
Abstract
Epidemiological studies report high levels of anxiety and depression amongst adolescents. These psychiatric conditions and complex interplays of biological, social and environmental factors are important risk factors for suicidal behaviours and suicide, which show a peak in late adolescence and early adulthood. Although deaths by suicide have fallen globally in recent years, suicide deaths are increasing in some countries, such as the US. Suicide prevention is a challenging global public health problem. Currently, there aren’t any validated clinical biomarkers for suicidal diagnosis, and traditional methods exhibit limitations. Artificial intelligence (AI) is budding in many fields, including in the diagnosis of medical conditions. This review paper summarizes recent studies (past 8 years) that employed AI tools for the automated detection of depression and/or anxiety disorder and discusses the limitations and effects of some modalities. The studies assert that AI tools produce promising results and could overcome the limitations of traditional diagnostic methods. Although using AI tools for suicidal ideation exhibits limitations, these are outweighed by the advantages. Thus, this review article also proposes extracting a fusion of features such as facial images, speech signals, and visual and clinical history features from deep models for the automated detection of depression and/or anxiety disorder in individuals, for future work. This may pave the way for the identification of individuals with suicidal thoughts.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Suicide is a major health burden: the World Health Organisation (WHO) reports ~ 785,000 suicides annually, equivalent to one person dying every 40 s, with an incidence of 10.6 per 100,000 population (Naghavi 2019). Epidemiological studies show huge variations in suicides between different geographical areas: although suicides have fallen in China (all people) and India (young people), they are growing in many countries, including the USA, Brazil, and South Korea. The risk of suicide is complex to predict. It is understood to be influenced by the interaction of multiple factors. These include biological (for example, personality factors), clinical (psychiatric and physical health conditions), psychological and social, cultural, and environmental factors. For example, suicidal rates are correlated with economic recession, access to high lethality measures and media reporting of suicides.
The Centers for Disease Control and Prevention report that suicide is the third leading cause of death amongst teenagers and adolescents in the US (Health, United States 2004: with chartbook on trends in the health of Americans and updated tables 2005). Epidemiological studies further indicate that young adults between the ages of 15–21 represent the highest prevalence rates of mental illness at 39% (Eisenberg et al. 2007). Psychiatric conditions associated with suicidal ideation and behaviour include depression, anxiety, substance use disorders, and eating disorders (Brådvik 2018). Some indications of suicidal ideation include an earlier suicide attempt or intentional self-harm behaviour, just as cutting or burning oneself (Korczak et al. 2015). A recent review article reported that language barriers and separation from family were risk factors of suicide, as these factors can lead to a feeling of hopelessness, depression, and anxiety. Other risk factors for suicidality amongst adolescents are poor communication between adolescents and their parents, parental mental health conditions, and intra-family disputes (Korczak et al. 2015). A study by Izadinia et al. (2010) reported that while anxiety, depression, mental health, and everyday stresses were all correlated with suicidal ideations, depression, followed by anxiety, were the main contributors to suicidal ideation (Izadinia et al. 2010). Furthermore, Yeh et al. (2019) established that half of the people who died by suicide had at least one diagnosed mental health condition before the death. Therefore, screening for suicidal risks is a critical step in reducing suicides. This review article focuses on diagnosing depression and anxiety mental health disorders as part of screening for suicidal behaviours and suicide. “Introduction” section describes the background of suicidal ideation and its main contributors. “Traditional screening tools for suicide” section discusses the traditional screening methods used in clinical practice and their limitations. “Biological markers for suicide” section discusses biological markers. “Machine learning tools for diagnosis” section describes the possibility of employing machine learning methods to detect depression and/or anxiety disorder for suicidal ideation identification. In “Methodology for the study” section, the methodology of this review study is explained. In “Summarised studies” section, the summarised studies are described. In “Discussion” section, the findings of the review study are discussed. In “Future avenues for research” section, future avenues for research are proposed, and in “Conclusion” section, the study is concluded.
Traditional screening tools for suicide
Providing support to people who disclose their suicidal ideation is critical in suicide prevention. However, some individuals choose not to seek help for their suicidal ideation, which significantly impedes suicide prevention efforts (Brådvik 2018). For example, although suicidal ideation is generally higher in females (Nock et al. 2008), deaths by suicide are higher in males due to both choices of more lethal methods and reluctance to seek help (World Health Organization 2014). Studies have also shown that many individuals generally prefer consulting their primary care practitioners for emotional concerns than suicidal ideation, specifically due to the stigma associated with suicide (Calear and Batterham 2019). There are various screening tools such as the Columbia Suicide Screen, Risk of Suicide Questionnaire, Suicidal Ideation Questionnaire, Suicidal Ideation Questionnaire JR, Diagnostic Predictive Scales, Suicide Risk Screen and the Suicide Probability Scale (Joe and Bryant 2007) that are widely used by non-mental health professionals for suicide assessment. Additionally, screening programs are largely used in schools to assess suicide risks. For instance, in the first stage of the Teen Screen program, which is described as a model for early suicide prevention intervention, students are tasked to complete the Teen Screen screening questionnaire, after which those identified to be at a higher risk are further assessed through the use of the Diagnostic Interview Schedule for children. In the final stage, a clinician interviews the identified at-risk students (Calear and Batterham 2019). Hence, conventional diagnosis of suicide includes self-reports and clinical interviews.
Limitations of traditional screening methods
However, the afore-mentioned screening tools exhibit some limitations. Studies have shown that a lack of resources due to scarce funding for the assessment programs hinder the implementation of such programs in schools. Furthermore, as educators and school councilors are overwhelmed with the demands of each school day, they are reluctant to implement such risk assessment programs in schools (Mazza 1997). Additionally, several studies that were conducted on the effectiveness of school-based screenings reported a high incidence of false positives (Thompson and Eggert 1999). Also, since most of the suicide screening tools were developed using individuals who were identified as being of white ethnicity (Manetta and Ormand 2005), the tools may not be effective in identifying at-risk adolescents of different ethnicities.
Biological markers for suicide
There are no proven accurate biological markers of suicide that can be integrated into clinical practice. Some demographic and behavioural markers exist (Heeringen and Mann 2014). Forecasting and averting suicidal behaviour is still a budding research field, and several markers have been identified for future study (Nugent et al. 2019). For instance, Niculesu et al. (2017) reported that Apolipoprotein E and interleukin-6 were promising biomarkers for suicidal prediction. Kaminsky et al. (2015) reported epigenetic and genetic markers, including SKA2, as potential markers for suicidality, but further study replication was recommended. Many studies recognized changed sleep architecture to be a biomarker of suicidal thoughts and behaviour (Malik et al. 2014; Bernert et al. 2017; Ballard et al. 2016). The lack of an animal model for suicide (Gould et al. 2017) is a major constraint on basic scientific research, although developing such models is underway. An inadequate number of post-mortem brains available for research poses another challenge (Costanza et al. 2014).
Machine learning tools for diagnosis
The need for AI tools for the diagnosis of suicide risk
The limitations of clinical screening methods for suicide and the frequency of non-disclosure of suicidal ideation mean that 60–70% of individuals who commit suicide are not known to be at risk by their primary care practitioners (Ahmedani et al. 2014). Pourmand et al. (2018) reported in a recent review that adolescents often divulge risk factors for suicide on social media like Facebook and Twitter, even though they don’t disclose them to doctors. Of all the mental health-related tweets shared by large media outlets, around 30% had reference to suicide (Calear and Batterham 2019). Hence researchers have explored information from social media which overtly mentions suicidal thoughts or attempts. In another recent review by Franco et al. (2018), about 3.23% of studies exploring such data were related to machine learning algorithms, highlighting the potential of cutting-edge technological tools to predict suicide risk (Calear and Batterham 2019).
Traditional machine learning models
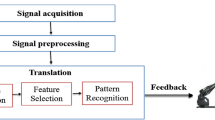
Machine learning is a sub-field of artificial intelligence (AI). Training of the machine learning model involves a sequence of steps; the input data is usually pre-processed to remove any noise, after which significant features are extracted and selected before the classification process. This workflow is presented in Fig. 1. In conventional machine learning, the system learns from its experience, wherein the system learns the pattern of the input data and responds from its learning, at the output (Voulodimos et al. 2018). At this juncture, the system becomes smarter as it learns the data automatically, without any human intervention (Voulodimos et al. 2018). However, machine learning works well with small data, but the extraction and selection of significant features are manual processes that require human intervention. Some examples of machine learning models commonly used for the classification of diseases include the support vector machine (Cristianini and Shawe-Taylor 2000), decision tree (Kingsford and Salzberg 2008), probabilistic neural networks (Specht 1990), k-nearest neighbour (Hu et al. 2016), and artificial neural networks (Grossi and Buscema 2007). Such conventional machine learning models have been fervently used in the classification of some mental illnesses such as schizophrenia (Sharma and Acharya 2021; Jahmunah et al. 2019), depression (Sharma et al. 2018a), Parkinson’s disease (Tuncer et al. 2020), and Alzheimer’s disease (Wei et al. 2020).

Workflow required for training a machine learning model
Advanced deep learning models
On the contrary, in more advanced machine learning, deep learning models with several layers between the input and output layers are used for classification purposes (Sharma et al. 2021a). Unlike conventional models, these models learn large input data before predicting a classification outcome. Furthermore, in contrast to traditional classifiers in deep models, the feature extraction and selection processes are automatically done by the model, without requiring human aid. Some examples of deep models commonly used for the classification of diseases include the convolutional neural network (CNN) (Sharma et al. 2018b), long short-term memory (LSTM) (Houdt et al. 2020), and autoencoders (Lopez Pinaya et al. 2019).
A CNN model comprises three main layers; convolution, pooling, and fully connected layers. The convolution and pooling layers aid in creating new feature maps in each succeeding layer, enabling the extraction of more complex features from the input data deeper into the network. The fully connected layers provide the output of the classification (Sharma et al. 2018b). Autoencoders comprise two main components known as the encoder, in which the model reduces the feature size and presents the input data into an encoded representation, and the decoder, wherein the model re-creates the data from the encoded version, such that it represents the original data very closely (Lopez Pinaya et al. 2019). The LSTM mainly comprises the input, forget, and output gates that control the information stored, read, and written on the cell, respectively, with the onset of input data. The model works by recollecting crucial information from previous states and building on them (Houdt et al. 2020). These models have been successfully employed in the automated detection of mental health conditions such as Parkinson’s disease (Oh et al. 2018), depression (Ay et al. 2019), and schizophrenia (Oh et al. 2020). Hence, machine learning techniques have also been employed efficaciously to detect mental health disorders. Figures 2a–c illustrate the architectures of the CNN, autoencoder, and LSTM deep models, respectively. The figures depict the workings of the models when the input data is fed to them.

Architectures of the CNN (a), autoencoder (b), and LSTM (c) models
Methodology for the study
This review study was conducted based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines to select the most relevant studies on AI tools developed for depression and/or anxiety diagnosis. To analyze more recent articles, the search was conducted between the years 2013 and 2022. The appropriate journal articles were searched through the Institute of Electrical and Electronics Engineers (IEEE), Google Scholar, PubMed, Science Direct, and Springer Link scientific repositories. The Boolean search strings such as “Machine Learning”, “Deep Learning”, “Artificial intelligence tools”, “Depression”, “Anxiety disorders” and “Suicidal ideation” were used in various combinations as perceived in Table 1. Three key processes were involved in the retrieval of articles based on the PRISMA guidelines. Initially, a total of 48,407 articles were identified based on the Boolean search strings for depression and anxiety disorder detection, wherein, for depression detection, 119,17 801, 8, 4771, and 3963 articles were retrieved from the IEEE, Google Scholar, PubMed, Science Direct and Springer link repositories respectively. For anxiety disorder detection, 16, 17,400, 3, 2211, and 2116 articles were retrieved from the aforementioned repositories. Then, articles were screened to eradicate duplicate and irrelevant articles, based on the inclusion and exclusion criteria, wherein articles on ‘mental health’, ‘stress’, ‘treatment’ or ‘treatment response’, ‘monitoring’, and ‘management’ were all excluded. Furthermore, theses, books, and abstracts were also omitted. The final number of articles relevant to this review were selected and set to 76, as seen in Tables 2, 3, 4 and 5. Figure 3 details how the PRISMA guideline was used to select the most relevant articles in this review.

Selection of relevant articles based on PRISMA guidelines
The search was conducted between May to June 2021. Studies were included if they met the following criteria:
-
(i)
They described the use of AI tools to diagnose depression and/or anxiety
-
(ii)
They were published between the years 2013 and 2022,
-
(iii)
They were published in a peer-reviewed journal,
-
(iv)
They were published in English.
Studies were excluded if:
-
(i)
They described the use of AI tools to diagnose depression and/or anxiety together with other conditions or disorders
-
(ii)
The article was not published in English
-
(iii)
The article was not published in a peer-reviewed journal
-
(iv)
The article was published before 2013
Summarised studies
Tables 2, 3, 4 and 5 summarize studies for detecting depression, anxiety disorder, suicidal ideation, and depression and anxiety disorder using AI tools, respectively. Comparing the tables, it can be deduced that most of the studies focus on detecting depression followed by depression and anxiety disorder as comorbid conditions. From the tables, it is also notable that most authors have successfully investigated audio and/or facial features for the detection of depression and/or anxiety disorder (Ooi et al. 2013; Zhou et al. 2015; Williamson et al. 2016; Pampouchidou et al. 2015; Pampouchidou et al. 2020; Yang et al. 2016, 2017; Dham et al. 2017; Alhanai et al. 2018; He and Cao 2018; Afshan et al. 2018; Zhu et al. 2018; Venkataraman 2018; Gavrilescu and Vizireanu Aug. 2019; Melo et al. 2019; Victor et al. 2019; Chlasta et al. 2019; Guntuku et al. 2019; Detecting Depression Using a Framework Combining Deep Multimodal Neural Networks with a Purpose-Built Automated Evaluation xxxx; Vázquez-Romero and Gallardo-Antolín 2020; Quatieri et al. 2020; Shinde et al. 2020; Zhang et al. Jul. 2020; Espinola et al. 2021; Matteo et al. 2021; Guo et al. 2021; Albuquerque et al. 2021). Additionally, some authors have widely analysed the brain signals (Sharma et al. 2018a, 2021b; Ay et al. 2019; Faust et al. 2014; Acharya et al. 2015; Bairy et al. 2016; Liao et al. 2017; Cai 2018; Uyulan et al. 2020; Qiao et al. 2020; Thoduparambil et al. 2020; Saeedi et al. 2020, 2021; Xie, et al. 2020; Qayyum et al. 2020; Khan et al. 2021; Seal et al. 2021; Bai et al. 2021). Some authors have also scoured and analysed texts from social media such as Twitter, Facebook and Reddit (Thoduparambil 2020; Saeedi 2020; Xie et al. 2020; Islam et al. 2018; Eichstaedt et al. 2018; Cacheda et al. 2019; Trotzek et al. 2020; Owen et al. 2020; Ramírez-Cifuentes et al. 2020; Safa et al. 2021; Tong et al. 2022; Gupta et al. 2022; Stankevich et al. 2018, 2020; Hussain et al. 2019; Alsagri and Ykhlef 2020). A few authors have explored the combination of audio and textural features (Alhanai et al. 2018; Park and Moon 2022), audio and visual recordings (Yang et al. 2017; Mallol-Ragolta et al. 2020; Saidi et al. 2020) while some others have used unique methods such as a combination of time series signal features (Zhou et al. 2015), measurement of electrodermal activity (Kim et al. 2018), magnetic resonance imaging (Kipli et al. 2013; Yamashita et al. 2020; Boeke et al. 2020), kinematic skeleton data (Li et al. 2021), photo-plethysmogram(PPG) signal features extraction (Khandoker 2017), gait characteristics (Wang et al. 2021) and optical flow visual-based method (Zhu et al. 2018). Haritha et al. (2017) explored respiratory signals for anxiety detection. However, apart from Ramirez et al. (2020) all these studies had only investigated the detection of depression and/or anxiety disorder alone, without linking to suicidal ideation. Ramirez et al. (2020) had uniquely assessed the suicide risk among social media users using text-based, statistical, behavioural, and image features. The study concludes that textural and behavioural features are the most promising for suicide risk assessment.
Discussion
Figure 4 details the different sources of data utilized by authors for the detection of depression and/or anxiety disorder. The figure shows that publicly available databases were used most widely, followed by data obtained from hospitals or research centres. The recording or construction of data were probably less commonly considered as these are often time-consuming and tedious, as compared to obtaining data from publicly available databases effortlessly. From Fig. 5, it is observable that mostly audio and/or facial video features, followed by EEG signals and texts from social media, were analyzed for the detection of depression and/or anxiety disorder. Also, from Fig. 6, it is evident that there are more studies on the detection of depression as compared to the detection of anxiety disorder or depression and anxiety disorder jointly. Furthermore, it can be reckoned from Fig. 6 that the trend for depression detection has been increasing from 2013 to 2022. It is also noticeable that more studies have been conducted for depression and/or anxiety disorder detection from 2019 to 2022. Within the same year range, a study on suicidal risk assessment was conducted in 2020. These could possibly be due to the hike in depression and anxiety disorders during the COVID-19 pandemic in children and adolescents (Śniadach et al. 2021). Figure 7 shows the number of studies that employed conventional machine learning and advanced deep learning models. From the figure, it is comprehendible that conventional machine learning techniques have been most commonly developed for the detection of depression and/or anxiety disorders. Furthermore, deep learning models have been explored since 2017, peaking in 2020, contending that these models have been gaining popularity in recent years.

Different sources of data

Pie chart representing the different types of input features used to detect depression and/or anxiety disorder

Bar graph detailing the number of studies conducted to detect depression and/or anxiety disorder from 2013 to 2022

Rejaibi et al. (2022) discussed that their recommended method of employing the recurrent neural network on audio features has some limitations wherein the generalization ability of this method to other datasets may be weaker as the shift from ideal circumstances of speech acquisition to speech in the rough conditions will increase the error rate of the method. They also compared the findings from other multimodal experiments and discussed that adding more features to the deep model enabled it to gain more knowledge about the identification of depression and was hence able to detect depression with higher accuracy. However, the computational complexity increases. They also stated that while adding visual features to the model increased the model performance by 20%, it appeared to be intrusive and invasive to patients. Park et al. (2022) conferred that their proposed method has limitations such as the inability to subdivide depression into mild or severe due to the way the model was developed in their study. They also discussed that the multimodal analysis of depression using text and voice data enhanced the classification accuracy as compared to using single data. Nasir et al. (2016) discussed that using geometric together with facial marker features improved the F1 score of their i-vector model compared to using the features separately. Adding polynomial feature sets to this resulted in a decline in model performance due to overfitting. They asserted that the i-vector model performed the best for audio features and polynomial parameterization of facial and geometrical features acted as the best video feature set. Yang et al. (2017) discussed that their developed hybrid DCNN-DNN model performed better than existing models, wherein text and semantic features had also been fused for depression detection besides audio and visual features.
Ramirez et al. (2020) debated that their observational study presents some limitations such as having no access to personal and medical information. Hence, the study lacks representativeness wherein analyses on gender, age, and location of users were not performed due to the lack of such information on Twitter. They also reported that while they had used text-based, statistical, behavioural, and image features for suicide risk assessment, the results could be improved by increasing textual and relational features.
Some authors also conducted a review study on depression detection. For instance, Wu et al. (2022) conducted a similar review study on depression detection using speech signals. While the authors reported that there has been a shift from exploring auditory features to deep model for speech depression recognition, they recommended overcoming depression detection challenges by collecting clinical information on depression to explore the core mechanism of speech in depression. They also concluded that combining multiple modalities for accurate and effective depression analysis is a possible trend in future research. While the review study by Wu et al. (2022) is also on depression detection, the authors focus more on employing deep learning methods with speech signals for depression detection, a contrast to this review study, which focuses on machine learning and deep learning models using various types of datasets for depression detection. We also quite differently propose the feature fusion method for future work. Nasser et al. (2020) conducted a review study on depression detection based on traditional machine learning methods using visual facial cues. The authors concluded that the Support Vector Machine technique is recommended for visual feature extraction methods for depression detection, due to the high accuracy obtained with a large number of subjects and with the usage of action units of full face. This review deviates from ours, as it only focuses on traditional machine learning techniques and visual facial cues as features for depression detection. In contrast to our study, William et al. (2021) conducted a review study on depression detection based on texts from social media. Based on the findings from the review, it has been established that the use of classifiers, support vector machines and probabilistic classifiers is the most common approach for depression detection using text analysis and that the BiLSTM combined with attention method generated the best results.
Salas-Zarate et al. (2022) also conducted a review study on detecting depression signs using social media. While the focus of this study is different from ours, the findings also vary. It has been established from the study that Twitter was the most studied social media, and word embedding was the most commonly employed linguistic feature extraction method and the support vector machine was the most prominent classifier that was used, for depression detection. In contrast to our study, Liu et al. (2022) reviewed studies that focused on a machine learning to determine depressive symptoms based on text mining for sentiment identification using social media data. The authors concluded that machine learning techniques could be effective in depression detection using text data from social media. In a different review study conducted by Guntuku et al. (2017), the authors analyzed the diverse approaches that were used to collate social media data comprising information regarding the users’ mental health. This varies from our study, which focuses on detecting depression and anxiety. The authors concluded that while depression and other mental illnesses are identifiable in many online environments, the generalizability of these studies to wider samples and benchmark for clinical criteria has not been determined.
Zhang et al. (2021) had conducted a review study on depression detection using virtual reality. The authors construed that while using virtual reality for depression detection has been increasingly acknowledged and virtual reality games have the potential to be designed for depression detection, they need to be improved. In another review study, Joshi et al. (2022) analysed how facial expressions, images, texts on social media, and emotional chatbots can effectively detect an individual’s emotions and depression. Various AI methods that have been employed for the analysis were discussed. From the findings, the authors established that depression, mood, and emotion could be detected by analyzing texts, videos, speech, gestures, or images through the employment of various machine learning and artificial intelligence-based models. In the review study by Aleem et al. (2022), the authors described various machine learning algorithms, along with their objectives and drawbacks, used for depression detection. They concluded that the support vector machine was the most prevalently used model, yielding high accuracies of above 75% for depression detection.
Hence, from the discussions above, it is clear that our review study differs from existing reviews in terms of focus and findings. Furthermore, based on the limitations and effects of modalities collated from some studies, it can be elucidated that using a fusion of features such as audio, visual, textual, and so on generally increases the classification accuracy of a deep model for depression detection, as the model gains more knowledge about depression identification. For instance, combining text and voice data improved the model’s performance as compared to using just a single data in the study by Park et al. (2022). However, one needs to be cautious about the type of features being analysed for different types of deep models. For instance, while adding visual features on top of speech signals increased the model’s performance in the study by Rejaibi et al. (2022), the computational complexity of the model increased. Furthermore, obtaining visual features can also appear as being intrusive and invasive to patients. Also, while the combination of the geometric and facial marker features improved the performance of the i-vector model, the addition of other features, like the polynomial, caused a decline in the model’s performance due to overfitting. Thus, while feature fusion is recommended, the types and number of features used depend on the type of deep model being developed, as quick depression detection is imperative in real-time settings.
From Tables 2, 3, 4 and 5, it is also notable that most authors had employed AI techniques for the studies. Some studies report high classification accuracies (95% and above) (Sharma et al. 2018a, 2021b; Ay et al. 2019; Afshan et al. 2018; Faust et al. 2014; Acharya et al. 2015; Uyulan et al. Jun. 2020; Thoduparambil et al. 2020; Saeedi et al. 2020, 2021; Qayyum et al. 2020; Khan et al. 2021; Seal et al. 2021; Khandoker 2017; Lech 2018; Tao et al. 2021) asserting the efficacy of using AI techniques for the detection of depression and/or anxiety disorder. There are advantages of using AI techniques for depression and/or anxiety detection, but there are pitfalls. Hence, the advantages and disadvantages of this review study are discussed below.
Advantages
-
1.
Detection of depression and/or anxiety using AI can be more rapid hence individuals with suicidal ideation can be identified faster.
-
2.
Depression and/or anxiety can be more accurately detected using AI tools, enabling suicidal ideation to be identified accurately.
-
3.
Using AI tools is cost-effective in diagnosing anxiety and/or depression, hence identifying suicidal ideation.
Limitations
-
1.
Using AI techniques for suicidal ideation may be presented with ethical (McKernan et al. 2018) and privacy issues (Gomes de Andrade et al. 2018).
-
2.
This study has not identified large databases of various ethnicities to better represent the global population.
-
3.
While this review discusses AI techniques for detecting depression and/or anxiety disorder, the features that best determine suicidal ideation in patients with depression and/or anxiety disorder have not been discovered.
Future avenues for research
Our review study underscores the significance of depression and/or anxiety disorder detection for identifying suicidal ideation, especially due to the unprecedented challenges brought about by the current COVID-19 pandemic. Findings from our review study demonstrate that audio and/or facial video features have been analyzed predominantly to detect depression and/or anxiety disorder. Furthermore, that machine learning techniques effectively detect depression and/or anxiety disorder. However, the features that best determine suicidal ideation in patients with depression and/or anxiety disorder have not been identified. Hence in our future work, we plan to gather large data from various ethnicities and propose to extract features such as facial images, EEG signals, speech signals, visual and clinical history features from huge population. The combination of features that best reduce the computational complexity of model, will be selected. The deep learning model which would train this feature set, would be kept in a secured cloud server. The classification result of the model (suicidal ideation is present/not present) would then be sent instantly to the mobile phones of involved clinicians, such as a psychiatrist, to assist in the stratification of clinical care. This idea is elucidated in Fig. 8.

Proposed scheme for the detection of suicidal ideation in individuals
Conclusion
Suicidal rates have been increasing globally, with adolescents having the highest prevalence rates of mental illness at 39%, wherein depression and anxiety mental health disorders have been identified as the main contributors to suicidal ideation. Traditional diagnostic methods such as self-report questionnaires and clinical interviews exhibit several limitations. AI tools have been employed to diagnose various diseases, including neurological illnesses. Hence this review paper summarizes studies that employed AI tools for the automated detection of depression and/or anxiety disorders. From the summary, it is apparent that AI tools are promising and can overcome the limitations of traditional depression and/or anxiety diagnostic methods. This study has also established that audio and/or facial video features have been most commonly analysed, followed by EEG signals, to detect depression and/or anxiety disorder. However, one main limitation of this review study is that the features that best determine suicidal ideation in patients with depression and/or anxiety disorder have not been discovered. Leveraging the recommended features for suicidal risk assessment by Ramirez et al. (2020), we hope to address this limitation in our future studies.
Data availability
Not admissible.
References
Acharya UR et al (2015) A novel depression diagnosis index using nonlinear features in EEG signals. Eur Neurol 74(1–2):79–83
Afshan A, Guo J, Park SJ, Ravi V, Flint J, Alwan A (2018) Effectiveness of voice quality features in detecting depression. In: Proceedings of the annual conference of the international speech communication association interspeech. pp 1676–1680
Ahmed A, Sultana R, Ullas MTR, Begom M, Rahi MMI, Alam MA (2020) A machine learning approach to detect depression and anxiety using supervised learning. In: 2020 IEEE Asia-Pacific Conference on computer science and data engineering (CSDE), pp. 1–6
Ahmedani BK et al (2014) Health care contacts in the year before suicide death. J Gen Intern Med 29(6):870–877
Albuquerque L, Valente ARS, Teixeira A, Figueiredo D, Sa-Couto P, Oliveira C (2021) Association between acoustic speech features and non-severe levels of anxiety and depression symptoms across lifespan. PLoS ONE 16(4):1–20
Aleem S, Huda NU, Amin R, Khalid S, Alshamrani SS, Alshehri A (2022) Machine learning algorithms for depression: diagnosis, insights, and research directions. Electronics 11(7):1111
Alhanai T, Ghassemi M, Glass J (2018) Detecting depression with audio/text sequence modeling of interviews. In: Proceedings of the annual conference of the international speech communication association interspeech. pp. 1716–1720
Alsagri HS, Ykhlef M (2020) Machine learning-based approach for depression detection in twitter using content and activity features. IEICE Trans Inf Syst E103D(8):1825–1832
Ay B et al (2019) Automated depression detection using deep representation and sequence learning with EEG signals. J Med Syst 43(7):1
Bai R, Guo Y, Tan X, Feng L, Xie H (2021) An EEG-based depression detection method using machine learning model. Int J Pharma Med Biol Sci 10(1):17–22
Bairy GM, Niranjan UC, Puthankattil SD (2016) Automated classification of depression Eeg signals using wavelet entropies and energies. J Mech Med Biol 16(3):1–13
Ballard ED et al (2016) Nocturnal wakefulness is associated with next-day suicidal ideation in major depressive disorder and bipolar disorder. J Clin Psychiatry 77(6):825–831
Bernert RA, Luckenbaugh DA, Duncan WC, Iwata NG, Ballard ED, Zarate CA (2017) Sleep architecture parameters as a putative biomarker of suicidal ideation in treatment-resistant depression. J Affect Disord 208:309–315
Boeke EA, Holmes AJ, Phelps EA (2020) Toward robust anxiety biomarkers: a machine learning approach in a large-scale sample. Biol Psychiatry Cogn Neurosci Neuroimaging 5(8):799–807
Brådvik L (2018) Suicide risk and mental disorders. Int J Environ Res Public Health 15(9):2028
Cacheda F, Fernandez D, Novoa FJ, Carneiro V (2019) Early detection of depression: social network analysis and random forest techniques. J Med Internet Res 21(6):e12554–e12554
Cai H et al (2018) A pervasive approach to EEG-based depression detection. Complexity. https://doi.org/10.1155/2018/5238028
Calear AL, Batterham PJ (2019) Suicidal ideation disclosure: Patterns, correlates and outcome. Psychiatry Res 278:1–6
Chlasta K, Wołk K, Krejtz I (2019) Automated speech-based screening of depression using deep convolutional neural networks. Procedia Comput Sci 164:618–628
Costanza A et al (2014) Neurobiology of suicide: Do biomarkers exist? Int J Legal Med 128(1):73–82
Cristianini N, Shawe-Taylor J (2000) An introduction to support vector machines and other kernel-based learning methods
Detecting depression using a framework combining deep multimodal neural networks with a purpose-built automated evaluation (XXXX) pp. 1–20
Dham S, Sharma A, Dhall A (2017) Depression scale recognition from audio, visual and text analysis
Di Matteo D et al (2021) Automated screening for social anxiety, generalized anxiety, and depression from objective smartphone-collected data: Cross-sectional study. J Med Internet Res 23(8):1–14
Eichstaedt JC et al (2018) Facebook language predicts depression in medical records. Proc Natl Acad Sci U S A 115(44):11203–11208
Eisenberg D, Gollust SE, Golberstein E, Hefner JL (2007) Prevalence and correlates of depression, anxiety, and suicidality among university students. Am J Orthopsychiatry 77(4):534–542
Espinola CW, Gomes JC, Pereira JMS, dos Santos WP (2021) Detection of major depressive disorder using vocal acoustic analysis and machine learning: an exploratory study. Res Biomed Eng 37(1):53–64
Faust O, Ang PCA, Puthankattil SD, Joseph PK (2014) Depression diagnosis support system based on eeg signal entropies. J Mech Med Biol 14(3):1–20
Franco-Martín MA, Muñoz-Sánchez JL, Sainz-de-Abajo B, Castillo-Sánchez G, Hamrioui S, de la Torre-Díez I (2018) A systematic literature review of technologies for suicidal behavior prevention. J Med Syst 42(4):71
Gavrilescu M, Vizireanu N (2019) Predicting depression, anxiety, and stress levels from videos using the facial action coding system. Sensors 19(17):3693
Gomes de Andrade NN, Pawson D, Muriello D, Donahue L, Guadagno J (2018) Ethics and artificial intelligence: suicide prevention on facebook. Philos Technol 31(4):669–684
Gould TD et al (2017) Animal models to improve our understanding and treatment of suicidal behavior. Transl Psychiatry 7(4):e1092–e1092
Grossi E, Buscema M (2007) Introduction to artificial neural networks. Eur J Gastroenterol Hepatol 19(12):1046–1054
Guntuku SC, Yaden DB, Kern ML, Ungar LH, Eichstaedt JC (2017) Detecting depression and mental illness on social media: an integrative review. Curr Opin Behav Sci 18:43–49
Guntuku SC, Preotiuc-Pietro D, Eichstaedt JC, Ungar LH (2019) What twitter profile and posted images reveal about depression and anxiety. In: Proceedings of 13th International conference on web and social media, ICWSM 2019, no. Icwsm. pp. 236–246
Guo W, Yang H, Liu Z, Xu Y, Hu B (2021) Deep neural networks for depression recognition based on 2D and 3D facial expressions under emotional stimulus tasks. Front Neurosci. https://doi.org/10.3389/fnins.2021.609760
Gupta S, Goel L, Singh A, Prasad A, Ullah MA (2022) Psychological analysis for depression detection from social networking sites. Comput Intell Neurosci 2022:4395358
Haritha H, Negi S, Menon RS, Kumar AA, Kumar CS (2017) Automating anxiety detection using respiratory signal analysis. In: 2017 IEEE region 10 symposium (TENSYMP). pp. 1–5
He L, Cao C (2018) Automated depression analysis using convolutional neural networks from speech. J Biomed Inf. https://doi.org/10.1016/j.jbi.2018.05.007
“Health, United States 2004: with chartbook on trends in the health of Americans and updated tables (2005) Med Benefits 22(22): 12
Hu LY, Huang MW, Ke SW, Tsai CF (2016) The distance function effect on k-nearest neighbor classification for medical datasets. Springerplus. https://doi.org/10.1186/s40064-016-2941-7
Hussain J et al (2019) Exploring the dominant features of social media for depression detection. J Inf Sci 46(6):739–759
Islam MR, Kabir MA, Ahmed A, Kamal ARM, Wang H, Ulhaq A (2018) Depression detection from social network data using machine learning techniques. Heal Inf Sci Syst 6(1):1–12
Izadinia N, Amiri M, Jahromi RG, Hamidi S (2010) A study of relationship between suicidal ideas, depression, anxiety, resiliency, daily stresses and mental health among Tehran university students. Proc Soc Behav Sci 5:1615–1619
Jahmunah V et al (2019) Automated detection of schizophrenia using nonlinear signal processing methods. Artif Intell Med 100:101698
Joe S, Bryant H (2007) Evidence-based suicide prevention screening in schools. Child Sch 29(4):219–227
Joshi ML, Kanoongo N (2022) Depression detection using emotional artificial intelligence and machine learning: a closer review. Mater Today Proc 58:217–226
Kaminsky Z et al (2015) Epigenetic and genetic variation at SKA2 predict suicidal behavior and post-traumatic stress disorder. Transl Psychiatry 5(8):e627–e627
Khan DM, Yahya N, Kamel N, Faye I (2021) Automated diagnosis of major depressive disorder using brain effective connectivity and 3D convolutional neural network. IEEE Access 9:8835–8846
Khandoker AH et al (2017) Suicidal ideation is associated with altered variability of fingertip photo-plethysmogram signal in depressed patients. Front Physiol 8:501
Kim AY et al (2018) Automatic detection of major depressive disorder using electrodermal activity. Sci Rep 8(1):1–9
Kingsford C, Salzberg SL (2008) What are decision trees? Nat Biotechnol 26(9):1011–1013
Kipli K, Kouzani A, Williams L (2013) Towards automated detection of depression from brain structural magnetic resonance images. Neuroradiology 55(5):567–584
Korczak DJ, D. D. C. Canadian Paediatric Society (2015) Suicidal ideation and behaviour. Paediatr Child Health 20(5):257–264
Lech M (2018) Detection of adolescent depression from speech using optimised spectral roll-off parameters. Biomed J Sci Tech Res 5(1):4350–4359
Li W, Wang Q, Liu X, Yu Y (2021) Simple action for depression detection: using kinect-recorded human kinematic skeletal data. BMC Psychiatry 21(1):1–11
Liao SC, Te Wu C, Huang HC, Cheng WT, Liu YH (2017) Major depression detection from EEG signals using kernel eigen-filter-bank common spatial patterns. Sensors 17(6):1385
Liu D, Feng XL, Ahmed F, Shahid M, Guo J (2022) Detecting and measuring depression on social media using a machine learning approach: systematic review. JMIR Ment Heal 9(3):e27244–e27244
Lopez Pinaya WH, Vieira S, R. Garcia-Dias, and A. Mechelli (2019) Autoencoders. Mach Learn Methods Appl Brain Disord. pp. 193–208
Malik S et al (2014) The association between sleep disturbances and suicidal behaviors in patients with psychiatric diagnoses: a systematic review and meta-analysis. Syst Rev 3(1):18
Mallol-Ragolta A, Zhao Z, Stappen L, Cummins N, Schuller B (2019) A hierarchical attention network-based approach for depression detection from transcribed clinical interviews. In: Proceedings of annual conference of the international speech communication association INTERSPEECH. 2019-September. pp. 221–225
Manetta AA, Ormand T (2005) A comparative analysis of substances used by suicidal and non-suicidal high school students. Sch Soc Work J 29(2):83–97
Mazza JJ (1997) School-based suicide prevention programs: are they effective? School Psych Rev 26(3):382–396
McKernan LC, Clayton EW, Walsh CG (2018) Protecting life while preserving liberty: ethical recommendations for suicide prevention with artificial intelligence. Front Psychiatry 9(December):1–5
De Melo WC, Granger E, Hadid A (2019) Combining global and local convolutional 3D networks for detecting depression from facial expressions. In: 14th IEEE international conference on automatic face gesture recognition, FG 2019
Naghavi M (2019l) Global, regional, and national burden of suicide mortality 1990 to 2016: systematic analysis for the Global Burden of disease Study 2016. BMJ 364:194
Nasir M, Jati A, Shivakumar PG, Chakravarthula SN, Georgiou P (2016) Multimodal and multiresolution depression detection from speech and facial landmark features. In: AVEC 2016: Proceedings of the 6th international workshop on audio/visual emotion challenge, co-located with ACM Multimedia. pp 43–50
Nasser SA, Hashim IA, Ali WH (2020) “A review on depression detection and diagnoses based on visual facial cues”, 2020 3rd Int. Conf Eng Technol Its Appl IICETA 2020:35–40
Niculescu AB et al (2017) Precision medicine for suicidality: from universality to subtypes and personalization. Mol Psychiatry 22(9):1250–1273
Nock MK et al (2008) Cross-national prevalence and risk factors for suicidal ideation, plans and attempts. Br J Psychiatry 192(2):98–105
Nugent AC, Ballard ED, Park LT, Zarate CA (2019) Research on the pathophysiology, treatment, and prevention of suicide: Practical and ethical issues. BMC Psychiatry 19(1):1–12
Oh SL et al (2018) A deep learning approach for Parkinson’s disease diagnosis from EEG signals. Neural Comput Appl 32:10927
Oh J, Oh B-L, Lee K-U, Chae J-H, Yun K (2020) Identifying schizophrenia using structural MRI With a deep learning algorithm. Front Psychiatry 11:16
Ooi KEB, Lech M, Allen NB (2013) Multichannel weighted speech classification system for prediction of major depression in adolescents. IEEE Trans Biomed Eng 60(2):497–506
Owen D, Camacho-Collados J, Espinosa-Anke L (2020) Towards preemptive detection of depression and anxiety in twitter. arXiv, pp. 82–89.
Pampouchidou A et al (2020) Automated facial video-based recognition of depression and anxiety symptom severity: cross-corpus validation. Mach vis Appl 31(4):1
Pampouchidou A, Marias K, Tsiknakis M, Simos P, Yang F, Meriaudeau F (2016) Designing a framework for assisting depression severity assessment from facial image analysis. In: IEEE 2015 Int. Conf. Signal Image Process. Appl. ICSIPA 2015 - Proc., no. October, pp. 578–583
Park J, Moon N (2022) Design and implementation of attention depression detection model based on multimodal analysis. Sustainability 14(6):3569
Pourmand A, Roberson J, Caggiula A, Monsalve N, Rahimi M, Torres-Llenza V (2018) Social media and suicide: a review of technology-based epidemiology and risk assessment. Telemed e-Health 25(10):880–888
Qayyum A, Razzak I, Mumtaz W (2020) Hybrid deep shallow network for assessment of depression using electroencephalogram signals. In: Lect Notes Comput Sci (including Subser Lect Notes Artif Intell Lect Notes Bioinformatics). 12534 LNCS: 245–257
Qiao Y, Duan L, Duan H, Wang C, Zhang X, Sha S (2020) Machine learning approaches for MDD detection and emotion decoding using EEG signals. Front Hum Neurosci 14:284
Quatieri TF, Williamson JR, Lammert AC, Heaton KJ, Palmer JS (2020) Noninvasive biomarkers of neurobehavioral performance. 24: 1
Ramírez-Cifuentes D et al (2020) Detection of suicidal ideation on social media: multimodal, relational, and behavioral analysis. J Med Internet Res 22(7):1–16
Rejaibi E, Komaty A, Meriaudeau F, Agrebi S, Othmani A (2022) MFCC-based recurrent neural network for automatic clinical depression recognition and assessment from speech. Biomed Signal Process Control 71:103107
Saeedi M, Saeedi A, Maghsoudi A (2020) Major depressive disorder assessment via enhanced k-nearest neighbor method and EEG signals. Phys Eng Sci Med 43(3):1007–1018
Saeedi A, Saeedi M, Maghsoudi A, Shalbaf A (2021) Major depressive disorder diagnosis based on effective connectivity in EEG signals: a convolutional neural network and long short-term memory approach. Cogn Neurodyn 15(2):239–252
Safa R, Bayat P, Moghtader L (2021) Automatic detection of depression symptoms in twitter using multimodal analysis. J Supercomput. https://doi.org/10.1007/s11227-021-04040-8
Saidi A, Ben Othman S, Ben Saoud S (2020) Hybrid CNN-SVM classifier for efficient depression detection system. In: Proceedings of international conference on advanced systems and emergent technologies IC_ASET2020. pp. 229–234
Salas-Zárate R, Alor-Hernández G, Salas-Zárate MDP, Paredes-Valverde MA, Bustos-López M, Sánchez-Cervantes JL (2022) Detecting depression signs on social media: a systematic literature review. Healthcare 10(2):1–22
Sardari S, Nakisa B, Rastgoo MN, Eklund P (2022) Audio based depression detection using Convolutional Autoencoder. Expert Syst Appl 189:116076
Seal A, Bajpai R, Agnihotri J, Yazidi A, Herrera-Viedma E, Krejcar O (2021) DeprNet: a deep convolution neural network framework for detecting depression using EEG. IEEE Trans Instrum Meas 70:1–13
Sharma M, Acharya UR (2021b) Automated detection of schizophrenia using optimal wavelet-based $$l_1$$norm features extracted from single-channel EEG. Cogn Neurodyn. https://doi.org/10.1007/s11571-020-09655-w
Sharma M, Achuth PV, Deb D, Puthankattil SD, Acharya UR (2018a) An automated diagnosis of depression using three-channel bandwidth-duration localized wavelet filter bank with EEG signals. Cogn Syst Res 52:508–520
Sharma N, Jain V, Mishra A (2018b) An analysis of convolutional neural networks for image classification. Procedia Comput Sci 132:377–384
Sharma N, Sharma R, Jindal N (2021a) Machine learning and deep learning applications: a vision. Glob Trans Proc 2:24
Sharma G, Parashar A, Joshi AM (2021b) DepHNN: a novel hybrid neural network for electroencephalogram (EEG)-based screening of depression. Biomed Signal Process Control 66:102393
Shinde SG, Tambe AC, Vishwakarma A, Mhatre SN (2020) Automated depression detection using audio features. 976–980
Śniadach J, Szymkowiak S, Osip P, Waszkiewicz N (2021) Increased depression and anxiety disorders during the covid-19 pandemic in children and adolescents: a literature review. Life 11(11):1188
Specht DF (1990) Probabilistic neural networks. Neural Netw 3(1):109–118
Stankevich M, Smirnov I, Kiselnikova N, Ushakova A (2020) Depression detection from social media profiles. Commun Comput Inf Sci 1223:181–194
Stankevich M, Isakov V, Devyatkin D, Smirnov I (2018) Feature engineering for depression detection in social media. In: ICPRAM 2018: Proceedings of the 7th international conference on pattern recognition applications and methods. 2018-January(Icpram): 426–431
Tao X, Chi O, Delaney PJ, Li L, Huang J (2021) Detecting depression using an ensemble classifier based on Quality of Life scales. Brain Inform. https://doi.org/10.1186/s40708-021-00125-5
Thoduparambil PP, Dominic A, Varghese SM (2020) EEG-based deep learning model for the automatic detection of clinical depression. Phys Eng Sci Med 43(4):1349–1360
Thompson EA, Eggert LL (1999) Using the suicide risk screen to identify suicidal adolescents among potential high school dropouts. J Am Acad Child Adolesc Psychiatry 38(12):1506–1514
Tong L et al (2022) Cost-sensitive boosting pruning trees for depression detection on twitter. IEEE Trans Affect Comput. https://doi.org/10.1109/TAFFC.2022.3145634
Trotzek M, Koitka S, Friedrich CM (2020) Utilizing neural networks and linguistic metadata for early detection of depression indications in text sequences. IEEE Trans Knowl Data Eng 32(3):588–601
Tuncer T, Dogan S, Acharya UR (2020) Automated detection of Parkinson’s disease using minimum average maximum tree and singular value decomposition method with vowels. Biocybern Biomed Eng 40(1):211–220
Uyulan C et al (2020) Major depressive disorder classification based on different convolutional neural network models: deep learning approach. Clin EEG Neurosci 52(1):38–51
van Heeringen K, Mann JJ (2014) The neurobiology of suicide. Lancet Psychiatry 1(1):63–72
Van Houdt G, Mosquera C, Nápoles G (2020) A review on the long short-term memory model. Artif Intell Rev 53(8):5929–5955
Vázquez-Romero A, Gallardo-Antolín A (2020) Automatic detection of depression in speech using ensemble convolutional neural networks. Entropy 22(6):688
Venkataraman D (2018) Extraction of facial features for depression detection among students. Int J Pure Appl Math 118(7):455–463
Victor E, Aghajan ZM, Sewart AR, Christian R (2019) Detecting depression using a framework combining deep multimodal neural networks with a purpose-built automated evaluation. Psychol Assess 31(8):1019–1027
Voulodimos A, Doulamis N, Doulamis A, Protopapadakis E (2018) Deep learning for computer vision: a brief review. Comput Intell Neurosci 2018:7068349
Wang Y, Wang J, Liu X, Zhu T (2021) Detecting depression through gait data: examining the contribution of gait features in recognizing depression. Front. Psychiatry 12:661213
Wei JKE et al (2020) Automated detection of Alzheimer’s disease using Bi-directional empirical model decomposition. Pattern Recognit Lett 135:106
William D, Suhartono D (2021) Text-based depression detection on social media posts: a systematic literature review. Procedia Comput Sci 179(2019):582–589
Williamson JR et al (2016) “Detecting depression using vocal, facial and semantic communication cues. In: AVEC 2016 - Proc. 6th Int. Work. Audio/Visual Emot. Challenge, co-located with ACM Multimed. 2016, pp. 11–18
World Health Organization (2014) Preventing suicide Preventing suicide. WHO Libr. Cat. Data, p. 89
Wu P, Wang R, Lin H, Zhang F, Tu J, Sun M (2022) Automatic depression recognition by intelligent speech signal processing: a systematic survey. CAAI Trans Intell Technol. https://doi.org/10.1049/cit2.12113
Xie Y et al. (2020) Anxiety and depression diagnosis method based on brain networks and convolutional neural networks. In: 2020 42nd annual international conference of the ieee Engineering in medicine and biology Society (EMBC). 1503–1506
Yadav U, Sharma AK (2022) A novel automated depression detection technique using text transcript. Int J Imaging Syst Technol. https://doi.org/10.1002/ima.22793
Yamashita A et al (2020) Generalizable brain network markers of major depressive disorder across multiple imaging sites. PLoS Biol 18(12):1–26
Yang L, Jiang D, He L, Pei E, Oveneke MC, Sahli H (2016) Decision tree based depression classification from audio video and language information. In: AVEC 2016—Proceedings of the 6th international workshop on audio/visual emotion challenge co-located with ACM Multimed. June 2018: 89–96
Yang L, Jiang D, Han W, Sahli H (2017) DCNN and DNN based multi-modal depression recognition. In: 2017 7th International conference on affective computing and intelligent interaction ACII 2017. 2018-Janua(May 2019): 484–489
Yeh HH et al (2019) Diagnosed mental health conditions and risk of suicide mortality. Psychiatr Serv 70(9):750–757
Zhang C, Luo H, Li Y (2021) Depression detection using virtual reality: a literature review. In: Proceedings of the Hawaii International Conference on System Sciences. 2020-Janua: 4001–4008
Zhang L, Duvvuri R, Chandra KKL, Nguyen T, Ghomi RH (2020) Automated voice biomarkers for depression symptoms using an online cross-sectional data collection initiative. Depress Anxiety 37(7):657–669
Zhou D et al (2015) Tackling mental health by integrating unobtrusive multimodal sensing. Proc Natl Conf Artif Intell 2:1401–1408
Zhu Y, Shang Y, Shao Z, Guo G (2018) Automated depression diagnosis based on deep networks to encode facial appearance and dynamics. IEEE Trans Affect Comput 9(4):578–584
Author information
Authors and Affiliations
Contributions
All authors have contributed to an acceptable and satisfying level.
Corresponding author
Ethics declarations
Conflict of interest
The authors have declared that no competing interests exist.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Barua, P.D., Vicnesh, J., Lih, O.S. et al. Artificial intelligence assisted tools for the detection of anxiety and depression leading to suicidal ideation in adolescents: a review. Cogn Neurodyn 18, 1–22 (2024). https://doi.org/10.1007/s11571-022-09904-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11571-022-09904-0