
Abstract
Glioblastoma (GB), a prevalent and highly malignant primary brain tumour with a very high mortality rate due to its resistance to conventional therapies and invasive nature, resulting in 5-year survival rates of only 4–17%. Despite recent advancements in cancer management, the survival rates for GB patients have not significantly improved over the last 10–20 years. Consequently, there exists a critical unmet need for innovative therapies. One promising approach for GB is Targeted Alpha Therapy (TAT), which aims to selectively deliver potentially therapeutic radiation doses to malignant cells and the tumour microenvironment while minimising radiation exposure to surrounding normal tissue with or without conventional external beam radiation. This approach has shown promise in both pre-clinical and clinical settings. A review was conducted following PRISMA 2020 guidelines across Medline, SCOPUS, and Embase, identifying 34 relevant studies out of 526 initially found. In pre-clinical studies, TAT demonstrated high binding specificity to targeted GB cells, with affinity rates between 60.0% and 84.2%, and minimal binding to non-targeted cells (4.0–5.6%). This specificity significantly enhanced cytotoxic effects and improved biodistribution when delivered intratumorally. Mice treated with TAT showed markedly higher median survival rates compared to control groups. In clinical trials, TAT applied to recurrent GB (rGB) displayed varying success rates in extending overall survival (OS) and progression-free survival. Particularly effective when integrated into treatment regimens for both newly diagnosed and recurrent cases, TAT increased the median OS by 16.1% in newly diagnosed GB and by 36.4% in rGB, compared to current standard therapies. Furthermore, it was generally well tolerated with minimal adverse effects. These findings underscore the potential of TAT as a viable therapeutic option in the management of GB.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Glioblastoma (GB), an aggressive brain cancer, exhibits poor prognosis with a 5-year survival rate of 4-17% |
Targeted Alpha Therapy (TAT) emerges as a promising approach, delivering therapeutic radiation doses to malignant cells while minimising exposure to normal tissue. |
TAT demonstrated high binding affinity to targeted cells, dose-dependent reduction in cell viability, and cell cycle arrest in G2/M phase. |
Intratumoral delivery of targeted agents showed promising biodistribution with significant tumour accumulation. |
TAT is generally well-tolerated with minimal side effects, irrespective of the specific alpha-emitting radionuclide used. |
1 Introduction
Glioblastoma (GB) is the most aggressive form of malignant primary brain cancer, carrying an extremely poor prognosis [1]. International studies have shown an annual incidence rate of approximately 0.59–5 per 100,000 persons, with an increasing incidence with age, and have indicated a rise in incidence number [2]. Globally, GB is among the most common primary malignant brain tumour, with a 5-year survival rate ranging from 4 to 17% [3].
GB, previously known as glioblastoma multiforme, is classified as a grade 4 tumour according to the World Health Organization (WHO) grading system for brain tumours [1]. GB is pathologically known to be highly heterogenous, invasive, proliferating and hypoxic [1, 4,5,6,7]. These characteristics collectively contribute to the aggressive and therapy resistant nature of GB, making it one of the most difficult types of brain cancers to achieve long-term control. The current standard treatment for GB patients involves maximal safe surgical resection followed by external beam radiotherapy (EBRT) plus concomitant and adjuvant chemotherapy with temozolomide (TMZ) [8]. Due to the diffuse invasiveness of GB, achieving a macroscopic and microscopic complete surgical resection is near impossible [9]. The persistence of subclinical infiltrating tumour cells at the edge of the tumour bed dispersed in the adjacent white matter pathways not eradicated by adjuvant non-surgical oncological treatments ultimately results in disease recurrence and progression [9].
Considering the low survival rate associated with the current standard treatment protocols compared to many other cancers, research has shifted its focus to new therapeutic approaches to address the challenges posed by GB. One promising approach for GB is Targeted Alpha Therapy (TAT), which aims to selectively deliver therapeutic radiation doses using alpha particles to the tissue of remaining malignant tumour cells and the tumour microenvironment, while minimising radiation exposure to surrounding critical normal tissue [10].
1.1 Targeted Alpha Therapy
TAT is a form of Target Radionuclide Therapy (TRT), which involves the administration of alpha-emitting radionuclides into the patient, either intravenously or intratumorally/locally. These radionuclides specifically accumulate at tumour sites due to their inherent chemical properties or active targeting mechanisms, and release ionising alpha particles that can precisely target cancer cells [10]. There are three main methods of delivering TAT:
-
i.
Passive targeting: This approach utilises radionuclides that naturally accumulate in certain tissues without a targeting agent. An example is Radium-224 (Ra-224), which has a natural affinity for bone and is under investigation for potential use in glioblastoma (GB) treatment due to its ability to target bone-like or calcified tumour tissues [11, 12].
-
ii.
Active targeting: In this more common approach, alpha-emitting radionuclides are conjugated to monoclonal antibodies (mAb), peptides or small molecules that target tumor-associated antigens expressed on cancer cells [13]. This method ensures that the radionuclide is delivered directly to the cancer cells, increasing the treatment's efficacy and reducing uptake by normal tissues.
-
iii.
Intratumoral implants: Referred to as diffusing alpha-emitters radiation therapy (DaRT), this method involves implanting sources ('seeds') containing low levels of Ra-224 directly into the tumour [14]. This strategy is akin to brachytherapy, a well-established treatment using radiation sources placed inside or next to the area requiring treatment. Both DaRT and brachytherapy deliver localised radiation; however, DaRT provides a targeted alpha-emission that may offer enhanced tumour control with minimal impact on surrounding healthy tissues [14].
Another form of TRT is Targeted Beta Therapy (TBT), which uses beta-emitting radionuclide instead of alpha. TBT is currently the most common TRT approach; however, TBT has two major drawbacks: beta-particles have a long range in tissue, ranging from 1 to 10 mm, resulting in unwanted exposure to neighbouring healthy tissue [15,16,17]; and a low linear energy transfer (LET) of around 0.2 keV/μm [16]. LET is a measurement of the mean rate of energy deposited locally along the track of a charged particle. Therefore, with low LET, ionisations within the cell are not as dense, causing a lower probability of irreparable DNA double-strand breaks and base chemical modifications that induce apoptosis (Fig. 1) [10].

Comparison of therapeutic particle ranges, LET, and DNA damage potencies (made in Canva)
Alpha-emitting radionuclides undergo radioactive decay releasing alpha-particles, a helium nucleus consisting of two protons and two neutrons with an electric charge of +2. Unlike beta-particles, alpha-particles have a much shorter range of 50–100 µm and a higher LET, which varies between 50 keV/μm and 230 keV/μm depending on the alpha-emitting isotope used [10]; therefore, they can deliver higher potent short-ranged radiation directly to the tumour cells while sparing more of the neighbouring healthy tissue (Fig. 1). Additionally, cell death due to alpha-particles are near-independent of oxygen level or rate of proliferation, which makes TAT suitable for treating hypoxic tumours such as GB [18].
The high LET of alpha particles significantly increases their Radiobiological Effectiveness (RBE) compared to beta particles. RBE is a comparative measure of cellular damage done by different types of radiation, reflecting the efficiency of energy deposition at the molecular level. Remarkably, while the general RBE for alpha particles is typically in the range of 5–10, it can rise dramatically to around 120 in scenarios where alpha particles are targeted internally [15]. This extremely high RBE is due to the fact that targeted alpha particles, due to their short range and concentrated energy deposition, are much more likely to hit and kill cancer cells directly. Most targeted cancer cells receive a large fraction of the alpha radiation's energy directly to the cell nucleus, which induces double-strand DNA breaks. In contrast, beta particles, their longer range and diffuse energy spread result in a significantly smaller fraction of the radiation dose, effectively damaging the targeted cells, and affirming their RBE of about 1 [15]. As such, there has been increased interest in TAT in recent years due to its advantageous characteristics over TBT.
This review aims to provide an overview of the current literature on TAT for GB treatment. Specifically, the focus is on studies investigating TAT efficacy in both pre-clinical models and clinical studies. Additionally, the review aimed to identify and highlight existing gaps in knowledge, and scopes for future research.
2 Search Method
To conduct a review of the existing literature on TAT for GB, a systematic literature search was performed across three databases: MEDLINE, Scopus and Embase. The search strategy (detailed in Appendix A, Online Supplemental Material) was developed in collaboration with a University of South Australia (UniSA) librarian, adhering to PRISMA 2020 guidelines [19]. Additionally, a grey literature search using Google Scholar was conducted, with the first 10 pages of results extracted for screening. The screening process was done through Covidence (Veritas Health Innovation, Melbourne, Australia), a specialised software for literature reviews, and after removing duplicates, exclusion criteria were applied, excluding conference abstracts, posters, review articles, and non-English language publications.
Subsequently, a review of the abstracts and full texts of the remaining papers was conducted independently by two reviewers (MES and EB), and any conflicts were discussed and resolved. Following this evaluation, 34 papers were deemed relevant and selected for inclusion in this review. Figure 2 is the overview of the search and article inclusion process. Although systematic approaches were used in the data extraction and analysis, the large variation in reporting and the small number of studies made meta-analysis of the literature not possible. Therefore, the approach taken involved integrating and synthesising the overall results.

Overview of the search method
3 Results and Discussion
The results and discussion of this review are organised into sections that detail the use of various radionuclides, as well as summarising findings from in vitro, in vivo and clinical studies relevant to TAT in GB.
3.1 Radionuclides
A wide array of isotopes has been explored for TAT in the context of GB. Among these isotopes, Astatine-211 (At-211) has been used in 14 pre-clinical studies, Bismuth-213 (Bi-213) in five clinical trials, and Actinium-225 (Ac-225) in six pre-clinical studies and one phase I clinical trial. Each isotope exhibits a unique set of characteristics. Ac-225, characterised by its 100% α-emission, a range of 0.04–0.10 mm, and a half-life (T1/2) of 238.10 h (~ 10 days), is shown to offer several advantages [20,21,22,23,24,25,26,27]. Notably, it exhibits compatibility with DOTA-complexation, rendering it a versatile choice for a variety of compounds [26]. Furthermore, its relatively extended half-life (T1/2) allows for enhanced transport and more efficient distribution before radioactive decay, particularly beneficial when treating larger tumour volumes, as indicated by Cordier et al. [28]. However, the longer T1/2 of Ac-225 results in the generation of multiple alpha particles due to its rapid decay chain (as depicted in Fig. 3). Moreover, recoiled daughters might impact its stability. Studies involving Ac-225 can be found in the references [20,21,22,23,24,25,26].

Ac-225 decay chain; photons with a branching ratio > 3% relative to 225Ac decay are shown
Bi-213, which boasts a 2.2% α-emission and 97.8% β-emission, possesses a range of 0.05–0.10 mm and a T1/2 of 0.77 h [27,28,29,30,31,32,33]. Like Ac-225, it can be effectively complexed with DOTA, offering a straightforward and universal solution [26, 30,31,32]. However, its short T1/2 and gamma-energy combination make it less efficient in terms of tumour distribution before radioactive decay [28]. The primary drawback of Bi-213 is its brief T1/2, which affects its residence time within critical GB cells. In these cases, the ratio between cell membrane coverage (receptor affinity) and time plays a pivotal role. Studies involving Bi-213 are listed in the references [28,29,30,31,32,33].
Lastly, At-211, featuring 42.0% α-emission and 58.0% electron capture, possesses a range of 0.05 mm and a T1/2 of 7.20 h [27, 34,35,36,37,38,39,40,41,42,43,44,45,46,47]. Its longer T1/2 gives it the potential to have a more advantageous biodistribution. However, At-211 is limited to applications involving mAb and smaller fragments, which can often exhibit low biological and chemical stability. Relevant studies pertaining to 211At are listed in the references [34,35,36,37,38,39,40,41,42,43,44,45,46,47].
3.2 Pre-Clinical Studies
A total of 26 pre-clinical papers were identified that investigated various aspects of TAT for GB. There were 12 in vitro studies, four in vivo studies, nine combined in vitro/in vivo studies, and one modelling study. A summary of pre-clinical studies is presented in Tables 1 and 2.
3.2.1 In Vitro Studies
In vitro studies primarily focused on several key aspects, including the binding affinity of different targeting agents, clonogenic survival/cell viability, and the potential for cell cycle arrest.
The binding affinity and binding rate of labelled alpha emitters were consistently high compared to non-targeted and unlabelled emitters. Notably, studies conducted by Zalutsky et al. [39, 41] and Larsen et al. [36] demonstrated that At-211 conjugated to mAbs 81C6/Mel-14 and 2'-deoxyuridine (AUdR) exhibited high binding specificity to targeted cells (ranging from 60.0% to 84.2%) and low binding to non-targeted cells (4.0–5.6%). Moreover, Ma et al. [42] and Liu et al. [43] found that the binding rates to targeted cells were 24.9% and 32.0%, respectively, while the binding rate to non-targeted cells was less than 7%. These studies explored At-221 conjugated to either a heterodimeric peptide (targeting vascular endothelial growth factor receptor (VEGFR) and integrins) or a fibroblast activation protein inhibitor (FAPI).
The therapeutic effectiveness of TAT was assessed in various ways in the literature, including cell viability, relative biological effectiveness (RBE), survival fraction of GB cells at specific absorbed dose rates, and activity concentration resulting in a specific survival rate. Larsen et al. [35, 36] and Rosenkranz et al. [37] investigated the activity concentrations resulting in a 37% survival rate (A37) of GB cells using At-211 conjugated to mAbs 81C6/Mel-14, AUdR, and engineered modular recombinant transporters. The A37 values for conjugated At-211 were significantly lower (4.4–56.6 kBq/ml) compared to free At-211 (32.6–132 kBq/ml). These findings underscore the heightened effectiveness and precision of At-211 conjugated to a targeting agent in killing clonogenic GB cells.
Majkowska-Pilip et al. [25], Ma et al. [42] and Liu et al. [43] reported on cell viability; a dose-dependent decrease in all studies was observed. Ac-225 conjugated to substance-P reduced cell viability to 50% at 50 kBq/ml; At-211 conjugated to FAPI and control reduced viability to 42.1% and 56.5% at 92 kBq/ml, respectively; and At-211 conjugated to heterodimeric peptide and control reduced viability to 47.5% and 62.0% at 75 kBq/ml, respectively. Furthermore, Majkowska-Pilip et al. [25], Ma et al. [42] and Liu et [43] demonstrated significant cell cycle arrest in the G2/M phase in treated cell lines compared to control, with treated cells in G2/M phase ranging from 62.1% to 80% and control cells at 11.9% to 36.6% (cells are more radiosensitive in these phases).
The therapeutic effectiveness of TAT compared to other treatment modalities was explored in several studies. Carlin et al. [38, 40] and Zalutsky et al. [39] highlighted that the 2 Gy survival fraction (SF2) for At-211 was significantly lower than that of Iodine-131 (I-131) and EBRT, meaning that At-211 is much more effective in killing cancer cells when exposed to a 2 Gy dose compared to I-131 and EBRT (i.e., more cytotoxic at this radiation dose). Additionally, Barazznol et al. [48] reported that the RBE of alpha particles compared to x-rays and protons was higher, with RBE10 (calculated at 10% survival) and RBE3Gy (survival level after 3 Gy) being 1.17 and 1.35 for protons and 1.84 and 3.79 for alpha particles, respectively. The RBE is a measure of how effective a particular type of radiation is at causing biological damage, relative to x-rays, although both alpha and protons have a higher RBE than X-rays, alpha particles had the highest RBE, indicating that they are more effective in causing biological damage.
Overall, the pre-clinical in vitro studies on TAT have shown its potential as an effective therapeutic approach for GB treatment. The high binding affinity to targeted cells, dose-dependent reduction in cell viability, and cell cycle arrest and enhanced cytotoxicity compared to other treatments collectively highlight the promising aspects of TAT.
Building on the existing in vitro studies that detail the binding affinity of TAT, cell viability, cell cycle arrest, and other cellular responses in GB treatment, further research is suggested in the following areas to address existing knowledge gaps. This recommendation aligns with the International Atomic Energy Agency (IAEA) [49] guidance for pre-clinical studies with radiopharmaceuticals. Below is an outline of studies that are covered by the included literature and those requiring further investigation:
IAEA Recommended Studies—Covered in Included Literature:
-
i.
Binding affinity and specificity: Several studies have examined the binding affinity and specificity of radiopharmaceuticals like At-211 conjugated with monoclonal antibodies and peptides. For example, Zalutskys and Larsen's [35, 39] studies show significant differences in binding to target versus non-target cells, which aligns with the IAEA's emphasis on understanding binding characteristics.
-
ii.
Cell viability and clonogenic survival: Studies (Table 1) have provided detailed clonogenic survival curves, showing how different doses affect survival rates of GB cells, addressing the IAEA's recommendation for cell viability studies.
-
iii.
Cellular response to radiation: The cellular response to radiation was also explored, including dose-dependent effects and RBE, contributing to understanding the efficacy of different types of radiation as recommended by IAEA.
-
iv.
Therapeutic efficacy: Carlin's [38, 40] studies demonstrated higher cytotoxicity and absorbed dose effectiveness of At-211 compared to I-131 and external beam radiation, providing crucial data on the therapeutic potential of radiopharmaceuticals.
IAEA Recommended Studies—Require Further Investigation:
-
i.
Internalisation and intracellular/subcellular distribution: Despite detailed binding and viability studies, the internalisation dynamics and subcellular localisation of tracers post-binding are not clearly addressed in the summarised studies. These are crucial for understanding how tracers behave inside cells after binding to their targets.
-
ii.
Blocking studies: Although high binding specificity is demonstrated, there is no clear mention of blocking studies to assess the saturability and specificity of binding beyond competitive interactions. Such studies would help confirm the selectivity and potential off-target effects.
-
iii.
Efflux pump assays and blood-brain barrier permeability: There is a lack of explicit studies on how these radiopharmaceuticals interact with the blood-brain barrier or efflux pumps, which is critical for CNS-targeted therapies like those for GB.
-
iv.
Metabolite analysis: It is important to understand the metabolic pathways and by-products after tracer uptake, which has not been detailed in the summary. This could affect both efficacy and toxicity profiles of the radiopharmaceuticals.
-
v.
Functional/efficacy assays beyond viability: Additional functional assays to evaluate the biochemical pathways affected post-binding could provide deeper insights into the mechanistic effects of TAT agents on GB cells.
By addressing these gaps, further research can enhance the understanding of the comprehensive therapeutic profile of TAT, particularly focusing on areas like tracer internalisation and metabolic processing, which are pivotal for ensuring the safety and effectiveness of treatment strategies for GB.
3.2.2 In Vivo Studies
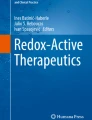
In vivo studies primarily focused on three aspects: biodistribution of targeted agents, median survival in treated animals versus control groups, and tumour growth/size reduction. Figure 4 provides a summary of the biodistribution of various targeting agents. It reveals that intravenous delivery of targeted agents resulted in tumour uptake ranging from 0.13% to 20.0% of the total injected dose per gram (%ID/g), while intratumoral delivery demonstrated a significantly higher tumour accumulation of 132.5%ID/g [20, 21, 39, 41,42,43]. Furthermore, intravenous injection groups displayed higher tumour-to-organ ratios, with the most significant uptake observed in the liver, spleen and kidneys (Fig. 4B) [20, 41,42,43]. Ma et al. [42] reported more favourable results concerning the tumour-to-organ ratio with intratumoral injection, including tumour-to-liver, tumour-to-kidney, and tumour-to-blood ratios of 11.13, 6.39, and 14.17, respectively, post-injection.

Biodistribution of the targeting agent. (A) The tumour accumulation (red arrow indicates the intratumoral injection result). (B) The intravenous injection distribution in tumour and healthy organs
The studies revealed promising results in terms of the median overall survival (OS) of mice treated with TAT. Treated groups demonstrated OS ranging from 14.6 to 41 days, while untreated/control groups ranged from 9 to 23 days [20, 21, 24, 42,43,44]. TAT also exhibited a dose-dependent tumour suppression effect, with doses between 180 and 740 kBq resulting in reduced tumour volume ranging from 48% to 77% [12, 37, 42, 43, 45]. Additionally, Watabe et al. [45] reported that TAT effectively suppressed tumour growth, with tumour size ratios of 0.6, 0.4 and 0.25 post-injection at 100, 500 and 1,000 kBq, respectively.
Overall, the in vivo studies underscore the potential of TAT in improving overall survival and reducing tumour growth in animal models. The findings suggest that intratumoral delivery may offer more favourable outcomes in terms of biodistribution and tumour-to-organ ratio. Further research is needed to optimise dosing and administration methods to maximise the therapeutic benefits of these targeted agents.
3.3 Clinical Studies
Despite many recent advances in anti-cancer treatment modalities, (surgery, external beam radiotherapy and chemotherapy) over the last decade, the overall median survival (OS) for newly diagnosed primary GB remains extremely low, ranging from 12 to 18 months [53,54,55,56,57,58]. There are currently limited clinical data, with only six phase I clinical studies identified, four of which were conducted by the same research group. A summary of these phase I studies is presented in Table 3, where different alpha-emitting radionuclides, such as At-211, Bi-213 and Ac-225, conjugated to various targeting agents, were investigated. The primary aim of these clinical studies is to assess the viability of TAT as a treatment option for recurrent glioblastoma (rGB).
In a clinical trial by Zalutsky et al. [34], At-211 was employed alongside Ch81C6, targeting Tenascin C, in 14 rGB patients. The treatment plan involved doses ranging from 71 MBq to 347 MBq, all conjugated to 10 mg of Ch81C6 within the surgical cavity. The study reported a median OS of 12 months, with observed variations in surgical cavity resection site volumes, highlighting the need for further evaluation of multiple dose administration schedules to optimise treatment efficacy.
Cordier et al. [28] delved into the use of Bi-213 in combination with Substance P/NK-1, focusing on two critically located GB patients. Patient 1 (P1) received one cycle of 1.07 GBq, and Patient 2 (P2) received one cycle of 1.92 GBq, involving intratumoral injection via two to three catheters with three to five injections per cycle. The findings from this investigation revealed a median OS-t (overall survival from the start of treatment (first cycle of TAT) to death from any cause) of 16 months for P1 and 19 months for P2, and no acute local or systemic toxicity were reported. However, both patients eventually experienced tumour recurrence, with the recurrence period spanning from 2 to 11 months post-treatment. Notably, the study showed that smaller tumours displayed a comprehensive radionecrotic transformation, while larger tumours primarily exhibited necrosis in the proximity of the catheters used for injection. This discrepancy in response is likely attributable to the relatively short T1/2 of Bi-213 (T1/2 of 0.77 h), potentially resulting in inadequate intratumoral distribution before radioactive decay occurs. These results have raised valid concerns regarding the suitability of Bi-213 for the treatment of larger tumour volumes. It suggests that Ac-225 (T1/2 of 238.10 h) may be a more appropriate choice for addressing such cases, potentially offering improved outcomes.
The studies conducted by Krolicki et al. [26, 30,31,32] have contributed to advancing our understanding of TAT for GB. Their clinical trials began in 2018 when they investigated the use of Bi-213 conjugated with Substance P/NK-1 in nine patients with secondary GB. This results showed a diverse spectrum of outcomes, with a median OS of 16.4 months. In 2019, Krolicki et al. [32] expanded their scope to include 20 rGB patients, categorised into NIH0, NIH1 and NIH2 groups based on the National Institutes of Health (NIH) clinical grading scale for GB. This scale ranges from 0 to 5, reflecting various levels of neurological function, with higher grades indicating worse neurological function. Notably, the study observed longer OS and PFS in patients with lower-grade NIH scores, highlighting the significance of patient stratification.
Their exploration of TAT continued with studies involving 21 and 29 patients with primary and secondary rGB, employing Ac-225 and Bi-213 conjugated with Substance P/NK-1, respectively. Surprisingly, the treatment effect appeared independent of the radioisotope injected activity within the range of 10–30 MBq. This could be attributed to the limited diffusion of the treatment into the tumour, predominantly influencing the peripheral regions near the cavity. Furthermore, the study noted the potential influence of tumour heterogeneity, exemplified by a diverse range of apparent diffusion coefficient (ADC) values observed in MRI scans, partly explaining the varied responses to treatment. The data from these trials showed that the OS time in primary GB increased to 23.6 months with Bi-213 and 21 months with Ac-225, and OS in rGB increased to 10.9 months with Bi-213 and 12 months with Ac-225 when compared to the OS with standard treatment [53,54,55,56,57,58]. Notably, the analysis showed a statistically significant longer OS-d and OS-r/c time for patients with secondary glioblastoma compared to those with primary glioblastoma. However, when comparing PFS and OS-t (the two most treatment-related parameters), both groups of patients demonstrated similar outcomes. This implies that local treatment administration of radionuclides effectively targets tumours in both patient groups, regardless of the genetic attributes of their tumours.
3.3.1 Delivered Dose
The published clinical studies touch upon factors influencing the radiation dose delivered by TAT, such as the total injected activity and the diffusion rate of the radiopharmaceutical into the tumour. However, specific numerical values for the actual radiation doses delivered to the tumour/target volume are not provided. The biodistributions of the radiopharmaceutical were assessed using PET/CT post-injection, and similar to the in vivo studies, the clinical studies reported on the %ID retaining in the blood pool. All clinical studies consistently reported a high retention of the radiopharmaceutical at the target site, a finding further confirmed by the low percentage values of the injected dose in the blood pool (maximum values in all studies were < 4–6 %ID) [26, 28, 30,31,32, 34]. The absence of detailed information on the translated dose to the target volume complicates the ability to establish definitive correlations between administered activities; a dose-response relationship and therapeutic outcomes becomes challenging.
Understanding the actual radiation dose delivered to the tumour is essential for optimising treatment protocols, ensuring adequate tumour coverage, and minimising treatment associated side effects. This highlights the critical need for further dosimetry studies that take into account the unique characteristics of the radiopharmaceutical, diffusion rates, and potential variations in individual tumour structures.
Additionally, while reports consistently detail the amount of activity administered, they lack quantification of how effectively this activity translates into energy deposition at the targeted volume. To bridge this gap, multiple imaging sessions are needed to estimate the activity within normal tissues and tumours. These imaging data allow for the reconstruction of a detailed spatial dosimetry based on time-activity curves. It is essential to ascertain whether the radiopharmaceutical accumulates uniformly, achieves sufficient intensity, and reaches the peripheries of the tumour where residual cells may exist. This dual challenge of delivery and dosimetry underscores the need for advanced imaging techniques and precise dosimetric calculations to ensure that the radiation dose is accurately distributed throughout the tumour volume.
3.3.2 Toxicities
Toxicity assessments across the studies by Zalutsky et al. [34], Cordier et al. [28] and Krolicki et al. [26, 30,31,32] revealed that TAT is a generally well tolerated treatment with minimal side effects (Table 3). Notably, toxicity profiles were similar between Ac-225 and Bi-213 when doses were equivalent, suggesting that adverse effects may be more related to dosing than the specific radionuclide used [30]. These findings underscore the importance of precise dosing considerations and careful dose-escalation protocols to minimise potential risks associated with targeted radionuclide therapies, particularly for Ac-225. Continued research and clinical monitoring are essential to refine treatment protocols and ensure patient safety.
Overall, these studies contribute to understanding TAT for GB, emphasising patient stratification and dosimetry considerations. Despite variations in outcomes, local administration of radionuclides demonstrated effective tumour targeting, impacting both primary and secondary GB. Further exploration is crucial for optimising treatment schedules and improving overall survival and progression-free survival for GB patients.
4 Delivery Methods
The blood-brain barrier (BBB) is a semi-permeable membrane, comprised of specialised endothelial cells supported by pericytes and astrocytes, that tightly regulates the passage of molecules into the brain [59]. The BBB's selective physical barrier, which restricts the entry of molecules larger than 400 Daltons, poses a challenge for delivering therapeutic agents to treat brain tumours [59]. Furthermore, brain tumours compromise the BBB, resulting in the formation of the blood-tumour barrier (BTB), characterised by heterogeneous permeability and active efflux mechanisms [60]. This creates a challenging scenario for drug delivery, as the efficacy of therapies is impeded by the expression of transport proteins and efflux transporters in both the BBB and the BTB [60].
To overcome these barriers, various strategies have been explored. One avenue is the use of peptide-drug conjugates, where peptides facilitate targeted drug delivery [61]. Peptide-drug conjugates exploit specific receptors on target tissues for selective drug transport; this is used for intravenous delivery. However, challenges persist, requiring stable conjugates with strong binding affinity, and the need to avoid modifying the drug's stability or binding affinity during delivery [61]. In vivo studies [21, 42, 43] demonstrate that only a few targeting agents can effectively cross the BBB to reach brain tissue, and systemic delivery often results in undesirable side effects in non-targeted tissues.
Particularly in GB treatment, the localised nature of the disease and the absence of distal metastases underscore the inherent risks of systemic radionuclide administration, such as off-target radiation exposure. Clinical evidence increasingly supports localised delivery methods like intratumoral or post-surgical cavity administration. These methods not only bypass the BBB but also target microscopic disease directly, overcoming the dilution effect typical of systemic administration. This approach aligns with the fact that GB does not typically metastasise, making localised delivery especially suitable. Clinical trials consistently utilise intratumoral and intracavitary delivery to maximise the efficacy of TAT agents and minimise systemic exposure.
Intratumoral and intracavitary methods involve direct injection, which provides localised TAT agent release, minimising systemic exposure. In the clinical studies, intratumoral and intracavitary delivery was implemented, and the biodistribution of the radiopharmaceutical was assessed using PET/CT [26, 30,31,32]. The local delivery of the TAT agents for the treatment of GB faces intricate challenges associated with the increased tissue pressure within tumours and adjacent tissues [26, 28, 30,31,32]. This elevated pressure diminishes the gradient that drives the diffusion process, resulting in a notable reduction in the absorbed dose by the peripheral areas of the treatment volume [30]. Tumour structural differences further complicate matters, highlighting the need for an understanding of tissue heterogeneity and variations in radiopharmaceutical diffusion. Apparent diffusion coefficient measurements derived from MRI examinations offer insights into diffusion variations within tumours, potentially influencing treatment responses [30]. Factors affecting successful locoregional therapy include molecular weight, physicochemical properties, extracellular space density, and the impact of repetitive injections on glial scarring [30]. The slow diffusion rate into swollen brain tissue poses a significant challenge, prompting exploration into convection-enhanced diffusion (CED) techniques [30, 62]. CED utilises a small hydraulic pressure that results in bulk/convection flow, enabling a homogeneous drug distribution directly into the adjacent brain [62].
Despite the progress, challenges persist in achieving effective drug delivery to the brain and overcoming the barriers imposed by the BBB and BTB. The complex interplay of biological processes necessitates further exploration and understanding for the successful implementation of local TAT in the treatment of GB, emphasising the importance of ongoing dosimetry studies and a nuanced approach to treatment protocols.
5 Limitations and Gaps in Literature
While the current literature on TAT for GB shows promise, several gaps and limitations necessitate further investigation and the optimisation of future clinical trials . Here are the limitations and gaps we identified:
-
i.
Radiation dose to susceptible organs: Systemically administered radionuclides pose a limitation due to the radiation dose reaching susceptible organs, including the liver, spleen, stomach and kidneys as seen in [20, 41,42,43]. Pre-clinical in vivo studies have indicated that intratumoral or local injection of the radionuclide is likely more effective and less toxic to healthy tissues [21, 42, 43].
-
ii.
Limited number of patients sampled: The clinical studies have been conducted on a very limited number of patients and have not been randomised to alternative available conventional therapies. Expanding the scope of studies to include a larger and more diverse patient population will provide a more comprehensive understanding of the therapy's efficacy and safety. These studies should also consider optimising patient inclusion criteria for further research and thus enable randomised studies.
-
iii.
Dosimetry studies: Additional dosimetry/radiobiological modelling studies are needed to better comprehend the complex biological processes involved in local radioisotope treatment of GB. These studies can give quantifiable evidence of TAT’s effectiveness in tumour cell kill, help refine treatment protocols, and optimise radiation dosages. Further dosimetry studies that quantify the radiation doses at the target site are crucial, considering factors such as the unique characteristics of the radiopharmaceutical, diffusion rates, and potential variations in individual tumour structures. Moreover, there is a significant need for cellular dosimetry studies to understand and predict the biological effects of alpha-particle radiopharmaceuticals. Dosimetry at the micro- or multi-cellular scale level can inform treatment optimisation and efficacy assessment by elucidating the radiation effects at the cellular level, which are critical for tailoring therapy to achieve maximum therapeutic benefit while minimising harm.
-
iv.
Microdosimetry models: The limited application of microdosimetric models highlights the importance of future studies in this area. Understanding radiation effects at the cellular level is critical for optimising treatment strategies.
-
v.
Intratumoral distribution: The challenge of achieving effective intratumoral distribution of alpha emitters, especially in larger tumours/volumes, needs further exploration. Using radioisotopes with longer half-lives such as Ac-225 may have an impact on this distribution issue and should be investigated in greater detail.
-
vi.
Mechanisms of action for TAT: Further research could delve into the mechanistic differences between TAT and other treatment modalities in terms of GB treatment. This would provide insights into the unique benefits and challenges associated with alpha-particle irradiation. Also, exploring its synergy with other treatment modalities such as external beam radiotherapy and chemotherapy could hold promise.
-
vii.
Delivery methods/diffusion of alpha-emitting agents: Innovative delivery methods for alpha-particle-emitting agents, especially considering their limited range, need to be explored. Additionally, looking at how to quantify the distribution of the agents after injection and predicate its path within treatment volume are important. Finding ways to ensure effective distribution within tumours is crucial.
-
viii.
Recoil effect of radionuclides: None of the reviewed studies have addressed the recoil effect, which is challenging to measure as it requires tracking daughter nuclides independently. This gap is critical as it could impact the stability and efficacy of radionuclide therapies. Recent simulation studies, such as those by Tronchin et al. [63], begin to address this by examining dosimetry from recoil daughter nuclides.
-
ix.
Factors affecting cytotoxicity: It is essential to explore the factors affecting the cytotoxicity of available alpha-emitting agents, comparing different radioisotopes and their potential clinical applications. This could lead to a more nuanced understanding of their therapeutic potential.
Overall, while TAT shows promise as a treatment for GB, addressing these identified gaps and optimising treatment protocols underpinned by further well designed preclinical and clinical studies are imperative for its successful application. TAT has significant potential to improve outcomes in a patient group with no material survival improvement over the last two decades and persistently remaining extremely low survival rates.
6 Review Limitations
It is important to recognise the limitations of this review. The search strategy was executed across diverse databases (MEDLINE, Embase and Scopus, supplemented by Google Scholar for grey literature), with papers published in non-English language and conference abstracts, posters and review articles excluded during the full-text review. Although the search strategy (Appendix A, Online Supplemental Material) was developed with aid of a UniSA librarian, it is acknowledged that these exclusions and limitations may have led to the oversight of some relevant articles.
7 Conclusion
TAT offers a promising avenue for treating GB, but its full potential hinges on overcoming significant challenges. Systemic administration of radionuclides raises concerns about radiation exposure to vulnerable adjacent normal tissues, advocating for localised delivery methods. Small patient samples in current studies necessitate larger and more diverse clinical trials to establish real-world effectiveness. Dosimetry studies and the investigation of local distribution methods are vital for refining dosing and enhancing treatment outcomes. Additionally, exploring the synergy of TAT with other novel therapies could hold promise.
References
WHO Classification of Tumours Editorial Board. World Health Organization Classification of Tumours of the Central Nervous System 5th ed. 5 ed. Lyon: Lyon: International Agency for Research on Cancer; 2021.
Grech N, Dalli T, Mizzi S, Meilak L, Calleja N, Zrinzo A. Rising incidence of glioblastoma multiforme in a well-defined population. Curēus. 2020;12(5):1–9.
Girardi F, Matz M, Stiller C, You H, Marcos Gragera R, Valkov MY, et al. Global survival trends for brain tumors, by histology: analysis of individual records for 556,237 adults diagnosed in 59 countries during 2000–2014 (CONCORD-3). Neuro Oncol. 2023;25(3):580–92.
Walker S, Busatto S, Pham A, Tian M, Suh A, Carson K, et al. Extracellular vesicle-based drug delivery systems for cancer treatment. Theranostics. 2019;9(26):8001–17.
Vollmann-Zwerenz A, Leidgens V, Feliciello G, Klein CA, Hau P. Tumor cell invasion in glioblastoma. Int J Mol Sci. 2020;21(6):1–21.
Yamahara T, Numa Y, Oishi T, Kawaguchi T, Seno T, Asai A, Kawamoto K. Morphological and flow cytometric analysis of cell infiltration in glioblastoma: a comparison of autopsy brain and neuroimaging. Brain Tumor Pathol. 2010;27(2):81–7.
Ahir BK, Engelhard HH, Lakka SS. Tumor development and angiogenesis in adult brain tumor: glioblastoma. Mol Neurobiol. 2020;57(5):2461–78.
Yalamarty SSK, Filipczak N, Li X, Subhan MA, Parveen F, Ataide JA, et al. Mechanisms of resistance and current treatment options for glioblastoma multiforme (GBM). Cancers (Basel). 2023;15(7):1–37.
Rodríguez-Camacho A, Flores-Vázquez JG, Moscardini-Martelli J, Torres-Ríos JA, Olmos-Guzmán A, Ortiz-Arce CS, et al. Glioblastoma treatment: state-of-the-art and future perspectives. Int J Mol Sci. 2022;23(13):1–35.
Poty S, Francesconi LC, McDevitt MR, Morris MJ, Lewis JS. α-emitters for radiotherapy: from basic radiochemistry to clinical studies—part 1. J Nucl Med. 2018;59(6):878–84.
Nishri Y, Vatarescu M, Luz I, Epstein L, Dumancic M, Del Mare S, et al. Diffusing alpha-emitters radiation therapy in combination with temozolomide or bevacizumab in human glioblastoma multiforme xenografts. Front Oncol. 2022;12(888100):1–15.
Cooks T, Tal M, Raab S, Efrati M, Reitkopf S, Lazarov E, et al. Intratumoral Ra-loaded wires spread alpha-emitters inside solid human tumors in athymic mice achieving tumor control. Anticancer Res. 2012;32(12):5315–21.
Yang K, Wu Z, Zhang H, Zhang N, Wu W, Wang Z, et al. Glioma targeted therapy: insight into future of molecular approaches. Mol Cancer. 2022;21(1):1–32.
Arazi L. Diffusing alpha-emitters radiation therapy: approximate modeling of the macroscopic alpha particle dose of a point source. Phys Med Biol. 2020;65(1):1–24.
Marcu L, Bezak E, Allen BJ. Global comparison of targeted alpha vs targeted beta therapy for cancer: In vitro, in vivo and clinical trials. Crit Rev Oncol Hematol. 2018;2018(123):7–20.
Pouget J-P, Lozza C, Deshayes E, Boudousq V, Navarro-Teulon I. Introduction to radiobiology of targeted radionuclide therapy. Front Med. 2015;2(12):1–11.
Bavelaar BM, Lee BQ, Gill MR, Falzone N, Vallis KA. Subcellular targeting of theranostic radionuclides. Front Pharmacol. 2018;9(996):1–17.
Sgouros G, Roeske JC, McDevitt MR, Palm S, Allen BJ, Fisher DR, et al. MIRD Pamphlet No 22 (abridged): radiobiology and dosimetry of alpha-particle emitters for targeted radionuclide therapy. J Nucl Med. 2010;51(2):311–28.
Page M, McKenzie J, Bossuyt P, Boutron I, Hoffmann T, Mulrow C, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372(71):1–9.
Behling K, Maguire WF, Di Gialleonardo V, Heeb LE, Hassan IF, Veach DR, et al. Remodeling the vascular microenvironment of glioblastoma with alpha-particles. J Nucl Med. 2016;57(11):1771–7.
Behling K, Maguire WF, Lopez Puebla JC, Sprinkle SR, Ruggiero A, O’Donoghue J, et al. Vascular targeted radioimmunotherapy for the treatment of glioblastoma. J Nucl Med. 2016;57(10):1576–82.
de Kruijff RM, van der Meer A, Windmeijer CAA, Kouwenberg JJM, Morgenstern A, Bruchertseifer F, et al. The therapeutic potential of polymersomes loaded with (225)Ac evaluated in 2D and 3D in vitro glioma models. Eur J Pharm Biopharm. 2018;127:85–91.
Sattiraju A, Xiong X, Pandya DN, Wadas TJ, Xuan A, Sun Y, et al. Alpha particle enhanced blood brain/tumor barrier permeabilization in glioblastomas using integrin alpha-v beta-3-targeted liposomes. Mol Cancer Ther. 2017;16(10):2191–200.
Sattiraju A, Solingapuram Sai KK, Xuan A, Pandya DN, Almaguel FG, Wadas TJ, et al. IL13RA2 targeted alpha particle therapy against glioblastomas. Oncotarget. 2017;8(26):42997–3007.
Majkowska-Pilip A, Rius M, Bruchertseifer F, Apostolidis C, Weis M, Bonelli M, et al. In vitro evaluation of (225) Ac-DOTA-substance P for targeted alpha therapy of glioblastoma multiforme. Chem Biol Drug Des. 2018;92(1):1344–56.
Krolicki L, Bruchertseifer F, Kunikowska J, Koziara H, Pawlak D, Kulinski R, et al. Dose escalation study of targeted alpha therapy with [(225)Ac]Ac-DOTA-substance P in recurrence glioblastoma - safety and efficacy. Eur J Nucl Med Mol Imaging. 2021;48(11):3595–605.
Bolcaen J, Kleynhans J, Nair S, Verhoeven J, Goethals I, Sathekge M, et al. A perspective on the radiopharmaceutical requirements for imaging and therapy of glioblastoma. Theranostics. 2021;11(16):7911–47.
Cordier D, Forrer F, Bruchertseifer F, Morgenstern A, Apostolidis C, Good S, et al. Targeted alpha-radionuclide therapy of functionally critically located gliomas with 213Bi-DOTA-[Thi8, Met(O2)11]-substance P: a pilot trial. Eur J Nucl Med Mol Imaging. 2010;37(7):1335–44.
Cordier D, Merlo A. Long-term results of targeted low-grade glioma treatment with (213)Bi-DOTA-[Thi(8), Met(O(2))(11)]-substance P. Cancer Biother Radiopharm. 2019;34(6):413–6.
Krolicki L, Kunikowska J, Bruchertseifer F, Kulinski R, Pawlak D, Koziara H, et al. Locoregional treatment of glioblastoma with targeted alpha therapy: [213 Bi]Bi-DOTA-substance P versus [225 Ac]Ac-DOTA-substance P-analysis of influence parameters. Clin Nucl Med. 2023;48(5):387–92.
Krolicki L, Bruchertseifer F, Kunikowska J, Koziara H, Krolicki B, Jakucinski M, et al. Prolonged survival in secondary glioblastoma following local injection of targeted alpha therapy with (213)Bi-substance P analogue. Eur J Nucl Med Mol Imaging. 2018;45(9):1636–44.
Krolicki L, Bruchertseifer F, Kunikowska J, Koziara H, Krolicki B, Jakucinski M, et al. Safety and efficacy of targeted alpha therapy with (213)Bi-DOTA-substance P in recurrent glioblastoma. Eur J Nucl Med Mol Imaging. 2019;46(3):614–22.
Feuerecker B, Biechl P, Seidl C, Bruchertseifer F, Morgenstern A, Schwaiger M, Eisenreich W. Diverse metabolic response of cancer cells treated with a (213)Bi-anti-EGFR-immunoconjugate. Sci Rep. 2021;11(1):6227.
Zalutsky MR, Reardon DA, Akabani G, Coleman RE, Friedman AH, Friedman HS, et al. Clinical experience with alpha-particle emitting 211At: treatment of recurrent brain tumor patients with 211At-labeled chimeric antitenascin monoclonal antibody 81C6. J Nucl Med. 2008;49(1):30–8.
Larsen RH, Akabani G, Welsh P, Zalutsky MR. The cytotoxicity and microdosimetry of astatine-211-labeled chimeric monoclonal antibodies in human glioma and melanoma cells in vitro. Radiat Res. 1998;149:2.
Larsen RH, Vaidyanathan G, Zalutsky MR. Cytotoxicity of alpha-particle-emitting 5-[211At]astato-2’-deoxyuridine in human cancer cells. Int J Radiat Biol. 1997;72(1):79–90.
Rosenkranz AA, Vaidyanathan G, Pozzi OR, Lunin VG, Zalutsky MR, Sobolev AS. Engineered modular recombinant transporters: application of new platform for targeted radiotherapeutic agents to alpha-particle emitting 211 At. Int J Radiat Oncol Biol Phys. 2008;72(1):193–200.
Carlin S, Akabani G, Zalutsky M. In vitro cytotoxicity of 211At-astatide and 131i-iodide to glioma tumor cells expressing the sodium/iodide symporter. PubMed. 2003;44(11):1827–38.
Zalutsky MR, Garg PK, Friedman HS, Bigner DD. Labeling monoclonal antibodies and F(ab’)2 fragments with the a-particle-emitting nuclide astatine-211: preservation of immunoreactivity and in vivo localizing capacity. Proc NatI Acad Sci USA. 1989;86:7149–53.
Carlin S, Mairs RJ, Welsh P, Zalutsky MR. Sodium-iodide symporter (NIS)-mediated accumulation of [(211)At]astatide in NIS-transfected human cancer cells. Nucl Med Biol. 2002;29(7):729–39.
Zalutsky MR, Stabin MG, Larsen RH, Bigner DD. Tissue distribution and radiation dosimetry of astatine-211-labeled chimeric 81C6, an alpha-particle-emitting immunoconjugate. Nucl Med Biol. 1997;24(3):255–61.
Ma H, Li F, Shen G, Pan L, Liu W, Liang R, et al. In vitro and in vivo evaluation of (211)At-labeled fibroblast activation protein inhibitor for glioma treatment. Bioorg Med Chem. 2022;55(116600):1–8.
Liu W, Ma H, Liang R, Chen X, Li H, Lan T, et al. Targeted alpha therapy of glioma using (211)At-labeled heterodimeric peptide targeting both VEGFR and integrins. Mol Pharm. 2022;19(9):3206–16.
Borrmann N, Friedrich S, Schwabe K, Hedrich HJ, Krauss JK, Knapp WH, et al. Systemic treatment with 4–211Atphenylalanine enhances survival of rats with intracranial glioblastoma. Nuklearmedizin. 2013;52(6):212–21.
Watabe T, Kaneda-Nakashima K, Shirakami Y, Liu Y, Ooe K, Teramoto T, et al. Targeted alpha therapy using astatine ((211)At)-labeled phenylalanine: a preclinical study in glioma bearing mice. Oncotarget. 2020;11(15):1388–98.
Dabagian H, Taghvaee T, Martorano P, Martinez D, Samanta M, Watkins CM, et al. PARP targeted alpha-particle therapy enhances response to PD-1 immune-checkpoint blockade in a syngeneic mouse model of glioblastoma. ACS Pharmacol Transl Sci. 2021;4(1):344–51.
Schneeweiss FHS, R N; Brown, I. 211At-a-dose dependence of poly-ADP-ribosylation of human glioblastoma cells in vitro. Strahlenther Onkol. 1999;175(9):458-61.
Barazzuol L, Jena R, Burnet NG, Jeynes JC, Merchant MJ, Kirkby KJ, Kirkby NF. In vitro evaluation of combined temozolomide and radiotherapy using X rays and high-linear energy transfer radiation for glioblastoma. Radiat Res. 2012;177(5):651–62.
(IAEA) IAEA. Guidance for Preclinical Studies with Radiopharmaceuticals. 1 ed. Vienna: International Atomic Energy Agency; 2023.
Takahashi A, Ohnishi K, Tsuji K, Matsumoto H, Aoki H, Wang X, et al. WAF1 accumulation by carbon-ion beam and alpha-particle irradiation in human glioblastoma cultured cells. Int J Radiat Biol. 2000;76(3):335–41.
Wank M, Schilling D, Reindl J, Meyer B, Gempt J, Motov S, et al. Evaluation of radiation-related invasion in primary patient-derived glioma cells and validation with established cell lines: impact of different radiation qualities with differing LET. J Neurooncol. 2018;139(3):583–90.
Nishri Y, Vatarescu M, Luz I, Epstein L, Dumančić M, Del Mare S, et al. Diffusing alpha-emitters radiation therapy in combination with temozolomide or bevacizumab in human glioblastoma multiforme xenografts. Front Oncol. 2022;12(888100):1–15.
Dejaegher J, De Vleeschouwer S. Recurring glioblastoma: a case for reoperation? Glioblastoma. Australia: Australia: Exon Publications; 2017. p. 281-96.
Smith K, Nakaji P, Thomas T, Pinnaduwage D, Wallstrom G, Choi M, et al. Safety and patterns of survivorship in recurrent GBM following resection and surgically targeted radiation therapy: results from a prospective trial. Neuro Oncol. 2022;24(6):S4–15.
Stupp R, Wong ET, Kanner AA, Steinberg D, Engelhard H, Heidecke V, et al. NovoTTF-100A versus physician’s choice chemotherapy in recurrent glioblastoma: A randomised phase III trial of a novel treatment modality. Eur J Cancer. 2012;48(14):2192–202.
Tsien C, Pugh S, Dicker a, Raizer J, Matuszak M, Lallana E, et al. ACTR-32. NRG ONCOLOGY RTOG 1205: RANDOMIZED PHASE II TRIAL OF CONCURRENT BEVACIZUMAB AND RE-IRRADIATION VS. BEVACIZUMAB ALONE AS TREATMENT FOR RECURRENT GLIOBLASTOMA. Neuro-oncology. 2019;21(6):20.
Shi W, Scannell Bryan M, Gilbert MR, Mehta MP, Blumenthal DT, Brown PD, et al. Investigating the effect of reirradiation or systemic therapy in patients with glioblastoma after tumor progression: a secondary analysis of nrg oncology/radiation therapy oncology group trial 0525. Int J Radiat Oncol Biol Phys. 2018;100(1):38–44.
Mandl ESMD, Dirven CMFMDP, Buis DRM, Postma TJMDP, Vandertop WPMDP. Repeated surgery for glioblastoma multiforme: only in combination with other salvage therapy. Surg Neurol. 2008;69(5):506-9.
Wu D, Chen Q, Chen X, Han F, Chen Z, Wang Y. The blood–brain barrier: structure, regulation, and drug delivery. Signal Transduct Target Ther. 2023;8(1):1–27.
Arvanitis CD, Ferraro GB, Jain RK. The blood–brain barrier and blood–tumour barrier in brain tumours and metastases. Nat Rev Cancer. 2020;20(1):26–41.
Upton DH, Ung C, George SM, Tsoli M, Kavallaris M, Ziegler DS. Challenges and opportunities to penetrate the blood-brain barrier for brain cancer therapy. Theranostics. 2022;12(10):4734–52.
Naidoo J, Fiandaca M, Lonser RR, Bankiewicz K. Convection-Enhanced Drug Delivery in the Central Nervous System. 2019;335–50.
Tronchin S, Forster J, Hickson K, Bezak E. Modeling the effect of daughter migration on dosimetry estimates for unlabeled actinium-225. Medical Physics. 2024.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions. M.E. was funded through the Australian Government Research Training Program Scholarship.
Conflicts of Interest/Competing Interests
Maram El Sabri, Leyla Moghaddasi, Puthenparampil Wilson, Frank Saran, and Eva Bezak declare that they have no conflicts of interest that might be relevant to the contents of this article.
Ethics Approval
This review did not require ethics approval as it is a literature review and does not involve any new studies of human or animal subjects.
Consent to Participate
Not applicable.
Consent for Publication
All authors consent to the publication of this article.
Availability of Data and Material
No datasets were generated or analysed during the current study.
Code Availability
Not applicable.
Author Contributions
E.B. proposed the review topic; M.E. and E.B. screened the abstracts and full-text, M.E. interpreted the findings and drafted the article; E.B., P.W., F.S. and L.M. revised and edited the manuscript. All authors have read and agreed to the published version of the manuscript.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Sabri, M.E., Moghaddasi, L., Wilson, P. et al. Targeted Alpha Therapy for Glioblastoma: Review on In Vitro, In Vivo and Clinical Trials. Targ Oncol 19, 511–531 (2024). https://doi.org/10.1007/s11523-024-01071-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11523-024-01071-y