
Abstract
Introduction
Hemodialysis (HD) patients are at increased risk of severe COVID-19 infection but infection rates vary. Our objectives are to describe COVID-19 positive HD patients’ characteristics, infection rates, and factors associated with mortality in HD COVID-19 cases in Kuwait.
Methods
Data on demographics, comorbidities, and treatments received, as well as mortality for HD patients admitted to hospitals for COVID-19, from 1/March to 31/July 2020, prospectively collected and analyzed.
Results
A total of 141 infected HD patients were admitted (Mean age 58 ± 16.1; Males 56%), representing 7% of the total HD population and 0.2% of all COVID-19 cases during the study period. Of those 141 infected HD patients, 27 (19%) died, and this represents 6% of total COVID-19-related mortality and 27% of the total HD mortality. In contrast, total covid-19-related mortality of all positive cases was only 0.7%, and total HD mortality during the study period was only 5%. COVID-19-positive HD patients who died were older and 59% were males. However, the differences were not statistically significant. Of the 61 infected HD patients who needed to be switched to continuous kidney replacement therapy (CKRT), 34% died, and of the 29 infected HD patients who needed admission to intensive care, 65% died.
Conclusion
HD population represents a small fraction of the total population; however, positive HD COVID-19 cases represent a sizable proportion of COVID-19 cases and a significant percentage of total COVID-19-related mortality, and total HD mortality.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
A novel coronavirus leading to severe respiratory infection (coronavirus disease 2019, COVID-19) was first identified in Wuhan, China in December 2019 [1]. It was identified as the seventh coronavirus that could infect humans and was named severe acute respiratory syndrome—Coronavirus 2 (SARS-CoV-2) [2]. COVID-19 infection was declared a pandemic by the World Health Organization (WHO) due to its high rate of transmission, on 11 March 2020 [3]. As of the end of November 2021, more than 260 million people had been infected and more than 5,200,000 died worldwide [4]. WHO have defined severe disease as “a patient with severe acute respiratory illness (fever and at least one sign/symptom of respiratory disease, e.g., cough, shortness of breath; AND requiring hospitalization)” [5]. One report from the United States showed that about 70% of patients with comorbidities infected with COVID-19 required hospital admission and more than 90% of deaths were in patients with underlying conditions [6]. Multiple reports from different countries listed some risk factors for severe COVID-19 infection that include advanced age and comorbidities, such as diabetes mellitus (DM), cardiovascular disease (CVD), and hypertension (HTN) [7, 8]. Data from the Global Burden of Disease (GBD) collaboration, using 2017 prevalence data and UN population estimates for 2020, have estimated the global population at high risk for severe COVID-19 to be 1.7 billion people, comprising 22% of the global population, of whom 349 million would require hospital admission if infected. This study found that CKD was the most prevalent risk factor for severe COVID-19 worldwide [9].
Hemodialysis (HD) patients are at higher risk of infections including COVID-19 due to compromised immune status from uremia, metabolic derangement, inflammation, oxidative stress, and intestinal dysbiosis [7, 10]. Moreover, HD patients have to visit the dialysis center for HD thrice weekly, which means they cannot adhere to the stay-home policy and cannot avoid close contact with other people [7]. The first report from China on COVID-19 and HD showed that 42 patients out of 230 were infected, and 13 of the 42 died (5.65% of the total HD population) [11]. Results from the European renal association – European dialysis and transplantation association (ERA-EDTA) registry earlier in the pandemic, between Feb 1st to April 30th, 2020, indicate a high mortality due to COVID-19 in dialysis patients reaching 21% [12]. Another report from US facilities showed a 25% COVID-19 mortality rate where older age, heart disease, and markers of frailty were highly associated with mortality [13]. To prevent the spread of infection in HD centers, the nephrology community in Kuwait has implemented the recommendations published in international guidelines [14,15,16,17]. The objectives of this multi-center prospective study are to describe the status of COVID-19 infection in HD patients, the characteristics of such patients, and factors associated with increased mortality in HD covid-19 patients in Kuwait.
Methods
In the first wave of COVID-19 infection in Kuwait, from March 1, 2020, to July 31, 2020, the Ministry of Health (MoH) policy was to admit all COVID-19 positive cases to public hospitals, regardless of the severity of the infection, and treat for free. MoH HD centers serve 95% of the HD population, and 100% of the peritoneal dialysis (PD) population. The remaining 5% of the HD population receive HD in the private sector. Such patients were transferred to and treated in MoH hospitals in the event of contracting COVID-19 infection. Asymptomatic patients were tested based on a history of contact with positive cases. Patients were discharged only when they were asymptomatic and PCR negative for SARS-CoV-2 as per MoH policy. Once a dialysis patient is admitted to a hospital due to COVID-19 infection, we started to collect data on demographics and comorbidities. Patients then were followed while inpatient prospectively for up to four weeks (or less if discharged or died earlier) to record treatments received and other data in case of death. All HD patients above the age of 18 admitted to MoH hospitals with COVID-19 infection were enrolled. We had no exclusion criteria, and we had no refusal to consent. Data were collected from six general MoH hospitals with nephrology service that includes HD treatment. The MoH prospectively collected COVID-19 infection rates and mortality rates in the country and reported results daily. We compared our results to the rates reported by MoH for the entire population. We also looked at the percentage of COVID-19-related mortality to the total mortality in the HD population during the study period. We also looked at mortality rates at 6 months post-infection for those who survived the acute event. The study protocol was approved by the Joint Ministry of Health and the Kuwait University Committee on Medical Research, and all recruited patients consented to study entry before starting data collection.
The data analysis was performed using the statistical software Stata16 (StataCorp, College Station, TX, USA). The data were summarized using descriptive statistics in the form of mean/SD for continuous variables and number/percentage for categorical variables. The 95% CI was obtained using the exact method. Chi-square test was performed to compare the mortality in covid-19 and non-covid-19 HD patients. The univariable binary logistic regression with a robust estimator was applied to find the association of patient characteristics with mortality in Covid-19 positive patients on HD. The p < 0.2 in univariable logistic regression was included in the multivariable logistic model with a robust estimator. A p value less than 0.05 was considered as significant.
Results
Total COVID-19 cases in the general and the dialysis population
The total number of COVID-19 positive cases confirmed by PCR from a nasopharyngeal swab from March 1, 2020, to July 31, 2020, was 66,957 [18]. (less than 1.5% of the total population of 4,600,000 or 146 per 10,000 of population) [19]. The total number of HD patients infected with COVID-19 was 141 (7% of the total HD population in 2000 and 0.2% of the total number of confirmed COVID-19 cases) (Table 1).
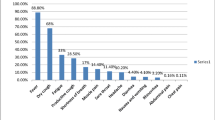
The mean age for HD patients with COVID-19 was 58 ± 16.1 (males 54.0 ± 17.5 were significantly younger than females 62.0 ± 13.2; p = 0.002). HTN, DM, heart disease, and chronic respiratory illness were present in 93%, 67%, 49%, 16%, respectively.
Steroids were given to 21% of patients, and hydroxychloroquine to 5%. Intensive care unit (ICU) admission was required for 20.6% of the HD patients, with 80% of those requiring mechanical ventilation (Table 1). Conventional HD was switched to continuous kidney replacement therapy (CKRT) in 61 patients (34%). The number of admitted patients who were on CKRT exceeds the number of patients admitted to ICU because many hemodynamically stable patients in the general medical wards were put on CKRT due to a lack of access to dialysate water in the inpatient wards in many MoH hospitals.
Outcomes
The total number of deaths due to COVID-19 infection in Kuwait during the study period was 447 (0.67% of the total number of positive cases) [18]. The total mortality in the HD population during that period regardless of the cause was 100 (5% of the total HD population), however, mortality due to COVID-19 infection in HD patients was 27% of the total mortality in the HD population, 6% of the total COVID-19 related mortality in the country, and 19% of the total HD COVID-19 positive cases. The mortality was significantly higher in covid-19 HD patients than in non-covid-19 patients 19.1% vs 3.9% OR = 5.80 [95% CI 3.58–9.37; p < 0.001].
HD Patients who died from COVID-19 were older with a mean age of 62.9 ± 12.1 vs 56.9 ± 15.2 for HD patients who survived but the mean difference between them was not statistically significant p = 0.058. HD patients who died also had respiratory illness more frequently (25% vs 14%) and 59% were males. Of the 61 patients who were switched to CKRT, 34% died. Of the 29 HD patients admitted to ICU, 65% died. Of those who died, 95% were on assisted ventilation, and 63% received corticosteroids. Except for age, no other factor was significantly associated with mortality in covid-19 HD patients in univariable logistic regression with a robust variance estimator. Linearity of age in the logit scale was checked by adding a square term in the model (Table 2). Multivariable logistic regression considered the factors that had p < 0.2 in univariable analysis with a robust estimator, effect of age also became insignificant between the survivors and non-survivors (Table 2).
A 6-months follow-up on HD patients who survived COVID-19 revealed that 16.7% of the 114-survivor died, five remained Oxygen dependent, and the rest recovered completely.
There were an additional seven PD patients who contracted the virus during the same period, representing 3% of the total PD population and 4.8% of the dialysis patients infected with SARS-CoV-2. Although the total number of COVID-19 positive PD patients was low, mortality in COVID-19 positive PD cases approached 43%, much higher than the mortality rate in COVID-19 HD patients (19%). PD Patients who died from the infection were older with a mean age of 62.6 vs 49.5 for survivors.
Discussion
Reported SARS-CoV-2 infection and mortality rates in the HD population are variable, [8, 9, 12, 13]. partly because early reports failed to adequately assess chronic kidney disease (CKD) prevalence and its impact on COVID-19 disease severity and instead focused on CKD-associated conditions (CVD, HTN, and DM) [20]. Reports were also influenced by sample sizes and the use of in-hospital populations groups of severely ill patients with an estimated risk that may not be generalizable to the broader kidney replacement therapy (KRT) population [12]. However, CKD and especially dialysis, is a common and strong risk factor for both infection and mortality [8, 9]. Studies from China, Europe, and North America reported higher mortality and more severe disease in HD patients compared to the general population [21,22,23,24,25,26,27,28,29].
COVID-19 infection rates in the dialysis population varied from 2.2 [22] to 19.6%, [25] with our study reporting a rate of 7%, and mortality rates varied from 16.2 [30] to 52%, [31] while our rate was 19%. Both rates are much higher than the general population in these reports and in our cohort. Dialysis patients also had a shorter time from symptom onset to ICU admission compared to other groups [32].
Our study confirms findings in other reports that infection and mortality rates in HD patients are higher than in the general population. Important risk factors for mortality in dialysis patients include older age and male gender [12, 13]. Although non-survivors in our HD population were older, mainly male, and had more comorbidities than survivors, differences were not statistically significant.
There is a paucity in the medical literature when it comes to COVID-19 infection and chronic PD patients. European data showed that PD patients represented 4% of total dialysis patients infected with COVID-19 (31 of 768 patients) and 5% of the total mortality in that group (29% of the infected PD group) [33]. A paper analyzing a single center experience reported that out of the total hospitalized dialysis population with the infection, 2.6% were PD patients (11 patients), with an 18% mortality rate in the PD group infected with the virus [34]. Another paper, again analyzing a single center experience reported a 3.4% PD share (2 patients) with no deaths [27]. A Canadian study reported a 1.8% infection rate in the entire in-center HD population for the province of Ontario versus 0.8% in the PD population [35]. PD patients represented 4.8% of the total infected dialysis patients, and 3% of the total PD population, and had a much higher death rate (~ 43%).
With regard to pharmacological treatment of COVID-19; corticosteroids, remdesivir, and tocilizumab have clinical benefits, but hydroxychloroquine and lopinavir-ritonavir combination are ineffective [36]. Steroids were used in only 21% of our HD patients, and the other medications were used in an even much lower proportion. Steroids were thought to be effective in cases with severe COVID-19-associated pneumonia followed by tocilizumab which was an off-label use at that time, but its use was restricted to ICU patients who met certain criteria as per the MoH policy at that time. Therefore, it is hard to draw any conclusion on the effect of such therapies on HD patients with COVID-19.
Unfortunately, the medical literature on the issue of the long-term impact of COVID-19 infection in the dialysis population was scarce. This study shed light on the impact of COVID-19 in dialysis patients with results that clearly show the associated increased morbidity and mortality. Such data is crucial to help policymakers and directors of hemodialysis centers in formulating more effective strategies to protect vulnerable patients with comorbidities and reduce pressure on health care systems.
Strengths and limitations
Our study aimed for complete national coverage, eliminating sampling bias found in smaller and non–population-based studies. However, lack of testing of positive cases (lack of symptoms, refusal of testing, or not reporting to the dialysis center), may have led to an overestimation of mortality, albeit small. Identifying at-risk populations is important for the design of effective interventions that aim to reduce the risk of transmission to vulnerable patients like in the dialysis population. Since we do not have complete clinical data for all the HD patients thus comparison was not done between the COVID-19 HD and non-COVID-19 HD patients.
Conclusion
Despite the fact the HD population represents only a small fraction of the total population, they represent a sizable proportion of the total COVID-19 positive cases and a significant percentage of the total COVID-19 related mortality. This study highlights the increased susceptibility of the HD population to COVID-19 infection, which is associated with a high rate of mortality in Kuwait, although lower than mortality rates reported in Europe and the United States. It also highlights the importance of adherence to screening, prevention, and isolation policies to reduce the spread of infection and save lives. It also lends support to the calls worldwide to give dialysis patients priority to receive the COVID-19 vaccine.
Availability of data and materials
Data can be provided by the corresponding author in case of a reasonable request. This is not a clinical trial.
References
Lu H, Stratton CW, Tang YW (2020) Outbreak of pneumonia of unknown etiology in Wuhan, China: the mystery and the miracle. J Med Virol 92(4):401–402. https://doi.org/10.1002/jmv.25678
Gorbalenya AE, Baker SC et al (2020) for the Coronaviridae Study Group of the International Committee on Taxonomy of Viruses. The species Severe acute respiratory syndrome-related coronavirus: classifying 2019-nCoV and naming it SARS-CoV-2. Nat Microbiol 5:536–544. https://doi.org/10.1038/s41564-020-0695-z
-World Health Organization. Listings of WHO’s response to COVID-19: https://www.who.int/news/item/29-06-2020-covidtimeline. Last accessed October/2020
-Johns Hopkins University of Medicine Coronavirus Resource Center: https://coronavirus.jhu.edu/map.html. Last accessed October/2020
- Global Surveillance for human infection with coronavirus disease (COVID-19) WHO. https://www.who.int/publications-detail/global-surveillance-for-human-infection-with-novel-coronavirus-(2019-ncov). (March 20, 2020), Accessed 8th Jun 2020
Preliminary estimates of the prevalence of selected underlying health conditions among patients with coronavirus disease 2019—United States, Centers for Disease Control and Prevention. February 12–March 28, 2020 CDC COVID-19 Response Team MMWR Morb Mortal Wkly Rep, 69 (2020), pp 382–386
Ikizler TA (2020) COVID-19 and dialysis units: What do we know now and what should we do? Am J Kidney Dis 76(1):1–3. https://doi.org/10.1053/j.ajkd.2020.03.008
Williamson EJ, Walker AJ, Bhaskaran K, Bacon S, Bates C, Morton CE, Curtis HJ, Mehrkar A, Evans D, Inglesby P, Cockburn J, McDonald HI, MacKenna B, Tomlinson L, Douglas IJ, Rentsch CT, Mathur R, Wong AYS, Grieve R, Harrison D, Forbes H, Schultze A, Croker R, Parry J, Hester F, Harper S, Perera R, Evans SJW, Smeeth L, Goldacre B (2020) Factors associated with COVID-19-related death using OpenSAFELY. Nature 584(7821):430–436. https://doi.org/10.1038/s41586-020-2521-4
Clark A, Jit M, Warren-Gash C, Guthrie B, Wang HHX, Mercer SW, Sanderson C, McKee M, Troeger C, Ong KL, Checchi F, Perel P, Joseph S, Gibbs HP, Banerjee A, Eggo RM, Centre for the Mathematical Modelling of Infectious Diseases COVID-19 working group (2020) Global, regional, and national estimates of the population at increased risk of severe COVID-19 due to underlying health conditions in 2020: a modelling study. Lancet Glob Health 8(8):e1003–e1017. https://doi.org/10.1016/S2214-109X(20)30264-3
Syed-Ahmed M, Narayanan M (2019) Immune dysfunction and risk of infection in chronic kidney disease. Adv Chronic Kidney Dis 26(1):8–15
Ma Y, Diao B, Lv X, Liang W, Zhu J, Liu L, Zhang S, Shen B, Wang H (2020) COVID-19 in hemodialysis (HD) patients: Report from one HD center in Wuhan, China. medRxiv. https://doi.org/10.1101/2020.02.24.20027201
Jager KJ, Kramer A, Chesnaye NC, Couchoud C, Sánchez-Álvarez JE, Garneata L, Collart F, Hemmelder MH, Ambühl P, Kerschbaum J, Legeai C, Del Pino Y Pino MD, Mircescu G, Mazzoleni L, Hoekstra T, Winzeler R, Mayer G, Stel VS, Wanner C, Zoccali C, Massy ZA (2020) Results from the ERA-EDTA Registry indicate a high mortality due to COVID-19 in dialysis patients and kidney transplant recipients across Europe. Kidney Int 98(6):1540–1548. https://doi.org/10.1016/j.kint.2020.09.006
Hsu CM, Weiner DE, Aweh G, Miskulin DC, Manley HJ, Stewart C, Ladik V, Hosford J, Lacson EC, Johnson DS, Lacson E Jr (2021) COVID-19 Among US dialysis patients: risk factors and outcomes from a national dialysis provider. Am J Kidney Dis 77(5):748–756. https://doi.org/10.1053/j.ajkd.2021.01.003 (e1; Epub 2021 Jan 17)
International Society of Nephrology Website. Recommendations for prevention and treatment of COVID-19. https://www.theisn.org/covid19/recommendations. Last accessed October/2020
Centers for Disease Control and Prevention Website. COVID-19 infection control guidance. https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-recommendations.html. Last accessed October/2020.
Basile C, Combe C, Pizzarelli F, Covic A, Davenport A, Kanbay M, Kirmizis D, Schneditz D, van der Sande F, Mitra S (2020) Recommendations for the prevention, mitigation and containment of the emerging SARS-CoV-2 (COVID-19) pandemic in haemodialysis centres. Nephrol Dial Transplant 35(5):737–741. https://doi.org/10.1093/ndt/gfaa069
American Society of Nephrology Website. Information for Screening and Management of COVID-19 in the Outpatient Dialysis Facility. https://www.asn-online.org/g/blast/files/DIALYSIS_COVID_2019_Update_03.13.2020_FINAL.pdf. Last accessed October/2020.
Ministry of Health of Kuwait Twitter Account. https://twitter.com/kuwait_moh. Last Accessed August/2020.
Public Authority for Civil Information (Kuwait). Population and labor market indicators: https://www.paci.gov.kw/stat/StatIndicators.aspx. Last Accessed August/2020.
ERA-EDTA Council, ERACODA Working Group (2021) Chronic kidney disease is a key risk factor for severe COVID-19: a call to action by the ERA-EDTA. Nephrol Dial Transplant 36(1):87–94. https://doi.org/10.1093/ndt/gfaa314
Henry BM, Lippi G (2020) Chronic kidney disease is associated with severe coronavirus disease 2019 (COVID-19) infection. Int Urol Nephrol 52(6):1193–1194. https://doi.org/10.1007/s11255-020-02451-9
Xiong F, Tang H, Liu L, Tu C, Tian JB, Lei CT, Liu J, Dong JW, Chen WL, Wang XH, Luo D, Shi M, Miao XP, Zhang C (2020) Clinical characteristics of and medical interventions for COVID-19 in hemodialysis patients in Wuhan, China. J Am Soc Nephrol 31(7):1387–1397. https://doi.org/10.1681/ASN.2020030354
Alberici F, Delbarba E, Manenti C, Econimo L, Valerio F, Pola A, Maffei C, Possenti S, Lucca B, Cortinovis R, Terlizzi V, Zappa M, Saccà C, Pezzini E, Calcaterra E, Piarulli P, Guerini A, Boni F, Gallico A, Mucchetti A, Affatato S, Bove S, Bracchi M, Costantino EM, Zubani R, Camerini C, Gaggia P, Movilli E, Bossini N, Gaggiotti M, Scolari F (2020) A report from the Brescia Renal COVID Task Force on the clinical characteristics and short-term outcome of hemodialysis patients with SARS-CoV-2 infection. Kidney Int 98(1):20–26. https://doi.org/10.1016/j.kint.2020.04.030
Tang H, Tian JB, Dong JW, Tang XT, Yan ZY, Zhao YY, Xiong F, Sun X, Song CX, Xiang CG, Tu C, Lei CT, Liu J, Su H, Huang J, Qiu Y, Miao XP, Zhang C (2020) Serologic detection of SARS-CoV-2 infections in hemodialysis centers: a multicenter retrospective study in Wuhan, China. Am J Kidney Dis 76(4):490–499. https://doi.org/10.1053/j.ajkd.2020.06.008 (e1)
Corbett RW, Blakey S, Nitsch D, Loucaidou M, McLean A, Duncan N, Ashby DR, West London Renal and Transplant Centre (2020) Epidemiology of COVID-19 in an Urban Dialysis Center. J Am Soc Nephrol 31(8):1815–1823. https://doi.org/10.1681/ASN.2020040534
Weiss S, Bhat P, Del Pilar Fernandez M, Bhat JG, Coritsidis GN (2020) COVID-19 Infection in ESKD: findings from a prospective disease surveillance program at dialysis facilities in New York City and Long Island. J Am Soc Nephrol JASN 31(11):2517–2521. https://doi.org/10.1681/ASN.2020070932
Valeri AM, Robbins-Juarez SY, Stevens JS, Ahn W, Rao MK, Radhakrishnan J, Gharavi AG, Mohan S, Husain SA (2020) Presentation and outcomes of patients with ESKD and COVID-19. J Am Soc Nephrol JASN 31(7):1409–1415. https://doi.org/10.1681/ASN.2020040470
Sim JJ, Huang CW, Selevan DC, Chung J, Rutkowski MP, Zhou H (2021) COVID-19 and survival in maintenance dialysis. Kidney Med. 3(1):132–135. https://doi.org/10.1016/j.xkme.2020.11.005
Ng JH, Hirsch JS, Wanchoo R, Sachdeva M, Sakhiya V, Hong S, Jhaveri KD, Fishbane S, Northwell COVID-19 Research Consortium and the Northwell Nephrology COVID-19 Research Consortium (2020) Outcomes of patients with end-stage kidney disease hospitalized with COVID-19. Kidney Int 98(6):1530–1539. https://doi.org/10.1016/j.kint.2020.07.030
COVID-19 Task Force Committee of the Japanese Association of Dialysis Physicians; Japanese Society for Dialysis Therapy; Japanese Society of Nephrology, Kikuchi K, Nangaku M, Ryuzaki M, Yamakawa T, Hanafusa N, Sakai K, Kanno Y, Ando R, Shinoda T, Nakamoto H, Akizawa T (2020) COVID-19 of dialysis patients in Japan: current status and guidance on preventive measures. Ther Apher Dial 24(4):361–365. https://doi.org/10.1111/1744-9987.13531
La Milia V, Bacchini G, Bigi MC, Casartelli D, Cavalli A, Corti M, Crepaldi M, Limardo M, Longhi S, Manzoni C, Ravasi C, Stucchi V, Viganò S (2020) COVID-19 outbreak in a large hemodialysis center in Lombardy. Italy Kidney Int Rep 5(7):1095–1099. https://doi.org/10.1016/j.ekir.2020.05.019
Flythe JE, Assimon MM, Tugman MJ, Chang EH, Gupta S, Shah J, Sosa MA, Renaghan AD, Melamed ML, Wilson FP, Neyra JA, Rashidi A, Boyle SM, Anand S, Christov M, Thomas LF, Edmonston D, Leaf DE, STOP-COVID Investigators (2021) Characteristics and outcomes of individuals with pre-existing kidney disease and COVID-19 admitted to intensive care units in the United States. Am J Kidney Dis 77(2):190–203. https://doi.org/10.1053/j.ajkd.2020.09.003 (e1)
Hilbrands LB, Duivenvoorden R, Vart P, Franssen CFM, Hemmelder MH, Jager KJ, Kieneker LM, Noordzij M, Pena MJ, Vries H, Arroyo D, Covic A, Crespo M, Goffin E, Islam M, Massy ZA, Montero N, Oliveira JP, Roca Muñoz A, Sanchez JE, Sridharan S, Winzeler R, ERACODA Collaborators (2020) Gansevoort RT COVID-19-related mortality in kidney transplant and dialysis patients: results of the ERACODA collaboration. Nephrol Dial Transplant 35(11):1973–1983. https://doi.org/10.1093/ndt/gfaa261
Sachdeva M, Uppal NN, Hirsch JS, Ng JH, Malieckal D, Fishbane S, Jhaveri KD (2020) COVID-19 in hospitalized patients on chronic peritoneal dialysis: a case series. Am J Nephrol 51:669–674. https://doi.org/10.1159/000510259
Taji L, Thomas D, Oliver MJ, Ip J, Tang Y, Yeung A, Cooper R, House AA, McFarlane P, Blake PG (2021) COVID-19 in patients undergoing long-term dialysis in Ontario. CMAJ 193(8):E278–E284. https://doi.org/10.1503/cmaj.202601
- Kim AY, Gandhi RT (2020) COVID-19: management in hospitalized adults. In: UpToDate, Post, TW (Eds), UpToDate, Waltham, MA. https://www.uptodate.com/login
Funding
Not funded.
Author information
Authors and Affiliations
Contributions
Research idea and study design: AAS, AAQ, AAY, YB, BAH, HAR. Data acquisition: AAS, AAQ, HB, AAY, YB, BAH, HAR, AAM, HS, ME, ME, EA, MA, AAT, MAS, AAA, RK. Data analysis/interpretation/statistical analysis: AAS, AAQ, HB, AAY, YB, BAH, HAR, AAM, RK. Supervision or mentorship: AAS, AAQ, AAY, YB, BAH, HAR. Manuscript writing and revision: AAS, AAQ, HB, AAY, YB, BAH, HAR, AAM, HS, ME, ME, EA, MA, AAT, MAS, AAA, RK. All authors take responsibility that this study has been reported honestly, accurately and transparently, and accepts accountability for the overall work by ensuring that questions pertaining to the accuracy or integrity of any portion of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
Approved by joint committee on medical and scientific research.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
AlSahow, A., AlQallaf, A., AlYousef, A. et al. Impact of COVID-19 infection on the dialysis population prospective, observational, nationwide study. Int Urol Nephrol 55, 721–727 (2023). https://doi.org/10.1007/s11255-022-03368-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-022-03368-1