is most likely to occur and injury onset studies suggest that ACL ruptures occur immediately after initial contact in a position of limited flexion [30]. This description is best matched by our initial contact orientations, all of which expressed between 10° and 22° of knee flexion. To minimize viscoelastic effects, 10 preconditioning cycles were simulated before the 10-cycle set where forces, torques, and strains were recorded. After all cycling was completed, the specimen was manually articulated to the initial position for the next task and the process was repeated. Once all simulations were performed on the intact knee, the specimen was resected of all soft tissue and the distal portions of the femoral condyles such that the only load-bearing structure remaining in the knee was the ACL or MCL, dependent on specimen group randomization. All simulations were repeated in this isolated ligament condition (Fig. 1). After simulation, the joint was returned to initial contact orientation, compressed to an unloaded position, and slowly distracted along a linear path to identify the neutral strain position of the ligament. Because the isolated ligament was the only intact load-bearing structure remaining across the joint, any magnitude of constantly maintained distraction force achieved while moving across this linear path would indicate the position at which the ligament transitioned from lax to taut. This transition was defined as the neutral strain point and was identified when the force sensors first registered a constant distraction force > 5 N. The remaining ligament was then resected and all simulations were repeated in a bone-only condition to be subtracted out as gravity contributions during data analysis.

Graph outlines the cadaveric model used in this investigation. For each specimen, all simulation conditions were applied to the intact knee (n = 11) as well as either the isolated ACL knee (n = 9) or isolated MCL knee (n = 8), dependent on group randomization.
Data Analysis
Having identified the neutral strain inflection point of the ACL and MCL, ligament strains were reported as absolute values rather than changes relative to the DVRT insertion orientation. This eliminated a limitation typical of in vitro ligament strain assessments [32, 40, 41, 52]. The eighth and ninth cycles of each 10-cycle set were used for analysis to mitigate cycle effects. All data points were time-normalized to percentage of landing phase for each task. Data from the intact knee portion of the model were analyzed across the whole population cohort; however, before analysis, data points from each contralateral pair were averaged so that the contralateral pairs would not have a weighted effect on calculations. Averaging contralateral pairs was justified because contralateral limbs express a lack of mechanical differences in robotic simulations [4]. For the isolated ligament portion of the model, ACL and MCL groups were compared as randomized previously. A 2 × 7 analysis of variance with a Bonferroni post hoc analysis was used to evaluate differences in ligament strain between ligaments (ACL, MCL) relative to each of the rotational stimuli applied to the joint (neutral, internal rotation, external rotation, knee abduction, knee adduction, combined abduction/internal rotation, and combined adduction/external rotation). Ligament of interest and rotation applied were independent variables, whereas ligament strains were dependent variables. In all models, each of the four motion tasks simulated were assessed separately from one another. Significance was determined at α < 0.05. All statistical analyses were performed in JMP Pro (Version 10.0.0; SAS Institute Inc, Cary, NC, USA). Effect size for the group with the smallest difference from neutral was 0.47, as determined from the raw data. Based on the 2 × 7 ANOVA model, G*Power (version 3.1.9.2; Universität Düsseldorf, Düsseldorf, Germany) indicated that a sample size of six per group would be needed to achieve 0.8 power. The minimum group size was eight for the MCL group (with nine for the ACL group and 11 for both groups in the intact knees). Therefore, the present analyses were sufficiently powered.
Results
For consistency, all example values presented in the results text were derived from the female DVJ simulation. For ACLs in the intact knees, there were no differences in mean ACL strain between each of the applied rotational stimuli, including the neutral position (largest mean difference was between isolated external and combined abduction/internal rotations, 2.3%; 95% confidence interval [CI], −0.3% to 4.3%; p = 0.08; Table 1). However, there were differences in the magnitude of change induced on ACL strain between the various rotational stimuli (abduction versus internal rotation mean difference, 2.3%; 95% CI, 1.4%–3.2%; p < 0.001; combined abduction/internal versus internal rotation mean difference, 1.3%; 95% CI, 0.4%–2.2%; p = 0.003; Table 2). For the intact knee condition, knee abduction (1.5% ± 1.0%) and combined knee abduction/internal rotation (1.8% ± 1.3%) fostered a greater change in ACL strain as compared with any other remaining stimuli (smallest mean difference, 1.0%; 95% CI, 0.1%–2.0%; p = 0.005; Table 2). External rotation was the only condition that induced strain relaxation on the ACL (smallest mean difference, 0.7%; 95% CI, −0.2% to 1.6%; p = 0.049).
Absolute MCL strains were smaller than ACL strains in the intact knee relative to positional external stimuli (mean difference, 3.2%; 95% CI, 1.2%–5.3%; p = 0.004), isolated external (mean difference, 2.8%; 95% CI, 0.7%–4.9%; p = 0.001), isolated internal (mean difference, 3.6%; 95% CI, 1.6%–5.7%; p = 0.001), isolated adduction (mean difference, 4.8%; 95% CI, 2.4%–7.1%; p < 0.001), combined abduction/internal (mean difference, 3.1%; 95% CI, 0.8%–5.5%; p = 0.012), and combined adduction/external (mean difference, 4.2%; 95% CI, 1.9%–6.6%; p = 0.001) rotations (Tables 1, 3). Within the MCL, isolated abduction produced strains of 2.1% ± 2.8% and combined abduction/internal produced strains of 2.0% ± 2.6%, while isolated adduction produced strains of −0.6% ± 2.7% and combined adduction/external produced strains of −0.8% ± 2.5%; however, these were found to have no difference from one another (smallest mean difference, 2.5%; 95% CI, −0.3% to 5.4%; p = 0.201; Table 3). These rotations acted in opposing manners because abduction increased MCL strain relative to neutral and adduction decreased MCL strain relative to neutral. Similarly, the magnitude of change in MCL strain relative to the neutral position was greater for abduction and combined abduction/internal rotation than for any other rotation (smallest mean difference, 1.6%; 95% CI, 0.7%–2.5%; p < 0.001; Table 4). Isolated adduction and combined adduction/external DOFs removed all load to the MCL in the intact knee because they produced negative absolute strain values. When specimens were resected down to the MCL-isolated condition, the MCL remained unstrained throughout most rotational stimuli with the exception of minimal strain occurring during abduction and combined abduction/internal rotation.
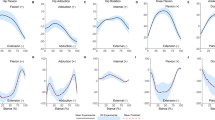
Transverse plane stimuli had a greater magnitude of change in ACL strain (internal rotation = 0.5% ± 0.4%, external rotation = −0.5% ± 0.2%) than MCL strain (internal rotation = 0.1% ± 0.2%, external rotation = 0.0% ± 0.1%; p = 0.002 and p < 0.001, respectively; Tables 2, 4; Figs. 2, 3). Likewise, change in strain relative to the neutral orientation was different between ligaments when adduction stimuli were applied, because they increased strain in the ACL (0.8% ± 0.7%), but decreased strain in the MCL (−0.9% ± 0.8%, p < 0.001). In the intact knee, there were no differences in the magnitude of change in strain between ligaments caused by abduction stimuli (ACL = 1.6% ± 1.0%, MCL = 1.8% ± 1.0%; p = 0.601). However, for the isolated ligament condition, the MCL experienced greater change in strain from abduction stimuli (2.2% ± 1.1%) than did the ACL (−0.1% ± 0.3%; p < 0.001).


Discussion
Despite the high cost and prevalence of ACL injuries, debate continues over which underlying mechanical factors contribute most substantially to ligament loading during injury. Because most intraarticular knee models use torsional or external load constraints, this study, to our knowledge, presents the first investigation of ACL and MCL strain response to kinematically restrained perturbations applied to the knee relative to an in vivo-derived initial contact position. Because clinical ACL injuries occur within the first 50 msec of contact [29], investigation of ligamentous response to perturbation in initial contact orientations should prove relevant to injury mechanics. The rotational perturbations selected have been identified as contributors to ACL strain [32, 40, 41, 50, 52], motions secondarily resisted by the ACL [12], or (in the case of knee abduction) predictors of ACL injury risk [13]. The minor alterations in absolute ACL strain induced by the presently applied rotational stimuli were not found to be different from strain magnitudes recorded at the neutral limb position. However, the magnitude of change induced on ACL strain in the intact knee was greater for pure abduction and combined abduction/internal rotations than any other DOF. Thus, this finding partially supports the hypotheses that combined abduction/internal rotation would increase ligament strain greater than any individual DOF and that pure internal rotation would have a lesser impact on ACL strain as compared with matched magnitudes of pure abduction rotation. In previous investigations, combined rotational stimuli have had a greater impact on ACL strain than rotations in any individual DOF. This has been documented in computational models [50], impact testing [32, 40, 41], and robotic manipulator-driven articulations [5].
A limitation of the current investigation is that the applied stimuli are nonphysiologic. Rarely in dynamic activity is rotation strictly confined to a single plane of motion. However, like clinical examinations such as the Lachman’s test, the current motions can still prove valuable in the assessment of functional ligament mechanics. Numerous investigators have used robotically simulated Lachman’s tests of pure anterior drawer to quantify ACL mechanics in the same fashion that the current study evaluates rotational perturbations [5]. Furthermore, the present results maintain clinical relevance because each stimuli is tested individually, but also in conjunction with one another, which is more representative of the physiologic condition where dynamic knee valgus is comprised of knee abduction combined with internal tibial rotation. A second limitation exists in the biologic variability in ACL mechanical behavior. Robotic manipulators are highly precise systems capable of reproducing movements with minimal error [17, 18]. However, previous investigations have indicated that the average ACL ruptures at 19% ± 10% strain, whereas individually these failures occur between 7% and 36% [32]. This presents a large natural variability in ACL strain between specimens. Furthermore, substantial biologic variability in loading outcomes has also been denoted in previous robotic manipulator applications [54]. As such, despite robotic manipulator precision, the biologic variability present in ACL mechanical properties between specimens may have created SDs large enough to preclude statistical significance at the strain magnitudes exhibited in this study. Post hoc power analysis (based on Table 1) indicated the effect size between isolated internal rotation stimuli and combined abduction/internal rotation stimuli was 0.44, which would have necessitated 114 specimens per group to achieve significance. This is both implausible and impractical to execute in a cadaveric study. Had the magnitude of rotational stimuli been increased to 8° in each direction, rather than an 8° total range centered around neutral, the data likely would have had an increased effect size and potentially exhibited additional differences between types of stimuli applied. Furthermore, the absence of differences in peak strain between applied rotational stimuli (Tables 1, 3) may be the result of limitations of DVRT implantation. Although the gauges were barbed and sutured in place, the ACL is not a rigid structure and allows either end of the sensor some movement within the implantation site. With the relatively small changes that were documented in ACL strain (< 2.0%), increased variation could mask the overall magnitude of change in some specimens. However, from a magnitude standpoint, the mean magnitude of change induced by combined abduction/internal rotations on ACL strain was 239% of internal rotation and 116% of abduction.
Frontal plane rotations of 4° did not affect differences in peak strain relative to the neutral orientation in the ACL or MCL, but abduction stimuli did elicit a greater change in strain than any other isolated rotation. This finding is similar to previous literature that demonstrated rotational offsets of 0.5° applied to the initial contact position had limited influence on knee kinetics during simulated gait [22]. However, kinetically controlled robotic models have demonstrated that 5-Nm increases in abduction torque result in additional anterior tibial translations and ACL force [5]. The MCL serves as the primary ligamentous resistor to knee abduction rotation [12]. This was corroborated in the present study, because isolated abduction and combined abduction/internal stimuli produced greater MCL strains than all other DOFs. No other rotational stimuli expressed a difference from one another or from the neutral orientation. Peak MCL strains during combined abduction/internal rotations were smaller than ACL strains. As a whole, when differences were identified between ligaments in corresponding DOFs, peak MCL strains were smaller than comparable ACL strains (Tables 1, 3). Despite that both ligaments resist the knee abduction rotation that is commonly associated with ACL injury [12, 24, 50], MCL failures only occur in approximately 30% to 40% of noncontact ACL injuries [31, 34, 48]. The generally reduced peak strain of the MCL in the intact knee that was expressed in the current study may help explain why the MCL is often resistant to injury in scenarios that produce ACL failure.
Transverse plane rotations did not affect differences in peak strain relative to the neutral orientation in the ACL or MCL. This finding is affirmed by kinetically driven robotic models because the application of internal tibial torsion to weightbearing knees did not affect ACL load and did not increase internal tibial rotation in ACL-deficient knees compared with ACL-intact knees [33, 55]. Particularly for the MCL in the isolated ligament condition, all transverse plane stimuli resulted in negative strain values, which indicated the ligament was slack and not bearing load from the perturbation (Table 3). For both ligaments, the change in strain induced by transverse plane rotations was less than frontal plane or combined stimuli involving knee abduction. Such behavior is corroborated by injury landing simulations where abduction had a substantially greater effect size on peak ACL strain than internal rotation [27]. The correlation between internal rotation and peak ACL strain observed in this injury simulation could be the result of the magnitude of stimuli because that model generated as much as 39° (3.7°) of internal tibial rotation, which is nearly 10× the perturbation utilized in the current investigation.
Combined 4° rotational stimuli did not affect differences in peak strain relative to neutral orientation in the ACL or MCL; however, comparable to isolated abduction, combined abduction/internal rotation stimuli elicited a greater change in strain for both ligaments than any other stimuli. In previous robotic, impact, and injury simulations, combined rotations have had a greater influence in intraarticular knee mechanics than either stimuli alone [5]. Because the present model provided a uniquely kinematically constrained simulation, it is possible that the magnitude of applied perturbation selected was not sufficient to elicit physiologically significant changes. None of the ACL strain values generated in the present study approached previously documented ligament failure strains. In drop landings simulated on cadaveric specimens, implanted DVRTs reported mean ACL failure strain of 19% [32]. These injuries were induced immediately after contact in limbs that were positioned relative to in vivo initial contact orientations. Similarly, as presented in previous literature [6], specimens in the present study were also positioned relative to in vivo initial contact orientations; however, the largest mean ACL strain documented was 5%. This value would be expected to increase if the range of applied rotational stimulus was expanded. An 8° increase in abduction rotation at initial contact has been prospectively linked with likelihood of ACL injury [13]. To reproduce that 8° range without risk of specimen damage, the present investigation deviated by 4° on either side of neutral for each plane of rotation. Relative to the ACL, this magnitude of deviation created differences in the delta strain values, but not in mean strains among the various applied stimuli. As noted, application of an expanded 8° stimulus on either side of the neutral orientation for each plane of rotation would likely increase relative differences in peak ACL strain and may identify differences between the respective DOFs.
In summary, when cadaveric specimens were simulated from initial contact orientations associated with in vivo athletic tasks, isolated abduction and combined abduction/internal rotation stimuli produced larger magnitudes of change in strain for the ACL and MCL than isolated internal rotation, despite that peak strain differences were absent between stimuli in both the ACL and MCL. Therefore, reduction of knee valgus with attention to maintaining neutral knee alignment during athletic tasks should be a driving hypothesis focus of ACL injury prevention programs because frontal plane rotations induced the greatest changes in strain on cadaveric specimens compared with other rotational stimuli. In addition, the MCL generally expressed less absolute strain than the ACL in the presented orientations, which may be indicative of how and why ACL failure often occurs without concomitant MCL injury. Finally, future cadaveric models should implement larger magnitudes of perturbation than were used in the present model because such a change is likely to increase the effect size of the observed strain outcome measures.
References
Andriacchi TP, Dyrby CO. Interactions between kinematics and loading during walking for the normal and ACL deficient knee. J Biomech. 2005;38:293–298.
Bates NA, Ford KR, Myer GD, Hewett TE. Impact differences in ground reaction force and center of mass between the first and second landing phases of a drop vertical jump and their implications for injury risk assessment. J Biomech. 2013;46:1237–1241.
Bates NA, Hewett TE. Motion analysis and the anterior cruciate ligament: classification of injury risk. J Knee Surg. 2016;29:117–125.
Bates NA, McPherson AL, Nesbitt RJ, Shearn JT, Myer GD, Hewett TE. Robotic simulation of identical athletic-task kinematics on cadaveric limbs exhibits a lack of differences in knee mechanics between contralateral pairs. J Biomech. 2017;53:36–44.
Bates NA, Myer GD, Shearn JT, Hewett TE. Anterior cruciate ligament biomechanics during robotic and mechanical simulations of physiologic and clinical motion tasks: a systematic review and meta-analysis. Clin Biomech. 2015;30:1–13.
Bates NA, Nesbitt RJ, Shearn JT, Myer GD, Hewett TE. A novel methodology for the simulation of athletic tasks on cadaveric knee joints with respect to in vivo kinematics. Ann Biomed Eng. 2015;43:2456–2466.
Bates NA, Nesbitt RJ, Shearn JT, Myer GD, Hewett TE. Relative strain in anterior cruciate ligament and medial collateral ligament during simulated jump landing and sidestep cutting tasks: implications for injury risk. Am J Sports Med. 2015;43:2259–2269.
Bates NA, Nesbitt RJ, Shearn JT, Myer GD, Hewett TE. Posterior tibial slope angle correlates with peak sagittal and frontal plane knee joint loading during robotic simulations of athletic tasks. Am J Sports Med. 2016;44:1762–1770.
Bates NA, Nesbitt RJ, Shearn JT, Myer GD, Hewett TE. Sex-based differences in knee ligament biomechanics during robotically simulated athletic tasks. J Biomech. 2016;49:1429–1436.
Beynnon B, Howe JG, Pope MH, Johnson RJ, Fleming BC. The measurement of anterior cruciate ligament strain in vivo. Int Orthop. 1992;16:1–12.
Boden BP, Torg JS, Knowles SB, Hewett TE. Video analysis of anterior cruciate ligament injury: abnormalities in hip and ankle kinematics. Am J Sports Med. 2009;37:252–259.
Boguszewski DV. Characterizing the porcine knee as a biomechanical surrogate model of the human knee to study the anterior cruciate ligament. Biomed Engineering. Cincinnati, OH, USA: University of Cincinnati; 2012:163.
Brent JL, Ford KR, Myer GD, Harrison AD, Hewett TE. Reliability of single leg landings on a portable force platform. Med Sci Sports Exerc. 2005;37:400.
Butler DL, Noyes FR, Grood ES. Ligamentous restraints to anterior-posterior drawer in the human knee. A biomechanical study. J Bone Joint Surg Am. 1980;62:259–270.
Diermann N, Schumacher T, Schanz S, Raschke MJ, Petersen W, Zantop T. Rotational instability of the knee: internal tibial rotation under a simulated pivot shift test. Arch Orthop Trauma Surg. 2009;129:353–358.
Ford KR, Myer GD, Hewett TE. Reliability of landing 3D motion analysis: implications for longitudinal analyses. Med Sci Sports Exerc. 2007;39:2021–2028.
Fujie H, Livesay GA, Woo SL-Y, Kashiwaguchi S, Blomstrom G. The use of a universal force moment sensor to determine in situ forces in ligaments: a new methodology. J Biomech Eng. 1995;117:1–7.
Fujie H, Mabuchi K, Woo SL, Livesay GA, Arai S, Tsukamoto Y. The use of robotics technology to study human joint kinematics: a new methodology. J Biomech Eng. 1993;115:211–217.
Gadikota HR, Seon JK, Kozanek M, Oh LS, Gill TJ, Montgomery KD, Li G. Biomechanical comparison of single-tunnel-double-bundle and single-bundle anterior cruciate ligament reconstructions. Am J Sports Med. 2009;37:962–969.
Gadikota HR, Wu JL, Seon JK, Sutton K, Gill TJ, Li G. Single-tunnel double-bundle anterior cruciate ligament reconstruction with anatomical placement of hamstring tendon graft: can it restore normal knee joint kinematics? Am J Sports Med. 2010;38:713–720.
Grood ES, Suntay WJ. A joint coordinate system for the clinical description of three- dimensional motions: application to the knee. J Biomech Eng. 1983;105:136–144.
Herfat ST, Boguszewski DV, Nesbitt RJ, Shearn JT. Effect of perturbing a simulated motion on knee and anterior cruciate ligament kinetics. J Biomech Eng. 2012;134:104504.
Herfat ST, Boguszewski DV, Shearn JT. Applying simulated in vivo motions to measure human knee and ACL kinetics. Ann Biomed Eng. 2012;40:1545–1553.
Hewett TE, Myer GD, Ford KR, Heidt RS Jr, Colosimo AJ, McLean SG, van den Bogert AJ, Paterno MV, Succop P. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: a prospective study. Am J Sports Med. 2005;33:492–501.
Hewett TE, Torg JS, Boden BP. Video analysis of trunk and knee motion during non-contact anterior cruciate ligament injury in female athletes: lateral trunk and knee abduction motion are combined components of the injury mechanism. Br J Sports Med. 2009;43:417–422.
Howard RA, Rosvold JM, Darcy SP, Corr DT, Shrive NG, Tapper JE, Ronsky JL, Beveridge JE, Marchuk LL, Frank CB. Reproduction of in vivo motion using a parallel robot. J Biomech Eng. 2007;129:743–749.
Kiapour AM, Demetropoulos CK, Kiapour A, Quatman CE, Wordeman SC, Goel VK, Hewett TE. Strain response of the anterior cruciate ligament to uniplanar and multiplanar loads during simulated landings: Implications for injury mechanism. Am J Sports Med. 2016;44:2087–2096.
Kilger RH, Thomas M, Hanford S, Alaseirlis DA, Paessler HH, Woo SL. The effectiveness of reconstruction of the anterior cruciate ligament using the novel knot/press-fit technique: a cadaveric study. Am J Sports Med. 2005;33:856–863.
Krosshaug T, Nakamae A, Boden BP, Engebretsen L, Smith G, Slauterbeck JR, Hewett TE, Bahr R. Mechanisms of anterior cruciate ligament injury in basketball: video analysis of 39 cases. Am J Sports Med. 2007;35:359–367.
Krosshaug T, Slauterbeck JR, Engebretsen L, Bahr R. Biomechanical analysis of anterior cruciate ligament injury mechanisms: three-dimensional motion reconstruction from video sequences. Scand J Med Sci Sports. 2007;17:508–519.
LaPrade RF, Wentorf FA, Fritts H, Gundry C, Hightower CD. A prospective magnetic resonance imaging study of the incidence of posterolateral and multiple ligament injuries in acute knee injuries presenting with a hemarthrosis. Arthroscopy. 2007;23:1341–1347.
Levine JW, Kiapour AM, Quatman CE, Wordeman SC, Goel VK, Hewett TE, Demetropoulos CK. Clinically relevant injury patterns after an anterior cruciate ligament injury provide insight into injury mechanisms. Am J Sports Med. 2013;41:385–395.
Lo J, Muller O, Wunschel M, Bauer S, Wulker N. Forces in anterior cruciate ligament during simulated weight-bearing flexion with anterior and internal rotational tibial load. J Biomech. 2008;41:1855–1861.
Mei Y, Ao YF, Wang J-Q, Ma Y, Zhang X, Wang J-N, Zhu J-X. Clinical characteristics of 4355 patients with anterior cruciate ligament injury. Chin Med J (Engl). 2013;126:4487–4492.
Miura K, Woo SL, Brinkley R, Fu YC, Noorani S. Effects of knee flexion angles for graft fixation on force distribution in double-bundle anterior cruciate ligament grafts. Am J Sports Med. 2006;34:577–585.
Myer GD, Ford KR, Brent JL, Hewett TE. Differential neuromuscular training effects on ACL injury risk factors in ‘high-risk’ versus ‘low-risk’ athletes. BMC Musculoskelet Disord. 2007;8:1–7.
Myer GD, Ford KR, Khoury J, Succop P, Hewett TE. Clinical correlates to laboratory measures for use in non-contact anterior cruciate ligament injury risk prediction algorithm. Clin Biomech. 2010;25:693–699.
Myer GD, Ford KR, Khoury J, Succop P, Hewett TE. Biomechanics laboratory-based prediction algorithm to identify female athletes with high knee loads that increase risk of ACL injury. Br J Sports Med. 2011;45:245–252.
Nesbitt RJ, Herfat ST, Boguszewski DV, Engel AJ, Galloway MT, Shearn JT. Primary and secondary restraints of human and ovine knees for simulated in vivo gait kinematics. J Biomech. 2014;47:2022-2027.
Oh YK, Kreinbrink JL, Wojtys EM, Ashton-Miller JA. Effect of axial tibial torque direction on ACL relative strain and strain rate in an in vitro simulated pivot landing. J Orthop Res. 2012;30:528–534.
Oh YK, Lipps DB, Ashton-Miller JA, Wojtys EM. What strains the anterior cruciate ligament during a pivot landing? Am J Sports Med. 2012;40:574–583.
Olsen OE, Myklebust G, Engebretsen L, Bahr R. Injury mechanisms for anterior cruciate ligament injuries in team handball: a systematic video analysis. Am J Sports Med. 2004;32:1002–1012.
Petersen W, Tretow H, Weimann A, Herbort M, Fu FH, Raschke M, Zantop T. Biomechanical evaluation of two techniques for double-bundle anterior cruciate ligament reconstruction: one tibial tunnel versus two tibial tunnels. Am J Sports Med. 2007;35:228–234.
Quatman CE, Hewett TE. The anterior cruciate ligament injury controversy: is ‘valgus collapse’ a sex-specific mechanism? Br J Sports Med. 2009;43:328–335.
Quatman CE, Kiapour AM, Demetropoulos CK, Kiapour A, Wordeman SC, Levine JW, Goel VK, Hewett TE. Preferential loading of the ACL compared with the MCL during landing: a novel in sim approach yields the multiplanar mechanism of dynamic valgus during ACL injuries. Am J Sports Med. 2014;42:177–186.
Quatman CE, Quatman-Yates CC, Hewett TE. A ‘plane’ explanation of anterior cruciate ligament injury mechanisms: a systematic review. Sports Med. 2010;40:729–746.
Renstrom P, Arms SW, Stanwyck TS, Johnson RJ, Pope MH. Strain within the anterior cruciate ligament during hamstring and quadriceps activity. Am J Sports Med. 1986;14:83–87.
Sankar WN, Wells L, Sennett BJ, Wiesel BB, Ganley TJ. Combined anterior cruciate ligament and medial collateral ligament injuries in adolescents. J Pediatr Orthop. 2006;26:733–736.
Seon JK, Gadikota HR, Wu JL, Sutton K, Gill TJ, Li G. Comparison of single- and double-bundle anterior cruciate ligament reconstructions in restoration of knee kinematics and anterior cruciate ligament forces. Am J Sports Med. 2010;38:1359–1367.
Shin CS, Chaudhari AM, Andriacchi TP. Valgus plus internal rotation moments increase ACL strain more than either alone. Med Sci Sports Exerc. 2011;43:1484–1491.
Sim JA, Gadikota HR, Li JS, Li G, Gill TJ. Biomechanical evaluation of knee joint laxities and graft forces after anterior cruciate ligament reconstruction by anteromedial portal, outside-in, and transtibial techniques. Am J Sports Med. 2011;39:2604–2610.
Withrow TJ, Huston LJ, Wojtys EM, Ashton-Miller JA. The effect of an impulsive knee valgus moment on in vitro relative ACL strain during a simulated jump landing. Clin Biomech. 2006;21:977–983.
Withrow TJ, Huston LJ, Wojtys EM, Ashton-Miller JA. The relationship between quadriceps muscle force, knee flexion, and anterior cruciate ligament strain in an in vitro simulated jump landing. Am J Sports Med. 2006;34:269–274.
Woo SL-Y, Debski RE, Wong EK, Yagi M, Tarinelli D. Use of robotic technology for diarthrodial joint research. J Sci Med Sport. 1999;2:283–297.
Wunschel M, Muller O, Lo J, Obloh C, Wulker N. The anterior cruciate ligament provides resistance to externally applied anterior tibial force but not to internal rotational torque during simulated weight-bearing flexion. Arthroscopy. 2010;26:1520–1527.
Yamamoto Y. Knee stability and graft function after anterior cruciate ligament reconstruction: a comparison of a lateral and an anatomical femoral tunnel placement. Am J Sports Med. 2004;32:1825–1832.
Zamarra G, Fisher MB, Woo SL, Cerulli G. Biomechanical evaluation of using one hamstrings tendon for ACL reconstruction: a human cadaveric study. Knee Surg Sports Traumatol Arthrosc. 2010;18:11–19.
Zantop T, Diermann N, Schumacher T, Schanz S, Fu FH, Petersen W. Anatomical and nonanatomical double-bundle anterior cruciate ligament reconstruction: importance of femoral tunnel location on knee kinematics. Am J Sports Med. 2008;36:678–685.
Acknowledgments
We thank the support of the staff at the Sports Health and Performance Institute at The Ohio State University and the Sports Medicine Biodynamics Laboratory at Cincinnati Children’s Hospital.
Author information
Authors and Affiliations
Corresponding author
Additional information
This work was supported by National Institutes of Health/NIAMS Grants #R01-AR049735 (TEH), #R01-AR055563 (TEH), #R01-AR056660 (JTS), and #R01-AR056259 (TEH).
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research ® editors and board members are on file with the publication and can be viewed on request.
Clinical Orthopaedics and Related Research ® neither advocates nor endorses the use of any treatment, drug, or device. Readers are encouraged to always seek additional information, including FDA-approval status, of any drug or device prior to clinical use.
Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
This work was performed at the University of Cincinnati, Cincinnati, OH, USA.
About this article

Cite this article
Bates, N.A., Nesbitt, R.J., Shearn, J.T. et al. Knee Abduction Affects Greater Magnitude of Change in ACL and MCL Strains Than Matched Internal Tibial Rotation In Vitro. Clin Orthop Relat Res 475, 2385–2396 (2017). https://doi.org/10.1007/s11999-017-5367-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-017-5367-9