
Abstract
Background
Postoperative pain and analgesia present challenges in bariatric surgery patients. Multimodal analgesia may provide better efficacy, less complications and expedite fast-track bariatric surgical care. There are no studies of the broader topic of perioperative analgesia and the overall impact. This study highlights the impact of multimodal intraoperative analgesia on fast-track bariatric surgery.
Methods
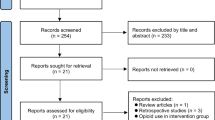
This observational study examined the perioperative outcome data of 412 consecutive laparoscopic bariatric surgery patients over a 6-year period. Perioperative outcome and variables were analysed and compared between different intraoperative analgesia types.
Results
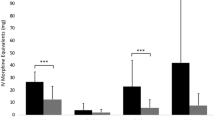
Mean BMI was 49, mean age was 42 and male:female ratio was 1:4. About 82% of patients received multimodal intraoperative analgesia, comprising various combinations of bupivacaine infiltration and intravenous acetaminophen, morphine, tramadol, parecoxib or diclofenac. Morphine was administered in 83% of patients and tramadol in 17%. Multimodal intraoperative analgesia provided better postoperative analgesia, shorter postanaesthesia care unit (PACU) duration, lower postoperative opioid requirement, less postoperative vomiting, earlier postoperative oral intake, earlier ambulation and shorter hospital stay compared to unimodal intraoperative morphine analgesia (p = 0.0001). Multimodal analgesia comprising tramadol + acetaminophen + diclofenac provided better postoperative analgesia, shorter PACU duration, lower postoperative opioid requirement, earlier ambulation, shorter hospital stay and less postoperative hypopnoea compared to patients who received morphine (p = 0.0001).
Conclusions
Multimodal intraoperative analgesia provides better postoperative analgesia, less complications and better perioperative outcomes and facilitates fast-track bariatric surgical care. Tramadol is suitable, efficacious and safe and associated with the best perioperative outcomes in bariatric surgery patients.
Similar content being viewed by others
References
Bamgbade OA, Adeogun BO, Abbas K. Fast-track laparoscopic gastric bypass surgery: outcomes and lessons from a bariatric surgery service in the United Kingdom. Obes Surg. 2012;22(3):398–402.
Dogan K, Kraaij L, Aarts EO, et al. Fast-track bariatric surgery improves perioperative care and logistics compared to conventional care. Obes Surg. 2015;25(1):28–35.
Bamgbade OA, Rutter TW, Nafiu OO, et al. Postoperative complications in obese and nonobese patients. World J Surg. 2007;31(3):556–60.
Lemanu DP, Srinivasa S, Singh PP, et al. Optimizing perioperative care in bariatric surgery patients. Obes Surg. 2012;22(6):979–90.
Bamgbade OA, Alfa JA. Dexmedetomidine anaesthesia for patients with obstructive sleep apnoea undergoing bariatric surgery. Eur J Anaesthesiol. 2009;26(2):176–7.
Lloret-Linares C, Lopes A, Declèves X, et al. Challenges in the optimisation of post-operative pain management with opioids in obese patients: a literature review. Obes Surg. 2013;23(9):1458–75.
Bamgbade OA, Chung AS, Khalaf WM, et al. Survey of perioperative care of adults with obstructive sleep apnoea. Eur J Anaesthesiol. 2009;26(8):706–8.
Weingarten TN, Sprung J, Flores A, et al. Opioid requirements after laparoscopic bariatric surgery. Obes Surg. 2011;21(9):1407–12.
Bamgbade OA. Advantages of doxapram for post-anaesthesia recovery and outcomes in bariatric surgery patients with obstructive sleep apnoea. Eur J Anaesthesiol. 2011;28(5):387–8.
Moncada R, Martinaitis L, Landecho M, et al. Does preincisional infiltration with bupivacaine reduce postoperative pain in laparoscopic bariatric surgery? Obes Surg. 2016;26(2):282–8.
Song K, Melroy MJ, Whipple OC. Optimizing multimodal analgesia with intravenous acetaminophen and opioids in postoperative bariatric patients. Pharmacotherapy. 2014;34(Suppl 1):14S–21S.
Ziemann-Gimmel P, Hensel P, Koppman J, et al. Multimodal analgesia reduces narcotic requirements and antiemetic rescue medication in laparoscopic Roux-en-Y gastric bypass surgery. Surg Obes Relat Dis. 2013;9(6):975–80.
Gonzalez AM, Romero RJ, Ojeda-Vaz MM, et al. Intravenous acetaminophen in bariatric surgery: effects on opioid requirements. J Surg Res. 2015;195(1):99–104.
Lam KK, Mui WL. Multimodal analgesia model to achieve low postoperative opioid requirement following bariatric surgery. Hong Kong Med J. 2016;22(5):428–34.
Ruiz-Tovar J, Muñoz JL, Gonzalez J, et al. Postoperative pain after laparoscopic sleeve gastrectomy: comparison of three analgesic schemes (isolated intravenous analgesia, epidural analgesia associated with intravenous analgesia and port-sites infiltration with bupivacaine associated with intravenous analgesia). Surg Endosc. 2017;31(1):231–6.
Schumann R. Anaesthesia for bariatric surgery. Best Pract Res Clin Anaesth. 2011;25(1):83–93.
Lehmann KA. Tramadol in acute pain. Drugs. 1997;53(Suppl 2):25–33.
Saurabh S, Smith JK, Pedersen M, et al. Scheduled intravenous acetaminophen reduces postoperative narcotic analgesic demand & requirement after laparoscopic Roux-en-Y gastric bypass. Surg Obes Relat Dis. 2015;11(2):424–30.
El-Shobary H, Christou N, Backman SB, et al. Effect of laparoscopic versus open gastric bypass surgery on postoperative pain and bowel function. Obes Surg. 2006;16(4):437–42.
Govindarajan R, Ghosh B, Sathyamoorthy MK, et al. Efficacy of ketorolac in lieu of narcotics in the operative management of laparoscopic surgery for morbid obesity. Surg Obes Relat Dis. 2005;1(6):530–5. discussion 535-536
Kamelgard JI, Kim KA, Atlas G. Combined preemptive and preventive analgesia in morbidly obese patients undergoing open gastric bypass: a pilot study. Surg Obes Relat Dis. 2005;1(1):12–6.
Acknowledgements
This study was approved and registered by the research department of Central Manchester University Hospital, Manchester, UK.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Institutional support is acknowledged, but there was no conflict of interest or financial involvement regarding any of the authors. The first author has no conflict of interest. The second author has no conflict of interest. The third author has no conflict of interest.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Statement of Human Rights
All procedures performed in this study were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Rights and permissions
About this article

Cite this article
Bamgbade, O.A., Oluwole, O. & Khaw, R.R. Perioperative Analgesia for Fast-Track Laparoscopic Bariatric Surgery. OBES SURG 27, 1828–1834 (2017). https://doi.org/10.1007/s11695-017-2562-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-017-2562-4