
Abstract
Crowding in Emergency Departments (EDs) has emerged as a global public health crisis. Current literature has identified causes and the potential harms of crowding in recent years. The way crowding is measured has also been the source of emerging literature and debate. We aimed to synthesize the current literature of the causes, harms, and measures of crowding in emergency departments around the world. The review is guided by the current PRIOR statement, and involved Pubmed, Medline, and Embase searches for eligible systematic reviews. A risk of bias and quality assessment were performed for each review, and the results were synthesized into a narrative overview. A total of 13 systematic reviews were identified, each targeting the measures, causes, and harms of crowding in global emergency departments. Key among the results is that the measures of crowding were heterogeneous, even in geographically proximate areas, and that temporal measures are being utilized more frequently. It was identified that many measures are associated with crowding, and the literature would benefit from standardization of these metrics to promote improvement efforts and the generalization of research conclusions. The major causes of crowding were grouped into patient, staff, and system-level factors; with the most important factor identified as outpatient boarding. The harms of crowding, impacting patients, healthcare staff, and healthcare spending, highlight the importance of addressing crowding. This overview was intended to synthesize the current literature on crowding for relevant stakeholders, to assist with advocacy and solution-based decision making.
Similar content being viewed by others


Introduction
Emergency Department (ED) crowding presents a global public health crisis and results from the inability of health care systems to provide adequate service, leaving the ED to serve as the safety valve for dysfunction or insufficient resources. ED crowding is defined as a situation where demand for emergency services exceeds the ability of an ED to provide care within an appropriate time frame [1]. Globally, several individual healthcare systems and the International Federation of Emergency Medicine have identified ED crowding as a public health concern and health equity issue [1,2,3].
A conceptual framework has been developed to classify and measure crowding within emergency departments. This framework includes three “buckets”: input, throughput, and output [4]. Input is defined as any factor that may increase the number of visitors to emergency departments, which can include a lack of access to primary care, an increase in the number of acutely presenting patients, and inefficient triage procedures [4, 5]. Throughput is defined as the flow of patients through the ED, which includes triage, time to diagnostic testing, and treatment [4]. Discharge of patients and movement to inpatient units represents the output component and represents a commonly cited reason for crowding in emergency departments [4, 6,7,8,9]. Output reflects challenges within healthcare systems as whole. This is especially emphasized considering when boarding of admitted inpatients within emergency departments is decreased, crowding and wait times are significantly reduced [4, 9].
The challenges for both staff and patients related to crowding and emergency department boarding were highlighted particularly during the COVID-19 pandemic, where ED crowding spiked due to access block and the transmissibility of the coronavirus [10]. Furthermore, access block causes a dose–response increase in the rate of mortality for patients boarded in emergency departments [7, 11].
Further harms associated with crowding and increased boarding in EDs include longer time to treatment, which may in turn impact disposition and chances of admission [12]. Crowding has also been shown to increase chances of return visits to emergency departments and increased healthcare utilization [13]. These outcomes are also not equal to every patient, the longstanding impacts of crowding have been shown to disproportionately impact disadvantaged populations to a greater degree [3].
The metrics of crowding have been measured and reported in several ways to optimize reporting of causes and harms of crowding. Metrics include patient flow in hospital beds, ED length of stay, or ED volume [5, 14]. These metrics were developed to assist in studying and understanding research to influence clinical practice guidelines.
There is a growing body of literature investigating the causes, measures, and harms of crowding in emergency departments. Approximately 200 total studies have been published yearly on emergency crowding in the last five years. Of these, approximately 20 are systematic reviews. The selected systematic reviews inform further research on interventions which may then be used to provide solutions to the current crisis of crowding in emergency departments. However, the global literature has not yet been summarized in an overview of reviews format, which aims to summarize the current state of the literature on these issues. While solutions for the crowding concerns may be local, there is a need for evidence-based decision making, thus data synthesis is useful in this field.
This overview of reviews seeks to synthesize the field of ED crowding with a focus on the causes, harms, and measures of overcrowding in emergency departments. This review will apply a global perspective and will cover facets of emergency department crowding from the perspective of input, throughput, and output. A second overview of reviews, which will analyze data from 2010 onwards, will focus on interventions and solutions and be presented in a subsequent paper.
Methods
We compiled evidence from self-defined systematic reviews that assessed the factors that cause ED crowding, appraised the measures of ED crowding, and analyzed the outcomes and harms related to crowding. Methodology was supported by the current PRIOR statement [15] for overview of reviews.
Eligibility
Articles were considered to be within scope of the study if they were: self-defined systematic reviews; if the reviews included an analysis of input, throughput, or output in the emergency department; had quantitative data available on the metrics of overcrowding; included data on the harms of overcrowding; analyzed the causes of overcrowding; or if the reviews were emergency department reviews. Studies were excluded based on being the wrong study type; if they investigated the interventions of crowding in the emergency department; if the studies were published earlier than 2010; if the reviews investigated specific conditions related to overcrowding; or were related to inpatient units; or the reviews were specific to one country.
Search
A health sciences librarian with experience in systematic reviews (HG) searched MEDLINE and Embase on the Ovid platform, from inception to October 5, 2022, for subject headings and keywords related to the concepts of emergency department and overcrowding. A search filter for systematic reviews, originally developed by the Canadian Agency for Drugs and Technologies in Health [16] was slightly modified to include scoping reviews and applied to the base search. Complete search strategies can be found in Appendix 1.
Data extraction and quality appraisal
During the extraction process, four reviewers sorted the reviews by population and intervention comparisons and extracted the primary studies that were used in the systematic review. The authors, populations, and outcomes were assessed by the reviewers. In the case of overlap, authors were to choose the newest article and the one of highest quality. However, given the broad search criteria and the global nature of this review, none of the reviews were excluded and moved forward to analysis. Reviewers independently extracted data from each systematic review, using a data table which was piloted by all reviewers. The primary author then confirmed the extraction data, and conflicts were resolved vis consensus with the whole team.
Data were extracted and tabulated for the following details: review title and author, the year of publication, the journal of publication, the databases which were searched for the study, the period surveyed by the study, the number of primary studies included, the types of primary studies which were included, the comparison groups in the study (if relevant), and the key findings from the authors. Furthermore, we extracted project specific metrics which included: the problems contributing to ED crowding, the metrics of crowding, and the harms of crowding.
Two reviewers independently assessed the risk of bias of the included systematic reviews using the systematic review specific JBI checklist tool [17]. The JBI tool evaluates possible biases in the reviews as well as evaluating the process used to establish the reviews. The JBI scores for each paper are included in Table 1. Two reviewers independently assessed the quality of each included article, with disagreements settled by a third reviewer. Scores ranged from low quality to high quality, with most of the studies being of moderate quality. These ratings can be accounted for due to the study design associated with systematic review. However, when summarizing the results into the narrative synthesis, the results of moderate to high quality articles were considered more strongly. Risk of bias from the primary studies was collected using the JBI tool in each of the systematic reviews.
Data synthesis
We synthesized the data into a narrative review, which is supported by the tables of statistical outcomes reported in the original systematic reviews. Given the heterogeneity across studies in the various outcomes, no additional statistical analyses were conducted. We reported the results of the systematic search in a narrative fashion governed by the PRIOR statement and the Preferred Reporting Items for Systematic Reviews (PRISMA) statement of reviews [15, 18].
Results
Results of the search process
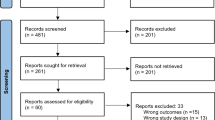
Two hundred and fifty-eight articles were retrieved from the seven identified databases. These articles were screened at the title and abstract stage, then 78 were screened in the full-text review. Thirteen full-text articles were included in the final review. These systematic reviews contained one hundred and eighty-seven individual primary studies, of which the majority consisted of observational studies, followed closely by randomized control trials. The PRISMA and Meta-Analyses flowchart of the study selection is depicted in Fig. 1.

PRISMA flow diagram
Description of included systematic reviews
Thirteen systematic reviews, each targeting aspects related to the causes, harms, and measures of emergency department crowding, were retained for this project. Several studies covered more than one category. The studies were grouped according to these categories: (a) Four reviews evaluated the validity of measures used to study emergency department crowding; (b) Four studies investigated the causes of emergency department overcrowding; and (c) Nine studies evaluated the possible outcomes and harms of crowding in emergency departments. Table 1 presents the main findings of each systematic review, as well as the evaluation of their characteristics and release date. The specific metrics of crowding that were evaluated by the systematic reviews are included in Table 2.
The primary studies consisted predominantly of observational studies. The studies were assessed by authors for overlap of the primary research used in the systematic reviews and determined that the study goals between the systematic reviews and the papers used were sufficiently unique to utilize the results of each systematic review independently.
Review findings
Metrics used to assess ED crowding
Measures of crowding in the emergency department serve multiple purposes. They provide a means with which to base research findings, as well as a quantitative measure that can be used to evaluate crowding interventions. Several metrics were noted to be used repeatedly in the systematic reviews and were appraised by authors for their effectiveness as well as the frequency of use in quality assurance and intervention research. A summary of the metrics that were evaluated by the relevant systematic reviews are included in Table 2. These could be classified broadly based on two headings: patient flow measures and metrics of patient occupancy [19]. Patient flow measures rely predominantly on time, whereas nonflow measures evaluate the number of people and utilization of resources [19]. Measures can be further subdivided into their aspect of emergency care: input, throughput, and output [14, 19,20,21]. A commonly assessed metric, which falls under the nonflow input category, is the number of waiting room patients and waiting room wait times, including time to triage and time to a bed in the emergency department [14, 21]. These metrics were found to be reliable across multiple studies, and reinforced by physician feedback, as a good evaluation of crowding and boarding in the emergency department [20]. Furthermore, the number of patients in the waiting room was linked to quality of care provided in the ED [22, 23]. A summary of the commonly investigated and relevant patient flow and occupancy metrics are contained in Table 3. From these, it was noted that the most prevalent measures included flow and metrics of occupancy, number of patients in the waiting room and the department, and the number of boarders.
Length of stay in the emergency department, a flow metric reflective of throughput care, was also commonly used and highly predictive of the degree of crowding in emergency departments [14, 21, 23]. This was accompanied by various measures of ED occupancy, including at individual time points and over an established period [14]. These time-based metrics are also used to understand the treatment load in the emergency department. To better understand patient experience and the efficiency of emergency departments, time to diagnostic testing from entry to the ED can be used [14]. These throughput measures have been associated with patient safety and employee satisfaction and performance [14, 23].
Boarding, a core output metric, is most frequently measured using comparisons between throughput measures and more specific metrics. One specific measure of emergency department output and access block is the number of admitted patients awaiting inpatient beds, number of boarders in the department, percentage of beds occupied by boarders within the department, or time from admitting to movement out of the ED [20, 22]. This has been compared to the ED output measure of “number of patients ready for discharge” to evaluate conditions in the emergency department at a given time [14, 20, 21, 23]. Finally, the culmination of these factors, or the individual factors themselves can be correlated with ED mortality rates, which are commonly used to measure quality of care in the ED [23].
The combination of the input, throughput, and output measures can be used to generate objective scores which have consistently been found to be a better predictive of crowding in the emergency department [14, 19]. The noted measures have been mentioned across several primary studies, however, more research should be performed regarding the generalizability of measures and their performance across multiple emergency department settings [19, 21]. Two composite mathematical indices assessing crowding severity include the National Emergency Department Overcrowding (NEDOC) score and the Emergency Department Work Index (EDWIN) score [8, 14, 19]. Both metrics have demonstrated a strong association with clinician opinions of crowding, patients leaving without being seen, and ambulance diversion [19]. Moreover, both have proven studied impacts based on quantitative capacity and usage metrics and correlate with perception of care and objective crowding [24]. Nonetheless, in their current state these measures are effective tools to investigate crowding in global EDs and to investigate causes and possible interventions.
Causes of overcrowding
The causes of overcrowding, like measures of overcrowding, can be grouped to better understand the intricacies of each issue and to stratify possible solutions. Causes of crowding are broken down broadly into patient, service delivery, and healthcare system-related factors, which can be grouped further into how they impact input, throughput, and output service in emergency departments [25, 26].
Patient presentations can impact resource utilization, therein impacting time spent and possible crowding in global emergency departments [8]. Factors that may increase time spent in the ED include being critically ill, extremes of age, male gender, and social determinants of health [25]. Thus, the ageing of the population, particularly in North America, and increasing patient reported loneliness have been cited as factors that contribute to increased patient presentations and longer length of stay in the ED [25, 26]. The speed of service delivery to these patients is impacted by ED staff-related factors, which may further exacerbate crowding issues [27].
Emergency service delivery via healthcare staff and flow in the emergency department impacts crowding through input, throughput, and output metrics [25]. Service delivery factors include a delay to discharge or imaging and lab investigations, increased time to inpatient consultation, staff fatigue, and crowding itself, which causes delays to diagnostic tools and final diagnoses [8, 25,26,27]. Inadequate staffing of nurses, high rates of provider burnout, excessive workloads, and high staff turnover is strongly associated with throughput causes and may further aggravate crowding issues [27]. While these are staff-related factors, they can be exacerbated by system-related factors, wherein healthcare system environments can significantly worsen conditions for staff [8].
Crowding in EDs globally presents a system-wide healthcare related issue, and is worsened by lack of access to both primary care and tertiary care [25]. Globally, crowding has also been linked to a lack of access to non-urgent primary care centers, leading to increased low acuity presentations in emergency departments [8, 25, 26, 28]. Departments have also noted an increase in mental health and addictions presentation due to limited access to resources and primary care physicians [26]. Furthermore, boarding of admitted patients in the ED, the most commonly cited cause of crowding, is shown to be caused by a shortage of inpatient beds, which is a result of challenges in hospital wards manifesting as high occupancy levels [25]. It is important to acknowledge that crowding is a global healthcare challenge, but should be informed by local considerations in order to tailor interventions to identified causes [8].
Health and system impacts
The importance of investigating ED crowding is emphasized when understanding the impacts to patients, healthcare staff, and the healthcare system at large. [8, 11, 14, 22,23,24,25, 27, 28]. These outcomes are the basis of many measures that are used for crowding research in the ED and highlight the importance of this research. Patient harms of crowding, at its worst, include an increased risk for morbidity, adverse events, and mortality [6, 25, 28]. Lesser effects of crowding include delayed time to assessment, decreased quality of care, or medication errors which may cumulate in low patient satisfaction [11]. Crowding can also cause increased walkouts prior to receiving care, which may contribute to an increased chance of readmission and prolonged time in the hospital [14, 24, 25]. These patient factors are further exacerbated by the impacts that crowding has on the healthcare system.
Crowding’s influence on the system impacts quality of care and the health of providers and patients. Crowding results in an increased workload, which decreases performance and efficiency, and increases the amount of time that patients spend in the ED [8, 14, 28]. Furthermore, as was observed during the COVID-19 pandemic, a high rate of bed occupancy can result in poor infection prevention and the spread of respiratory infections [28]. All these factors, including poor compliance to quality of care and worse understanding of patient conditions can increase the cost of care and treatment in the ED [11, 13, 28].
Crowding is a major patient safety concern and has a large impact on the healthcare system and healthcare providers’ wellbeing. Understanding the magnitude of these effects should motivate the development of interventions to better control ED crowding in emergency departments globally.
Discussion
Emergency department crowding presents a global healthcare concern, with many inciting factors and consequential outcomes. The results of this overview of reviews group the main problems of overcrowding into the measures, causes, and consequences of overcrowding. Current literature, while heterogeneous, presents common themes with regards to the measurements, causes, and outcomes of crowding in global emergency departments. The measures that are used in crowding literature can be stratified based on their aspect of emergency care: input, throughput, and output. These were further divided into flow and non-flow metrics, wherein one review states that flow metrics are growing in use and popularity [20]. This is in alignment with recent works, which suggests that current literature is difficult to apply clinically due to heterogeny between measurements and a lack of a standard definition in many metrics, even when in the same geographical region [29, 30]. Additionally, it was in accordance with current literature that suggests that time-based targets may be most effective in evaluating the impacts of crowding and measuring interventions, which may warrant further research on these flow metrics [31, 32]
The major causes of ED crowding were broken down into patient-based, staff-based, and system-based factors. The most prevalent issue appears to be system based, resulting in access block, and exacerbating patient-related and staff-related factors. These results are consistent with current literature, which suggests that patient-based factors may put a strain on hospital resources and can be alleviated by systems-based solutions [33]. This is also consistent with research which identifies staffing shortages as both a cause and an outcome of crowding in EDs, though lack of standardization of staffing requirements limits research into its role as a cause [6, 8, 27]. Current literature, in line with the results reported in this literature, reports that ED crowding can be predicted by measuring boarding rates in the emergency department [34, 35]. Thus, it is important to target healthcare-level solutions to reduce the negative impacts of emergency department crowding [5].
The importance of managing crowding on an international scale cannot be understated as there are several various negative outcomes that have emerged due to crowding. These outcomes predominantly impact patients in terms of treatment quality and resulting management shortcomings. However, crowding has impacts on staff burnout and satisfaction, and has a proven financial impact on the healthcare system. The most commonly cited factor, and the most important in terms of patient care, is that ED crowding increases the chances of adverse events and mortality for patients [7]. In some cases, this association is profound; one study showed that for every 5 h spent in the ED, chance of mortality increased by over 50% [36]. Chances of poor outcomes are increased, because crowding is associated with poorer service delivery, patients leaving without being seen, and staff burnout [3, 24, 33, 37].
Future investigations should focus on the interventions which have found to be most effective with regards to the heterogeneous causes of crowding [14]. A current difficulty with current interventions is that they do not appear to be matching the issues that have been presented in the crowding literature [14, 38]. Thus, it is important to consider the specific community and national circumstances that are facing departments when proposing solutions. Furthermore, these results can be used to help inform the international conversation on the global harms, causes, and measures of crowding in emergency departments. This is the first overview of reviews to comprehensively synthesize the global literature on crowding in this context.
Limitations
A wide range of primary studies were utilized to produce the systematic reviews that were analyzed for this research. While this reflects the differences in global literature effectively, it results in differences in measurements and criteria within studies, making it difficult to standardize the results. To minimize this, we synthesized the results into a narrative review to descriptively summarize the outcomes of interest.
Another important factor that was considered is that the primary studies used to make the reviews were predominantly conducted in developed countries. Thus, the presented results may not reflect the current causes and outcomes of crowding in developing countries, which structure healthcare in a different way. The presented issues, therefore, may not manifest in the same way and may not be effectively studied using the same measurements in developed countries.
Conclusion
This overview outlined the results of 13 systematic reviews, which analyzed the current state of the literature in global emergency department overcrowding. The current state of ED crowding research employs a varied set of measurements that analyze all aspects of emergency care, including input, throughput, and output. While these accurately reflect crowding measures, there is a need to develop a standard validated set of measures that may be used to better understand crowding across jurisdictions, and thus on a global scale. Similarly, there are several factors which cause and contribute to crowding in global emergency departments. The foremost of these, reflected in every systematic review that analyzed causes, is inpatient boarding which causes access blocks and diverts bed usage from new incoming ED patients to those awaiting inpatient beds. Worldwide, ED crowding is having a negative impact on the mission of emergency care through worsening patient outcomes, ED staff and infrastructure, and healthcare spending. While the causes and solutions to ED crowding will be unique and require tailoring to local circumstances, the 13 systematic reviews highlighted here serve as a foundation for concerted evidence-informed efforts.
References
Affleck A et al (2013) Emergency department overcrowding and access block. Can J Emerg Med 15(6):359–370
Javidan AP et al (2021) The international federation for emergency medicine report on emergency department crowding and access block: a brief summary. Emerg Med J 38(3):245–246
Bernstein SL et al (2009) The effect of emergency department crowding on clinically oriented outcomes. Acad Emerg Med 16(1):1–10
Asplin BR et al (2003) A conceptual model of emergency department crowding. Ann Emerg Med 42(2):173–180
Ansah JP et al (2021) Modeling emergency department crowding: restoring the balance between demand for and supply of emergency medicine. PLoS ONE 16(1):e0244097–e0244097
McKenna P et al (2019) Emergency department and hospital crowding: causes, consequences, and cures. Clin Exp Emerg Med 6(3):189–195
Jones S et al (2022) Association between delays to patient admission from the emergency department and all-cause 30-day mortality. Emerg Med J 39(3):168
Morley C et al (2018) Emergency department crowding: a systematic review of causes, consequences and solutions. PLoS ONE 13(8):e0203316
Lee JH et al (2022) Effect of a boarding restriction protocol on emergency department crowding. Yonsei Med J 63(5):470–479
Savioli G et al (2021) Impact of coronavirus disease 2019 pandemic on crowding: a call to action for effective solutions to “access block.” West J Emerg Med 22(4):860–870
do Nascimento Rocha, H.M., A.G.M. da Costa Farre, and V.J. de Santana Filho, (2021) Adverse events in emergency department boarding: a systematic review. J Nurs Scholarsh 53(4):458–467
Hoot NR et al (2020) Does crowding influence emergency department treatment time and disposition? J Am College Emerg Physic Open 2(1):e12324–e12324
Doan Q et al (2019) The impact of pediatric emergency department crowding on patient and health care system outcomes: a multicentre cohort study. CMAJ 191(23):E627–E635
Badr S et al (2022) Measures of Emergency Department Crowding, a Systematic Review. How to Make Sense of a Long List. Open Access Emerg Med. 14:5–14
Gates M et al (2022) Reporting guideline for overviews of reviews of healthcare interventions: development of the PRIOR statement. BMJ 378:e070849
Hubbard W et al (2022) Development and validation of paired MEDLINE and Embase search filters for cost-utility studies. BMC Med Res Methodol 22(1):310
Peters MD (2015) Not just a phase: JBI systematic review protocols. JBI Database Syst Rev Implement Rep 13(2):1–2
Page MJ et al (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372:n71
Hwang U et al (2011) Measures of crowding in the emergency department: a systematic review. Acad Emerg Med 18(5):527–538
Stang AS et al (2015) Crowding measures associated with the quality of emergency department care: a systematic review. Acad Emerg Med 22(6):643–656
Abudan A, Merchant RC (2021) Multi-dimensional measurements of crowding for pediatric emergency departments: a systematic review. Glob Pediatr Health. 8:2333794x21999153
Jones PG, Mountain D, Forero R (2021) Emergency department crowding measures associations with quality of care: a systematic review. Emerg Med Australas 33(4):592–600
Di Laura D et al (2021) Efficiency measures of emergency departments: an Italian systematic literature review. BMJ Open Qual 10(3):e001058
Carter EJ, Pouch SM, Larson EL (2014) The relationship between emergency department crowding and patient outcomes: a systematic review. J Nurs Scholarsh 46(2):106–115
Rasouli HR, Aliakbar Esfahani A, Abbasi Farajzadeh M (2019) Challenges, consequences, and lessons for way–outs to emergencies at hospitals: a systematic review study. BMC Emerg Med 19(1):62
Lowthian JA et al (2011) Systematic review of trends in emergency department attendances: an Australian perspective. Emerg Med J 28(5):373–377
McDermid F, Judy M, Peters K (2020) Factors contributing to high turnover rates of emergency nurses: a review of the literature. Aust Crit Care 33(4):390–396
Rasouli HR et al (2019) Outcomes of crowding in emergency departments; a systematic review. Arch Acad Emerg Med 7(1):e52
Morris ZS et al (2012) Emergency department crowding: towards an agenda for evidence-based intervention. Emerg Med J 29(6):460–466
Rowe BH, McRae A, Rosychuk RJ (2020) Temporal trends in emergency department volumes and crowding metrics in a western Canadian province: a population-based, administrative data study. BMC Health Serv Res 20(1):356
Andersson J et al (2020) Long emergency department length of stay: a concept analysis. Int Emerg Nurs 53:100930
McRae AD et al (2022) A comparative evaluation of the strengths of association between different emergency department crowding metrics and repeat visits within 72 hours. CJEM 24(1):27–34
Eriksson CO et al (2017) The Association between hospital capacity strain and inpatient outcomes in highly developed countries: a systematic review. J Gen Intern Med 32(6):686–696
Smith AJ et al (2022) Multisite evaluation of prediction models for emergency department crowding before and during the COVID-19 pandemic. J Am Med Inform Assoc. https://doi.org/10.1093/jamia/ocac214
Kenny JF, Chang BC, Hemmert KC (2020) Factors affecting emergency department crowding. Emerg Med Clin North Am 38(3):573–587
Plunkett PK et al (2011) Increasing wait times predict increasing mortality for emergency medical admissions. Eur J Emerg Med 18(4):192–196
Gorski JK et al (2021) Crowding is the strongest predictor of left without being seen risk in a pediatric emergency department. Am J Emerg Med 48:73–78
Valipoor S et al (2021) Data-driven design strategies to address crowding and boarding in an emergency department: a discrete-event simulation study. HERD 14(2):161–177
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Pearce, S., Marchand, T., Shannon, T. et al. Emergency department crowding: an overview of reviews describing measures causes, and harms. Intern Emerg Med 18, 1137–1158 (2023). https://doi.org/10.1007/s11739-023-03239-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11739-023-03239-2