
Abstract
Purpose
Roux-en-Y gastric bypass (RYGB) and sleeve gastrectomy (SG) are the two most popular procedures performed. The decision of which technique is most appropriate depends on the surgeon’s preferences and experience. However, several factors strongly influence the decision of the procedure performed, including gastrointestinal disorders or asymptomatic upper gastrointestinal endoscopy (UGE) findings.
This study aimed to describe the pathological endoscopic findings in morbidly obese patients undergoing preoperative routine UGE.
Materials and Methods
A retrospective review of a prospectively collected database of all UGEs performed before bariatric surgery was performed. UGE was routinely performed to all the patients as part of the preoperative evaluation protocol.
Results
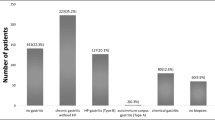
A total of 790 patients were included. Surgical technique included 610 (77.2%) RYGB and 180 (22.8%) SG. Twenty-one asymptomatic patients presented esophagitis at UGE. In only seven patients (0.89%), the endoscopic findings of esophagitis had changed the initial surgical decision. The presence of ulcers or adenomatous or incompletely resected polyps was an indication for SG, to assure future endoscopic access in case it is needed. In 25 patients (3.17%), the initial operation would have been changed based on UGE findings.
Conclusion
Preoperative UGE allows the diagnosis of asymptomatic esophagitis related to gastroesophageal reflux disease and the identification of asymptomatic polyps and ulcers, with the potential ability for malignant transformation. In up to 3.17% of the cases, the endoscopic findings changed the operative strategy. As the complication rate associated with the procedure is low, we recommend the routine performance of preoperative UGE before bariatric surgery.
Similar content being viewed by others


References
Obesity and overweight facts sheet. World Health Organization Website. https://www.who.int/news-room/fact-sheets/detail/ obesity-and-overweight. Updated. Accessed March 2, 2020. February 16, 2018:3.
Diabetes facts sheet. World Health Organization Website. https://www.who.int/news-room/fact-sheets/detail/diabetes. Updated October 30, 2018. Accessed March 2, 2020.
Wolter S, Duprée A, Miro J, et al. Upper gastrointestinal endoscopy prior to bariatric surgery-mandatory or expendable? An analysis of 801 cases. Obes Surg. 2017;27(8):1938–43.
Sjostrom L. Review of the key results from the Swedish Obese Subjects (SOS) trial—a prospective controlled intervention study of bariatric surgery. J Intern Med. 2013;273(3):219–34.
Jans A, Näslund I, Ottosson J, et al. Duration of type 2 diabetes and remission rates after bariatric surgery in Sweden 2007–2015: a registry-based cohort study. PLoS Med. 2019;16(11):e1002985.
Zhao H, Jiao L. Comparative analysis for the effect of Roux-en-Y gastric bypass vs sleeve gastrectomy in patients with morbid obesity: evidence from 11 randomized clinical trials (meta-analysis). Int J Surg. 2019;72:216–23.
Gastrointestinal surgery for severe obesity: National Institutes of Health Consensus Development Conference Statement. Am J Clin Nutr. 1992;55(2 Suppl):615S–619S.
Canil AM, Iossa A, Termine P, et al. Histopathology findings in patients undergoing laparoscopic sleeve Gastrectomy. Obes Surg. 2018;28(6):1760–5.
Wang Y, Song Y, Chen J, et al. Roux-en-Y gastric bypass versus sleeve gastrectomy for super super obese and super obese: systematic review and meta-analysis of weight results, comorbidity resolution. Obes Surg. 2019;29(6):1954–64.
Kang JH, Le QA. Effectiveness of bariatric surgical procedures. Medicine. 2017;96(46):e8632.
Brunt EM, Wong VW, Nobili V, et al. Nonalcoholic fatty liver disease. Nat Rev Dis Primers. 2015;1:15080.
Pories WJ. Bariatric surgery: risks and rewards. J Clin Endocrinol Metab. 2008;93(11 Suppl 1):S89–96.
Stefater MA, Wilson-Pérez HE, Chambers AP, et al. All bariatric surgeries are not created equal: insights from mechanistic comparisons. Endocr Rev. 2012;33(4):595–622.
Wolfe BM, Kvach E, Eckel RH. Treatment of obesity: weight loss and bariatric surgery. Circ Res. 2016;118(11):1844–55.
Abou Hussein B, Khammas A, Shokr M, et al. Role of routine upper endoscopy before bariatric surgery in the Middle East population: a review of 1278 patients. Endoscopy International Open. 2018;06:E1171–6.
Öner Rİ, Özdaş S. Histopathological findings in morbid obese patients undergoing laparoscopic sleeve Gastrectomy: does H. pylori infection effective on pathological changes? Obes Surg. 2018;28(10):3136–41.
Bou Daher H, Sharara AI. Gastroesophageal reflux disease, obesity and laparoscopic sleeve gastrectomy: the burning questions. World J Gastroenterol. 2019;25(33):4805–13.
Sauerland S, Angrisani L, Belachew M, et al. Obesity surgery: evidence-based guidelines of the European Association for Endoscopic Surgery (EAES). Surg Endosc. 2005;19:200–21.
Dhariwal A, Plevris JN, Lo NT, et al. Age, anemia, and obesity associated oxygen desaturation during upper gastrointestinal endoscopy. Gastrointest Endosc. 1992;38:684–8.
Bennett S, Gostimir M, Shorr R, et al. The role of routine preoperative upper endoscopy in bariatric surgery: a systematic review and meta-analysis. Surg Obes Relat Dis. 2016;12:1116–25.
Parikh M, Liu J, Vieira D, et al. Preoperative endoscopy prior to bariatric surgery: systematic review and meta-analysis of the literature. Obes Surg. 2016;26:2961–6.
Kasyap AK, Sah SK, Chaudhary S. Clinical spectrum and risk factors associated with asymptomatic erosive esophagitis as determined by Los Angeles classification: a cross-sectional study. PLoS One. 2018;13:e0192739.
Manterola C, Munoz S, Grande L, et al. Initial validation of a questionnaire for detecting gastrooesophageal reflux disease in epidemiological settings. J Clin Epidemiol. 2002;55:1041–5.
Martın Garcıa-Almenta E, Ruiz-Tovar J, Sanchez SS. Vıa clınica en cirugıa bariatrica. Albacete: Im3diA comunicacion S.L.; 2017.
SAGES guideline for clinical application of laparoscopic bariatric surgery. Surg Obes Relat Dis. 2009;5:387–405.
Evans JA, Muthusamy VR, Acosta RD, et al. The role of endoscopy in the bariatric surgery patient. Gastrointest Endosc. 2015;29:1007–17.
Schreiner MA. Endoscopy in the obese patient. Gastroenterol Clin N Am. 2010;39:87–97.
SAGES Guidelines Committee. SAGES guideline for clinical application of laparoscopic bariatric surgery. Surg Endosc. 2008;22:2281–300.
Melissas J, Braghetto I, Molina JC, et al. Gastroesophageal reflux disease and sleeve gastrectomy. Obes Surg. 2015;25(12):2430–5.
Yeung KTD, Penney N, Ashrafian L, et al. Does sleeve gastrectomy expose the distal esophagus to severe reflux?: a systematic review and meta-analysis. Ann Surg. 2020;271:257–65.
Gagner M. Is sleeve gastrectomy always an absolute contraindication in patients with Barrett's? Obes Surg. 2016;16:715–7.
Pérez de la Serna y Bueno J, Ruiz de León San Juan A. pH-metry/impedance-24 hours pH-metry. Rev Esp Enferm Dig. 2015;107(4):243.)
Schwameis K, Lin B, Roman J, et al. Is pH testing necessary before antireflux surgery in patients with endoscopic erosive esophagitis? J Gastrointest Surg. 2018;22:8–12.
Saarinen T, Kettunen U, Pietiläinen KH, et al. Is preoperative gastroscopy necessary before sleeve gastrectomy and Roux-en-Y gastric bypass? Surg Obes Relat Dis. 2018;14:757–63.
Ghaderi I, Gondal AB, Samamé J, et al. Preoperative endoscopic and radiologic evaluation of bariatric patients: what do they add? J Gastrointest Surg. 2019; https://doi.org/10.1007/s11605-019-04219-8.
Peker KD, Sahbaz NA, Seyit H, et al. An alternative view on the necessity of EGD before sleeve gastrectomy. Surg Obes Relat Dis. 2017;13(12):1959–64.
Fernandes SR, Meireles LC, Carrilho-Ribeiro L, et al. The role of routine upper gastrointestinal endoscopy before bariatric surgery. Obes Surg. 2016;26:2105–10.
Rosai J. Stomach. In: Rosai J, editor. Ackerman’s surgical pathology. St Louis: Mosby; 1996. p. 616–66.
Kashiwagi H. Ulcers and gastritis. Endoscopy. 2003;35(1):9–14.
Genta RM, Schuler CM, Robiou CI, et al. No association between gastric fundic gland polyps and gastrointestinal neoplasia in a study of over 100,000 patients. Clin Gastroenterol Hepatol. 2009;7:849–54.
Carmack SW, Genta RM, Schuler CM, et al. The current spectrum of gastric polyps: a 1-year national study of over 120,000 patients. Am J Gastroenterol. 2009;104:1524–32.
Moulla Y, Lyros O, Mehdorn M, et al. Preoperative upper-GI endoscopy prior to bariatric surgery: essential or optional? Obes Surg. 2020; https://doi.org/10.1007/s11695-020-04485-5.
Schneider R, Lazaridis I, Kraljevic M, et al. The impact of preoperative investigations on the management of bariatric patients; results of a cohort of more than 1200 cases. Surg Obes Relat Dis. 2018;14:693–9.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Statement of Informed Consent
Informed consent was obtained from all individual participants included in the study.
Statement of Human Rights
All procedures performed in this study were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
García-Gómez-Heras, S., Garcia, A., Zubiaga, L. et al. Prevalence of Endoscopic Findings Before Bariatric Surgery and Their Influence on the Selection of the Surgical Technique. OBES SURG 30, 4375–4380 (2020). https://doi.org/10.1007/s11695-020-04800-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-020-04800-0