
Abstract
Purpose/objectives
We report the outcomes of the largest cohort to date of patients receiving both bevacizumab (BEV) and fractionated stereotactic radiotherapy (FSRT) for progressive or recurrent high grade glioma (HGG). Furthermore, the sequence of these two treatment regimens was analyzed to determine an optimal treatment paradigm for recurrent HGG.
Materials/methods
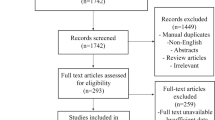
After Institutional Review Board approval, patients with pathologically confirmed WHO grade III anaplastic astrocytoma (AA) or IV glioblastoma multiforme (GBM) glioma who subsequently underwent re-irradiation at recurrence with FSRT were retrospectively reviewed. Patients from this group who had received BEV were also identified. Survival from initial diagnosis, as well as from recurrence and re-irradiation, were analyzed as study endpoints. Date of recurrence was defined as the date of radiographic evidence of progressive/recurrent disease. Kaplan–Meier curves were generated utilizing a log-rank test with a p-value ≤ 0.05 considered significant to compare treatment sequences in terms of survival outcomes.
Results
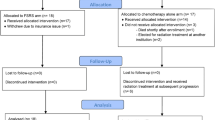
A total of 118 patients with recurrent/progressive HGG (GBM = 87, AA = 31) had received both BEV and FSRT. Patient characteristics were as follows: median KPS at recurrence was 80 (range 50–100); median age at recurrence was 57 years; median time to radiographic recurrence/progression was 10.8 months (mo) and 33.1% of patients had surgery for recurrence. The median time from the start of BEV to FSRT was 6.4 months and from FSRT to the start of BEV was 5.1 months. For the entire cohort, median overall survival (OS) was 26.7 months and median survival time (MST) from recurrence was 13.8 months (24.4 months and 11.9 months for GBM only). In patients that received BEV prior to FSRT (n = 50), median OS and MST from recurrence were 25.2 and 13.3 months respectively. In patients receiving FSRT first (n = 56), median OS and MST from recurrence were 28.8 months and 13.9 months, respectively. Sequencing of BEV and FSRT at recurrence was not significantly associated with OS (p = 0.08) or median survival from recurrence (p = 0.75).
Conclusions
The combination of FSRT and BEV for recurrent/progressive HGG provides promising results in terms of overall survival and survival from recurrence. Combining these treatment modalities appears to improve upon the historic outcomes of either treatment alone. The outcomes data from this study support the ongoing RTOG trial exploring the combination of BEV and FSRT for recurrent HGG.


Similar content being viewed by others

References
Ostrom QT, Gittleman H, Farah P et al (2013) CBTRUS statistical report: primary brain and central nervous system tumors diagnosed in the United States in 2006–2010. Neuro-Oncology 15(Suppl 2):ii1–i56. https://doi.org/10.1093/neuonc/not151
Stupp R, Mason WP, van den Bent MJ et al (2005) Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 352(10):987–996. https://doi.org/10.1056/NEJMoa043330
Gilbert MR, Wang M, Aldape KD et al (2013) Dose-dense temozolomide for newly diagnosed glioblastoma: a randomized phase III clinical trial. J Clin Oncol Off J Am Soc Clin Oncol 31(32):4085–4091. https://doi.org/10.1200/JCO.2013.49.6968
Gilbert MR, Dignam JJ, Armstrong TS et al (2014) A randomized trial of bevacizumab for newly diagnosed glioblastoma. N Engl J Med 370(8):699–708. https://doi.org/10.1056/NEJMoa1308573
Friedman HS, Prados MD, Wen PY et al (2009) Bevacizumab alone and in combination with irinotecan in recurrent glioblastoma. J Clin Oncol Off J Am Soc Clin Oncol 27(28):4733–4740. https://doi.org/10.1200/JCO.2008.19.8721
Vredenburgh JJ, Desjardins A, Herndon JE et al (2007) Bevacizumab plus irinotecan in recurrent glioblastoma multiforme. J Clin Oncol Off J Am Soc Clin Oncol 25(30):4722–4729. https://doi.org/10.1200/JCO.2007.12.2440
Wick W, Gorlia T, Bendszus M et al (2017) Lomustine and bevacizumab in progressive glioblastoma. N Engl J Med 377(20):1954–1963. https://doi.org/10.1056/NEJMoa1707358
Fogh SE, Andrews DW, Glass J et al (2010) Hypofractionated stereotactic radiation therapy: an effective therapy for recurrent high-grade gliomas. J Clin Oncol Off J Am Soc Clin Oncol 28(18):3048–3053. https://doi.org/10.1200/JCO.2009.25.6941
Combs SE, Gutwein S, Thilmann C, Huber P, Debus J, Schulz-Ertner D (2005) Stereotactically guided fractionated re-irradiation in recurrent glioblastoma multiforme. J Neurooncol 74(2):167–171. https://doi.org/10.1007/s11060-004-2463-y
Gutin PH, Iwamoto FM, Beal K et al (2009) Safety and efficacy of bevacizumab with hypofractionated stereotactic irradiation for recurrent malignant gliomas. Int J Radiat Oncol Biol Phys 75(1):156–163. https://doi.org/10.1016/j.ijrobp.2008.10.043
Shapiro LQ, Beal K, Goenka A et al (2013) Patterns of failure after concurrent bevacizumab and hypofractionated stereotactic radiation therapy for recurrent high-grade glioma. Int J Radiat Oncol Biol Phys 85(3):636–642. https://doi.org/10.1016/j.ijrobp.2012.05.031
Cabrera AR, Cuneo KC, Desjardins A et al (2013) Concurrent stereotactic radiosurgery and bevacizumab in recurrent malignant gliomas: a prospective trial. Int J Radiat Oncol Biol Phys 86(5):873–879. https://doi.org/10.1016/j.ijrobp.2013.04.029
Bevacizumab with or without radiation therapy in treating patients with recurrent glioblastoma. https://clinicaltrials.gov/ct2/show/NCT01730950. Accessed 5 jan 2018
Schmidt B, Lee H-J, Ryeom S, Yoon SS (2012) Combining bevacizumab with radiation or chemoradiation for solid tumors: a review of the scientific rationale, and clinical trials. Curr Angiogenes 1(3):169–179
Macdonald DR, Cascino TL, Schold SC, Cairncross JG (1990) Response criteria for phase II studies of supratentorial malignant glioma. J Clin Oncol 8(7):1277–1280. https://doi.org/10.1200/JCO.1990.8.7.1277
Wen PY, Macdonald DR, Reardon DA et al (2010) Updated response assessment criteria for high-grade gliomas: response assessment in neuro-oncology working group. J Clin Oncol 28(11):1963–1972. https://doi.org/10.1200/JCO.2009.26.3541
Common terminology criteria for adverse events v4.03. https://ctep.cancer.gov/protocolDevelopment/electronic_applications/docs/CTCAE_4.03.xlsx. Accessed 2 May 2015
Taal W, Oosterkamp HM, Walenkamp AME et al (2014) Single-agent bevacizumab or lomustine versus a combination of bevacizumab plus lomustine in patients with recurrent glioblastoma (BELOB trial): a randomised controlled phase 2 trial. Lancet Oncol 15(9):943–953. https://doi.org/10.1016/S1470-2045(14)70314-6
Cuneo KC, Vredenburgh JJ, Sampson JH et al (2012) Safety and efficacy of stereotactic radiosurgery and adjuvant bevacizumab in patients with recurrent malignant gliomas. Int J Radiat Oncol Biol Phys 82(5):2018–2024. https://doi.org/10.1016/j.ijrobp.2010.12.074
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest to disclose.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Palmer, J.D., Bhamidipati, D., Song, A. et al. Bevacizumab and re-irradiation for recurrent high grade gliomas: does sequence matter?. J Neurooncol 140, 623–628 (2018). https://doi.org/10.1007/s11060-018-2989-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11060-018-2989-z