
Abstract
The present study investigated the influence of strain in the form of adolescent motherhood on maladaptive coping in the form of delinquency among 6628 adolescent females. A series of tobit regression analyses revealed a significant, negative effect of adolescent motherhood on delinquency, a finding that persisted when controlling for coping factors and other known correlates of crime. Although these results are contrary to the predictions of general strain theory, the findings lend some support to theoretical approaches that associate low-self control, low self-esteem, and social support with delinquency. The results underscore the importance of considering measures of opportunity in future tests of general strain theory.
Similar content being viewed by others


Introduction
According to recent statistics, there were 273,105 babies born to adolescent females aged 15–19 in 2013, which translates to a rate of 26.5 births per 1000 females in this age group (United States Office of Adolescent Health 2015). The overwhelming majority of these births (89 %) took place outside of marriage. Given these figures, it is perhaps no surprise that some have referred to teen childbearing in the United States as an epidemic (McDonell et al. 2007). Although teen pregnancy rates have declined over the past 20 years, the teen birth rate in the US is still considerably higher than other developed nations (McDonell et al. 2007; Sheftall et al. 2010). Research on teen pregnancy is by no means a new endeavor, and scholars have identified a number of meaningful correlates (Hoskins and Simons 2015). Missing from the literature to date is a theoretically informed understanding of the ways in which adolescent mothers cope with the stressors of parenting. Agnew’s (1992, 2006) general strain theory (GST) offers insight into the relationships between adolescent motherhood, negative emotions, and maladaptive coping.
Within the criminological literature, tests of GST using adolescent samples have examined the processes by which strain results in delinquency, focusing on such strains as victimization and child maltreatment (Hollist et al. 2009; Kort-Butler 2010). Across adolescent and other populations, health-related issues have increasingly been conceptualized as sources of strain (Holtfreter et al. 2015; Stogner and Gibson 2010). The lives of adolescent mothers are similarly impacted in ways that reflect strain. For example, teen mothers experience an increase in stress associated with financial, academic, and psychological deficits. Compared to males and non-parents, teen mothers are at greater risk for experiencing negative emotional states such as depression as a result of these strains (Birkeland et al. 2005; Futris and Schoppe-Sullivan 2007; Sigfusdottir et al. 2004). Although there are many healthy ways of coping with negative emotions (e.g., exercising, and meditating), there are also maladaptive responses, such delinquency or substance abuse (Agnew 1992, 2006). Prior research suggests that there is a relationship between depression and delinquency among females (Dixon et al. 2004, Pulay et al. 2008; Vaske and Gehring 2010). Compared to their male counterparts, depression is more prevalent among female offenders (McClellan et al. 1997; Teplin et al. 2002; Vaske and Gehring 2010). Vaske and Gehring (2010) found that substance use was more common among females who experience higher levels of depression. This finding implies that substance abuse is a maladaptive coping mechanism for depressed females. The documented associations between pregnancy, depression and delinquency merit further investigation within the context of GST.
According to GST, delinquency is influenced indirectly by stressful life events, also known as strains. Agnew (1992, 2006) notes that strains take three main forms: (1) the actual or anticipated failure to achieve positively valued goals; (2) the removal of positively valued stimuli; and (3) the presentation of noxious stimuli. In the context of adolescent motherhood, the arrival of a child who is likely unplanned, coupled with drastic changes in lifestyle and routine, certainly could be considered “noxious stimuli.” The educational deficits that often follow teen parenthood reflect an actual or anticipated failure to achieve positively valued goals (e.g., a high school diploma and perhaps further education). In the language of GST, the disruption in social life and lost connections to formerly supportive peers are consistent with Agnew’s conceptualization of strain as the removal of positively valued stimuli. In the sections that follow, we present research findings that support our conceptualization of teen motherhood as consistent with the first and second types of strains previously articulated. Note, however, that likening a new baby to the presentation of noxious stimuli is largely assumed.
Despite a 30 % decrease in adolescent pregnancies since the early 1990s, teen parenting has remained a consistent social problem in the United States (Futris and Schoppe-Sullivan 2007; Klein 2005; Sheftall et al. 2010). For example, nearly a million teens between the ages of 15–19 become pregnant annually (Birkeland et al. 2005; McDonell et al. 2007). A significant number conceive out of wedlock, which may lead to subsequent strain (Singh and Darroch 2000; United States Office of Adolescent Health 2015). Stressors such as decreased financial resources, physical exhaustion, task overload, role restriction and confusion, social isolation, and depressive symptoms are all consequences associated with teenage motherhood (Birkeland et al. 2005; Uno et al. 1998; Webster-Stratton 1990). The responsibilities of childbearing contribute to academic, psychological, economic, and social problems for adolescent mothers (Futris and Schoppe-Sullivan 2007; Uno et al. 1998).
Conceptualizing adolescent childrearing as strain goes beyond the birthing of a child to the roles and responsibilities of mothers as primary caregivers of a newborn. Adolescent mothers may face many adversities, psychologically, economically, and physically in regards to their health, and the health of their child (Miller-Johnson et al. 1999); Compared to infants born to adult mothers, infants born to adolescent mothers are at higher risks for low birth weights, neurodevelopmental delay, and not surviving past the age of one (Rhein et al. 1997). Each of these factors may act as a stressor or strain on adolescent mothers. Early childbearing can be an expensive responsibility that places a financial strain on teen mothers (McDonell et al. 2007). Adolescent parents are more likely to have larger families and to receive welfare (Klepinger et al. 1995). Expenses associated with the care of a child such as toiletries, food, and other costs are often difficult for adolescent mothers, resulting in an increased likelihood that they will rely on government assistance for support. Problems arising from teen parenting extend beyond the immediate financial responsibilities and into the social realm of adolescent mothers.
Although having a social life is important during the adolescent period, it may be extremely difficult for teen mothers to maintain friendships while adjusting to their new responsibilities. Clifford and Brykczynski (1999) describe the experience of adolescent mothers as living in two worlds: adolescence and motherhood. Once a teen gives birth to a child, she will no longer be able to engage in the level of social activities she once enjoyed prior to childbirth. As a result, friendships may be hindered, causing teen mothers to rely on others (e.g., grandparents of the child) for support (Miller-Johnson et al. 1999). Adolescent mothers are more likely to become depressed or socially isolated, limiting their social sphere to other teenage mothers. Research suggests that the friends of adolescent mothers have difficulty understanding their peers’ new childcare responsibilities, which increases the prevalence of social isolation (Wayland and Rawlins 1997). Intimate ties promote a sense of identity and emotional security, and act as a safeguard against the effects of stress; these buffers are reduced for adolescent mothers (Zippay 1995). Social isolation limits access to support to help teens cope positively with parenting strains (McDonell et al. 2007). In line with GST, the disruption in friendship networks that accompanies teen motherhood reflects the removal of positively valued stimuli.
Many studies demonstrate the negative impact of teen childbearing on a mother’s educational aspirations. Compared to non-parenting teens, teen mothers typically perform poorly in school and are less likely to complete their education (McDonell et al. 2007). Klepinger et al. (1995) found that, irrespective of race or ethnicity, teen mothers were one to three years behind their peers in school. Data from the National Longitudinal Survey of Youth indicate that 35 % of teen mothers graduated from high school compared to 85 % of teens who did not have children (Hotz et al. 1997; Klepinger et al. 1995). This lack of education limits one’s ability to work in certain positions, as well as receive adequate pay needed to achieve the “American Dream.” Individuals who become parents as teens are more likely than their non-parenting counterparts to have their educational journey truncated (Fletcher and Wolfe 2012). Teenage fatherhood decreases years of schooling, and increases the likelihood of general education development (GED) receipt (Fletcher and Wolfe 2012). Younger mothers face even greater educational deficits than young fathers given their roles as primary caregivers. In the context of GST, the findings regarding teen parenting and educational shortcomings mirror the conceptualization of strain as the actual or anticipated failure to achieve positively valued goals.
According to GST, strain leads to an increase in negative emotionality (i.e., anger, frustration, anxiety and depression) consequently leading to involvement in crime as a means of corrective action. The central assumption of GST is that delinquency arises as a response to stressful life events (Mazerolle and Maahs 2000). Compared to adult mothers, adolescent mothers experience higher levels of depressive symptoms (Deal and Holt 1998). Postpartum depression may result, at least in part, from the hormonal changes that occur after giving birth to a child. This experience can be challenging for any mother, but may be especially challenging for teens. During the postpartum period, one out of every four women experiences some form of emotional distress (Birkeland et al. 2005). Teenage mothers may be at risk for engaging in crime-analogous or delinquent behaviors as a means of coping with negative emotional states.
Depression is correlated with a variety of negative outcomes, including delinquent and criminal behavior (Daigle et al. 2007). Affective disorders are more prevalent among females than males (Hodgkinson and Prins 2011). Depressive symptoms account for a significant amount of affective disorders experienced by females (Hodgkinson and Prins 2011). Females are twice as likely as males to experience symptoms of depression (e.g., Nolen-Hoeksema 2001). Female depression has been linked to biological vulnerability (Birkeland et al. 2005; Hodgkinson and Prins 2011). Female hormones (e.g., estrogen) have an effect on mood and negative emotions (Hodgkinson and Prins 2011; Wisner et al. 2002).
Other factors that increase female vulnerability to depression include low income, unemployment or low employment status, low educational levels, larger family sizes, and lack of a supportive relationship (Hodgkinson and Prins 2011). Women may respond to strains via negative emotions like depression, as opposed to anger (Hodgkinson and Prins 2011). Moreover, depression has been associated with higher levels of involvement in delinquent and criminal behavior, including violence (Beyers and Loeber 2003; Dixon et al. 2004; Pulay et al. 2008). Consistent with GST, delinquency is a maladaptive way of coping (Agnew 1992, 2006).
According to GST, negative affective states (e.g., anger, depression, and frustration) may arise within individuals who face strains (Mazerolle and Maahs 2000). The chances of delinquent outcomes are increased when anger and frustration occur as a response to strain (Mazerolle and Maahs 2000). Agnew (2001) states, “Crime may be a method for reducing strain (e.g., stealing money one desires), seeking revenge, or alleviating negative emotions (e.g., through illicit drug use)” (p. 319). Coping is fundamental when handling strains and stressors. Prior research suggests that females tend to respond to strain with sadness and depression, while males turn outward (e.g., with anger and frustration) (Broidy and Agnew 1997). In the context of adolescent motherhood, GST would suggest that the relationship between teen parenting and delinquency is by negative emotionality, in the form of depression.
According to Agnew (2006), a number of coping factors may condition the effects of strain. For example, self-esteem, social support, self-efficacy, prior deviant experiences, intelligence, moral beliefs, and affiliation with deviant peers have all been identified as causes of delinquent responses to negative emotions (Agnew 1992). Delinquency and a variety of risky, crime-analogous acts (e.g., excessive drinking, using drugs, driving too fast, engaging in illicit sex, and gambling) may be explained by underlying personality traits, such as low self-control or low constraint (Chapple 2005; Gottfredson and Hirschi 1990; Pratt and Cullen 2000). Individuals lacking in self-control are often more physical, more impulsive, and easily provoked, and more likely to cope with strain through delinquency (Mazerolle and Maahs 2000). In short, an individual’s levels of self-control may explain involvement in criminal or deviant behavior, as well as the response to strain (Gottfredson and Hirschi 1990; Mazerolle and Maahs 2000; Pratt and Cullen 2000). In a different vein, the availability of social support can buffer individuals from strain, thus decreasing the likelihood of maladaptive coping (Kaufman 2009). The analyses that follow thus account for low self-control—a known correlate of crime—and also consider the role of two coping factors: low self-esteem and social support.
Drawing on general strain theory, the current study addresses the following research questions: (1) Is the stressful life event of teen motherhood associated with maladaptive coping in the form of delinquency? (2) Do negative emotions (conceptualized as depressive symptomology) mediate the relationship between teen motherhood and delinquency? That is, when depression is included in the model, is the relationship between teen motherhood and maladaptive coping reduced to non-significance? (3) Does the effect of teen motherhood on delinquency persist when controlling for low self-esteem, low self-control, and social support?
Method
Participants
The data for this study were drawn from the second wave of the National Longitudinal Survey of Adolescent Health (Add Health). The Add Health data consists of a national sample of adolescents in grades 7th through 12th who were randomly selected from 80 high schools and 52 middle schools across the United States between 1994 and 1995. In the recruitment process, researchers stratified schools by region of country, urbanicity, school size, school type, and ethnicity to ensure that the data were representative of the schools in the United States (Bearman et al. 1997). Although sampling weights are available, they are not applied in the analyses that follow.
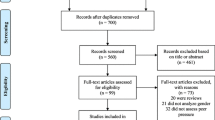
Procedure
The present study uses wave two of the restricted Add Health data due to the lack of adolescent mothers represented in wave 1. The second wave was conducted in 1996, which consisted of nearly 15,000 students who participated in the follow-up to the in-home interviews that were administered at wave one. Respondents who were in grade 12 in the first wave were not included in wave two. In addition, the data that are used in the current study are solely from female respondents; of the 14,738 participants, 7556 were female. After restricting the data to females only, and taking into account missing data using listwise deletion, the final study sample was 6628 participants. More specifically, the data were made up of females between the ages of 11 and 21 years old (M = 15.98, SD 1.58). The data included 67 (1.01 %) adolescent mothers (≤17 years old), and two comparison groups comprised of 62 (0.94 %) adult mothers (≥18 years old) and 6499 (98.05 %) non-mother participants. In regards to racial/ethnic background, approximately 58.36 % of the sample was White, while the remaining 41.64 % was made up of racial and ethnic minorities.
Measures
To measure involvement in delinquent behavior, the current study uses 13 items that range from relatively minor acts (e.g., stealing something less than $50) to serious violent acts (e.g., shot or stabbed someone) (Dornbusch et al. 2001). Participants were asked how often they committed these particular acts over the past 12 months. Each item featured a 4 point scale: (0) never, (1) 1 or 2 times, (2) 3 or 4 times, and (3) 5 or more times. The items were summed to create an additive scale (α = 0.76). Higher scores indicate more reported instances of delinquency. See the “Appendix” for a complete list of the items used to construct the delinquency scale.
Consistent with prior research, the current study defines an adolescent as an individual between the ages of 12 and 17 (Mersky et al. 2012; Robbins et al. 2008). Adolescent motherhood is defined as a female who gave birth to a child between the ages of 12 and 17, and who is actively involved in the child rearing process. Adolescent motherhood is constructed using two survey items. First, pregnant females self-reported how their pregnancy ended. Responses were coded dichotomously (0 = no live birth and 1 = live birth). The second item asked mothers, “Does the child live with you?” This item captures child rearing. The adolescent motherhood variable was constructed by summing the two dummy coded variables. Participants who scored a 2 (indicating childbearing and child rearing) were classified as adolescent mothers (coded 1), while all others were coded as otherwise (coded 0).
Depression is operationalized as an 11-item additive scale (see Peck 2013). The scale includes items taken from the CES-D (Radloff 1977) that asked adolescents, in the past 7 days, how often: (1) you felt depressed, (2) you thought your life had been a failure, (3) you were bothered by things that usually don’t bother you, (4) you did not feel like eating, (5) you talked less than usual, (6) you felt lonely, (7) you felt sad, (8) you thought people disliked you, (9) life was not worth living, (10) you felt like you could not shake off the blues even with help from my family and friends, and (11) you enjoyed life (reverse coded). Responses were closed-ended: (0) never/rarely, (1) sometimes, (2) a lot of times, and (3) most/all the time. The scale was coded so that higher scores indicate higher levels of depression (α = 0.85; mean inter-item r = 0.170). Depression was used as opposed to other forms of negative emotionality (e.g., anger, frustration, and anxiety) because past research has shown that females are more likely to experience depression when compared to their male counterparts (see Hodgkinson and Prins 2011; Smith et al. 2008). Furthermore, adolescent mothers are at risk for experience postpartum depression after conceiving (Birkeland et al. 2005).
We include low self-control, low self-esteem, and social support in the analyses, as they all have been found to influence coping. Low self-control was measured using a 4-item low self-control scale adapted from Perrone et al. (2004). Specific items included how often each of the following occurred: (1) you had trouble keeping your mind on what you were doing, (2) you had trouble getting your homework done, (3) you had trouble paying attention in school, and (4) you had trouble getting along with your teachers. The responses for the first item were coded as (0) never, (1) sometimes, (2) a lot of times, (3) most/all of the time. Reponses for the remaining items were coded as (0) never, (1) just a few times (2) about once a week, (3) almost every day, and (4) every day. The items were summed to create an additive scale. Higher scores indicate lower levels of self-control (α = 0.68, mean inter-item r = 0.304).
Low self-esteem was measured using Rosenberg’s (1965) 6-item scale. The measures asked respondents on a scale of one-to-five: (1 = strongly agree, 2 = agree, 3 = neither agree nor disagree, 4 = disagree, and 5 = strongly disagree) how much they agree with the following items: (1) you have a lot of good qualities, (2) you have a lot to be proud of, (3) you like yourself the way that you are, (4) you feel like you are doing everything just about right, (5) you feel socially accepted, and (6) you feel loved and wanted. Higher scores on the additive scale indicated lower levels of self-esteem (α = 0.85, mean inter-item r = 0.300).
Lastly, social support was operationalized using a 7-item additive scale (see Wight et al. 2006). The scale includes items asking respondents, “how much do you feel that…”: (1) adults care about you, (2) your teachers care about you, (3) your parents care about you, (4) your friends care about you, (5) people in your family understand you, (6) your family pays attention to you, and (7) you and your family have fun together. Items were coded as (0) not at all (1) very little, (2) somewhat, (3) quite a bit, and (4) very much. The scale was coded so that higher scores indicate higher levels of social support (α = 0.79, mean inter-item r = 0.275).
Age and White are included as statistical controls in the multivariate analyses to guard against spuriousness. Age was measured in years (M = 15.96, SD 1.58), while White was a dummy variable (1 = yes, 0 = no).
Data Analysis
The data analytic strategy consists of several steps. To conduct diagnostics and preliminary hypothesis testing, the analyses begin by presenting bivariate correlations for the dependent, independent, and control variables. Because the correlations between the independent variables did not exceed |.45|, harmful levels of collinearity did not appear to be a problem. This conclusion was supported after conducting model diagnostics (VIF range = 1.00–1.43, mean VIF = 1.21). Next, because there is evidence of over-dispersion in the delinquency scale (mean = 2.46, variance = 11.08), and the outcome variable is truncated at the lower end of the distribution, the study estimates a series of tobit regression models. To check for heteroscedasticity, the Bruesch–Pagan test was used. The results indicated the presence of heteroscedasticity (χ2 = 2615.69, p < .001). Therefore, robust standard errors are estimated. All analyses were conducted in STATA 13 (StataCorp, College Station, TX).
Results
The descriptive statistics and bivariate correlations for the variables used in the current study are presented in Table 1. At the bivariate level, several significant associations between variables of interest are observed. First, as expected, depression is significantly and positively related to delinquency in the current study (r = 0.247; p ≤ .001). On the other hand, the relationship between adolescent motherhood and depression was not significant at the bivariate level. Second, there is a significant and negative correlation between low self-esteem and delinquency at the bivariate level (r = 0.203; p ≤ .001). This suggests that individuals with lower levels of self-esteem are more likely to be involved in delinquent behaviors, providing support to findings from previous research (Trzesniewski et al. 2006). Third, consistent with prior research (Gottfredson and Hirschi 1990; Pratt and Cullen 2000), low self-control is correlated with involvement in delinquency (r = 0.364; p ≤ .001). Stated differently, individuals with low levels of self-control were at increased risk for engaging in problem behaviors. Fourth, at the bivariate level social support was statistically and negatively associated with delinquency (r = −0.290; p ≤ .001). In other words, those with higher levels of social support are less likely to be delinquent. This finding affirms the notion that social support may influence coping outcomes among individuals who experience strains and stressors (Agnew 2006). Lastly, although the relationship is not statistically significant at the bivariate level, there is a negative correlation between adolescent motherhood and delinquency (r = −0.02; p ≤ .10). When compared to non-mother adolescents and older mothers (18 years or older), adolescent mothers are less likely to be involved in delinquent behavior. This finding implies that adolescent motherhood is negatively associated with delinquent behavior. The next set of analyses investigates these relationships in a multivariate context.
As noted previously, the dependent variable is a count variable, and over-dispersion was detected. Accordingly, Table 2 presents a series of tobit regression models. The F-statistic for each model reached statistical significance (p ≤ .001), indicating that the models fit the data well. Model 1 provides the unstandardized estimate for the relationship between adolescent motherhood and delinquency among the participants in the study, net of control variables. The unstandardized coefficient suggests that being an adolescent mother decreases the probability of being involved in delinquent behavior by 61 % (p ≤ .05), a finding that runs counter to our predictions. Regarding control variables, being white did not reach statistical significance, while age was negative and significantly associate with delinquency (b = −0.22; p ≤ .001). The hypothesized mediator (i.e., depression) enters the equation in model 2.
After adding depression into the equation in model 2, no mediation effect between adolescent motherhood and delinquency was observed. The effect of adolescent motherhood on delinquent behavior was negative and significant, net of control variables (b = −0.72; p ≤ .01). More specifically, being an adolescent mother was associated with a 72 % decrease in the probability of engaging in delinquent behavior. Although depression did not mediate the relationship between adolescent motherhood and delinquency, it was the strongest predictor of delinquency. For instance, every one standard deviation increase in depression is associated with a 17 % increase in delinquency. In short, while depression does not mediate the relationship between adolescent motherhood and delinquency, it does increase the probability of delinquency; the latter finding is consistent with past research identifying direct effects of negative emotions on maladaptive coping.
Model 3 regresses delinquency on adolescent motherhood, net of coping factors, and statistical controls. Model 3 shows that adolescent motherhood remained statistically significant. More specifically, the unstandardized coefficient indicates that being an adolescent mother reduces the probability of delinquent behaviors by 49 % (p ≤ .05). In regards to negative emotionality, depression increased the probability of engaging in delinquent activity. Unsurprisingly, low-self control was the strongest predictor of delinquency, which is consistent with previous research (Pratt and Cullen 2000). For instance, every one standard deviation increase in low self-control was associated with a 34 % increase in delinquency (p ≤ .001). Next, low self-esteem was positive and significantly correlated with delinquency. Individuals with low levels of self-esteem were at increased risk for involvement in delinquent behavior (b = 0.03; p ≤ .05). The last coping factor suggested by past research to influence the response to strain is social support. Social support has a negative and statistically significant effect on delinquency, a finding that highlights the importance of supportive family, peers, and others among adolescents. More specifically, for every one standard deviation increase in social support, there was a 13 % decrease in delinquency (p ≤ .001). Indeed, social support appears to operate as a protective factor in this at-risk population of youth. We suspect also that unmeasured forms of support (e.g., access to governmental assistance programs) may also help alleviate some of the pressures associated with adolescent motherhood (i.e., financial problems), thus potentially explaining the negative relationship between our measure of strain and delinquency. Note also that age remained a significant predictor of delinquency throughout all the models; specifically, as age increases, levels of delinquency decrease. This finding is consistent with life course explanations of desistance from offending. We now turn to the implications of these results for theory, research and policy.
Discussion
Guided by GST and prior research, the current study examined the relationship between adolescent motherhood and delinquency, more specifically, the role of depression as a potential mediator. Previous work (see Hope et al. 2003) examining this relationship failed to take into account negative emotions (i.e., depression) that may arise from the strains of teen parenting (e.g., financial, educational, psychological, etc.). We found a direct and statistically significant effect of adolescent motherhood on delinquency, albeit in the opposite direction of theoretical expectations. Moreover, the relationship between teen motherhood and delinquency was not mediated by depression, and the effect of teen motherhood on delinquency persisted when controlling for low self-control, low self-esteem, and social support. Consistent with prior research, depression, low self-control, and low self-esteem were all significant risk factors for delinquency, while social support significantly decreased delinquency. The results reported here have implications for theory and future research, as well as policy efforts aimed at addressing the consequences of teen parenting.
The finding that adolescent motherhood reduces delinquency appears to run counter to the predictions of general strain theory. Recall Agnew’s (1992, p. 64) contention that the strains most conducive to delinquency are those that are of “high magnitude, clustered, recent, of a long duration, perceived as unjust, and caused by or associated with low social control.” In our conceptualization of strain, the stressors of adolescent motherhood are implied but remain unmeasured directly (e.g., financial, educational, etc.). For some adolescents, it may be that teen motherhood lacks important qualitative dimensions of other strains (e.g., victimization) that have been linked to delinquency and other forms of maladaptive coping (e.g., substance abuse). That is not to say that teen mothers do not experience strain in the form of actual or anticipated failure to achieve positively valued goals, the removal of positively valued stimuli, and the presentation of noxious stimuli. Rather, the source and nature of the strain itself—a new baby—simply limits opportunity for delinquency.
Although many responsibilities and adversities may result from adolescent motherhood, the childrearing process for some adolescent mothers may create a sense of meaning and hope, and an opportunity to create a new self-identity (Clemmens 2003; Edin and Kefalas 2005). In other words, motherhood may serve as a “turning point” in the lives of adolescents, causing them to refrain from or “quit” delinquent behavior. Sampson and Laub (1990) provide reasoning for why individuals desist from criminal involvement through life course transitions, (e.g., marriage, employment, and education). Certain life course transitions place informal social controls on individuals, contributing to desistence from criminal and delinquent behaviors (Clemmens 2003; Sampson and Laub 1990). Along these lines, motherhood is a major life event (e.g., life course transition) for females, which may promote desistence from delinquent behavior. Factors unmeasured here—such as attachment to their children as well as to their own parents—could also serve as a protective factor for teens. In short, most research highlights the negative outcomes of adolescent motherhood, but a positive consequence suggested by the current study may be the end of delinquency. Longitudinal research that investigates whether the protective effects of teen motherhood have a lasting impact on desistance would be a welcome addition to this literature.
As in nearly all research, limitations are inevitable. One limitation of the current study is that the analyses are conducted using a cross sectional research design. More specifically, depression and delinquency were measured at the same time, which limits the ability to make causal inferences. Nonetheless, it is important to note that the relationship between depression and delinquency is in the anticipated theoretical direction. Additionally, we relied on a female only sample. Males obviously play a role in teen parenting, albeit a lesser one in many cases. Subsequent studies should consider examining the effects of teen parenting on delinquency among males, especially with regard to the role that negative emotions may play and the extent to which both of these outcomes may be gendered. For example, males may respond to the strains of fatherhood with anger, as opposed to depression. Males may cope with anger in positive (e.g., help-seeking) or maladaptive ways (e.g., delinquency). GST asserts that anger and frustration produce emotional reactions that increase the likelihood of a criminal response (e.g., aggressing others) (Broidy and Agnew 1997). In other words, individuals who experience anger and frustration may be at higher risk for delinquent involvement then those who only experience depression. Future research examining the effects of teenage parenthood on a variety of negative emotions, and links to delinquency in males as well as females might shed more light on these relationships.
Although teenage pregnancy rates may be on the decline, it is clear that teen motherhood remains an important social and public health problem in the United States. A variety of institutions (e.g., the family, school, and health care) should continue to play a role in the prevention of teen pregnancy through education and prevention strategies. Despite such efforts, adolescents still account for a significant portion of births, presenting challenges for social services, public health, and education. The negative impact of teen motherhood on delinquency may be explained, at least in part, by the availability of public assistance programs, such as Women, Infants, and Children (WIC), the supplemental nutrition program provided by the United States Department of Agriculture. More specifically, such services can directly address the financial strains experienced by teen mothers. Unfortunately, the Add Health data do not include measures of access to such services. Future research should attempt to directly evaluate the impact of social programs in the lives of teen parents.
The current study also suggests that service providers should be especially attuned to the mental health needs of adolescent mothers (e.g., depression) to help teens develop pro-social (as opposed to maladaptive) coping mechanisms. In addition, service providers should consider implementing risk assessments for teenage mothers to detect signs of depression in order to better provide for the needs of this population (Cox et al. 2008). Given our findings that low self-control and low self-esteem increased delinquency, and social support served as a protective factor, programs directed toward increasing self-control, self-esteem, and social support would be useful. Previous studies demonstrate that quality of parenting is also related to these outcomes, as well as to delinquency and risky sexual behavior (Brody et al. 2004). Incorporating parents into interventions would therefore also be a logical step. Educational administrators should also pay close attention to challenges facing adolescent mothers so they can best accommodate needs and service to increase other positive outcomes that may also reduce delinquency, such as high school graduation. Strengthening connections between social institutions is also important. For example, delinquency prevention programs that are administered in a school setting could help not just depressed teen mothers, but all adolescents, desist from crime and successfully transition into adulthood.
References
Agnew, R. (1992). Foundation for a general strain theory of crime and delinquency. Criminology, 30(1), 47–88.
Agnew, R. (2001). Building on the foundation of general strain theory: Specifying the types of strain most likely to lead to crime and delinquency. Journal of research in crime and delinquency, 38(4), 319–361.
Agnew, R. (2006). Pressured into crime: An overview of general strain theory. New York: Oxford University Press.
Bearman, P.S., Jones, J., & Undry, J. R. (1997). The National Longitudinal Study of Adolescent Health Research design. www.cpc.unc.edu/addhealth
Beyers, J. M., & Loeber, R. (2003). Untangling developmental relations between depressed mood and delinquency in male adolescents. Journal of Abnormal Child Psychology, 31(3), 247–266.
Birkeland, R., Thompson, J. K., & Phares, V. (2005). Adolescent motherhood and postpartum depression. Journal of Clinical Child and Adolescent Psychology, 34(2), 292–300.
Brody, G. H., Murry, V. M., Gerrard, M., Gibbons, F. X., Molgaard, V., McNair, L., et al. (2004). The strong African-American families program: Translating research into prevention programming. Child Development, 75(3), 900–917.
Broidy, L., & Agnew, R. (1997). Gender and crime: A general strain theory perspective. Journal of Research in Crime and Delinquency, 34(3), 275–306.
Chapple, C. L. (2005). Self-control, peer relations, and delinquency. Justice Quarterly, 22(1), 89–106.
Clemmens, D. (2003). Adolescent motherhood: a meta-synthesis of qualitative studies. The American Journal of Maternal/Child Nursing, 28(2), 93–99.
Clifford, J., & Brykczynski, K. (1999). Giving voice to childbearing teens: Views on sexuality and the reality of being a young parent. The Journal of School Nursing, 15(1), 4–15.
Cox, J. E., Buman, M., Valenzuela, J., Joseph, N. P., Mitchell, A., & Woods, E. R. (2008). Depression, parenting attributes, and social support among adolescent mothers attending a teen tot program. Journal of Pediatric and Adolescent Gynecology, 21(5), 275–281.
Daigle, L. E., Cullen, F. T., & Wright, J. P. (2007). Gender differences in the predictors of juvenile delinquency assessing the generality-specificity debate. Youth Violence and Juvenile Justice, 5(3), 254–286.
Deal, L. W., & Holt, V. L. (1998). Young maternal age and depressive symptoms: Results from the 1988 National Maternal and Infant Health Survey. American Journal of Public Health, 88(2), 266–270.
Dixon, A., Howie, P., & Starling, J. (2004). Psychopathology in female juvenile offenders. Journal of Child Psychology and Psychiatry, 45(6), 1150–1158.
Dornbusch, S. M., Erickson, K. G., Laird, J., & Wong, C. A. (2001). The relation of family and school attachment to adolescent deviance in diverse groups and communities. Journal of Adolescent Research, 16(4), 396–422.
Edin, K., & Kefalas, M. (2005). Promises I can keep: Why poor women put motherhood before marriage. Berkeley: University of California Press.
Fletcher, J. M., & Wolfe, B. L. (2012). The effects of teenage fatherhood on young adult outcomes. Economic Inquiry, 50(1), 182–201.
Futris, T. G., & Schoppe-Sullivan, S. J. (2007). Mothers’ perceptions of barriers, parenting alliance, and adolescent fathers’ engagement with their children. Family Relations, 56(3), 258–269.
Gottfredson, M. R., & Hirschi, T. (1990). A general theory of crime. Palo Alto, CA: Stanford University Press.
Hodgkinson, S., & Prins, H. (2011). Perspectives on depression, gender and crime: Depression sometimes masked, missed and misunderstood? Probation Journal, 58(2), 137–154.
Hollist, D. R., Hughes, L. A., & Schaible, L. M. (2009). Adolescent maltreatment, negative emotion, and delinquency: An assessment of general strain theory and family-based strain. Journal of Criminal Justice, 37(4), 379–387.
Holtfreter, K., Reisig, M. D., & O’Neal, E. N. (2015). Prescription drug misuse in late adulthood: An empirical examination of competing explanations. Journal of Drug Issues. doi:10.1177/0022042615589405
Hope, T. L., Wilder, E. I., & Watt, T. T. (2003). The relationships among adolescent pregnancy, pregnancy resolution, and juvenile delinquency. The Sociological Quarterly, 44(4), 555–576.
Hoskins, D. H., & Simons, L. G. (2015). Predicting the risk of pregnancy among African American youth: Testing a social contextual model. Journal of Child and Family Studies, 24(4), 1163–1174.
Hotz, V. J., McElroy, S. W., & Sanders, S. G. (1997). The impacts of teenage childbearing on the mothers and the consequences of those impacts for government. In R. Maynard (Ed.), Kids having kids: Economic costs and social consequences of teen pregnancy (pp. 55–94). Washington, DC: The Urban Institute Press.
Kaufman, J. M. (2009). Gendered responses to serious strain: The argument for a general strain theory of deviance. Justice Quarterly, 26(3), 410–444.
Klein, J. D. (2005). Adolescent pregnancy: Current trends and issues. Pediatrics, 116(1), 281–286.
Klepinger, D. H., Lundberg, S., & Plotnick, R. D. (1995). Adolescent fertility and the educational attainment of young women. Family Planning Perspectives, 27(1), 23–28.
Kort-Butler, L. (2010). Experienced and vicarious victimization: Do social support and self-esteem prevent delinquent responses? Journal of Criminal Justice, 38(4), 496–505.
Mazerolle, P., & Maahs, J. (2000). General strain and delinquency: An alternative examination of conditioning influences. Justice Quarterly, 17(4), 753–778.
McClellan, D. S., Farabee, D., & Crouch, B. M. (1997). Early victimization, drug use, and criminality a comparison of male and female prisoners. Criminal Justice and Behavior, 24(4), 455–476.
McDonell, J. R., Limber, S. P., & Connor-Godbey, J. (2007). Pathways teen mother support project: Longitudinal findings. Children and Youth Services Review, 29(7), 840–855.
Mersky, J. P., Topitzes, J., & Reynolds, A. J. (2012). Unsafe at any age: Linking childhood and adolescent maltreatment to delinquency and crime. Journal of Research in Crime and Delinquency, 49(2), 295–318.
Miller-Johnson, S., Winn, D., Coie, J., Maumary-Gremaud, A., Hyman, C., Terry, R., & Lochman, J. (1999). Motherhood during the teen years: A developmental perspective on risk factors for childbearing. Development and Psychopathology, 11(1), 85–100.
Nolen-Hoeksema, S. (2001). Gender differences in depression. Current Directions in Psychological Science, 10(5), 173–176.
Peck, J. H. (2013). Examining race and ethnicity in the context of general strain theory, depression, and delinquency. Deviant Behavior, 34(9), 706–726.
Perrone, D., Sullivan, C. J., Pratt, T. C., & Margaryan, S. (2004). Parental efficacy, self-control, and delinquency: A test of a general theory of crime on a nationally representative sample of youth. International Journal of Offender Therapy and Comparative Criminology, 48(3), 298–312.
Pratt, T. C., & Cullen, F. T. (2000). The empirical status of Gottfredson and Hirschi’s general theory of crime: A meta-analysis. Criminology, 38(3), 931–964.
Pulay, A. J., Dawson, D. A., Hasin, D. S., Goldstein, R. B., Ruan, W. J., Pickering, R. P., et al. (2008). Violent behavior and DSM-IV psychiatric disorders: results from the national epidemiologic survey on alcohol and related conditions. The Journal of Clinical Psychiatry, 69(1), 12–22.
Radloff, L. S. (1977). The CES-D scale: A self-report depression scale for research in the general public. Applied Psychological Measurement, 1(3), 385–401.
Rhein, L. M., Ginsburg, K. R., Schwarz, D. F., Pinto-Martin, J. A., Zhao, H., Morgan, A. P., & Slap, G. B. (1997). Teen father participation in child rearing: Family perspectives. Journal of Adolescent Health, 21(4), 244–252.
Robbins, M. S., Szapocznik, J., Dillon, F. R., Turner, C. W., Mitrani, V. B., & Feaster, D. J. (2008). The efficacy of structural ecosystems therapy with drug-abusing/dependent African American and Hispanic American adolescents. Journal of Family Psychology, 22(1), 51–61.
Rosenberg, M. (1965). Society and the adolescent self-image. Princeton, NJ: Princeton University Press.
Sampson, R. J., & Laub, J. H. (1990). Crime and deviance over the life course: The salience of adult social bonds. American Journal of Sociology, 55(5), 609–627.
Sheftall, A. H., Schoppe-Sullivan, S. J., & Futris, T. G. (2010). Adolescent mothers’ perceptions of the co-parenting relationship with their child’s father: A function of attachment, security, and trust. Journal of Family Issues, 31(7), 884–905.
Sigfusdottir, I. D., Farkas, G., & Silver, E. (2004). The role of depressed mood and anger in the relationship between family conflict and delinquent behavior. Journal of Youth and Adolescence, 33(6), 509–522.
Singh, S., & Darroch, J. E. (2000). Adolescent pregnancy and childbearing: levels and trends in developed countries. Family Planning Perspectives, 32(1), 14–23.
Smith, D. J., Kyle, S., Forty, L., Cooper, C., Walters, J., Russell, E., et al. (2008). Differences in depressive symptom profile between males and females. Journal of Affective Disorders, 108(3), 279–284.
Stogner, J., & Gibson, C. L. (2010). Healthy, wealthy, and wise: Incorporating health issues as a source of strain in Agnew’s general strain theory. Journal of Criminal Justice, 38(6), 1150–1159.
Teplin, L. A., Abram, K. M., McClelland, G. M., Dulcan, M. K., & Mericle, A. A. (2002). Psychiatric disorders in youth in juvenile detention. Archives of General Psychiatry, 59(12), 1133–1143.
Trzesniewski, K. H., Donnellan, M. B., Moffitt, T. E., Robins, R. W., Poulton, R., & Caspi, A. (2006). Low self-esteem during adolescence predicts poor health, criminal behavior, and limited economic prospects during adulthood. Developmental Psychology, 42(2), 381.
United States Office of Adolescent Health. (2015). Trends in teen pregnancy and childbearing. Washington, DC: United States Department of Health and Human Services.
Uno, D., Florsheim, P., & Uchino, B. N. (1998). Psychosocial mechanisms underlying quality of parenting among Mexican-American and white adolescent mothers. Journal of Youth and Adolescence, 27(5), 585–605.
Vaske, J., & Gehring, K. (2010). Mechanisms linking depression to delinquency for males and females. Feminist Criminology, 5(1), 8–28.
Wayland, J., & Rawlins, R. (1997). African American teen mothers’ perceptions of parenting. Journal of Pediatric Nursing, 12(1), 13–20.
Webster-Stratton, C. (1990). Stress: A potential disrupter of parent perceptions and family interaction. Journal of Clinical Child Psychology, 19(4), 302–312.
Wight, R. G., Botticello, A. L., & Aneshensel, C. S. (2006). Socioeconomic context, social support, and adolescent mental health: A multilevel investigation. Journal of Youth and Adolescence, 35(1), 109–120.
Wisner, K. L., Parry, B. L., & Piontek, C. M. (2002). Postpartum depression. New England Journal of Medicine, 347(3), 194–199.
Zippay, A. (1995). Expanding employment skills and social networks among teen mothers: Case study of a mentor program. Child and Adolescent Social Work Journal, 12(1), 51–69.
Acknowledgments
The authors would like to thank Mike Reisig, Callie Burt, and the anonymous reviewers for their helpful comments on earlier drafts of this article.
Author information
Authors and Affiliations
Corresponding author
Appendix: Scale Items for Delinquency Measure
Appendix: Scale Items for Delinquency Measure
The delinquency scale was created by summing responses to the following items:
-
1.
Paint graffiti or signs on someone else’s property or in a public place.
-
2.
Deliberately damage property that didn’t belong to you.
-
3.
Lie to your parents or guardians about where you had been or whom you were with.
-
4.
Take something from a store without paying for it.
-
5.
Run away from home.
-
6.
Drive a car without its owner’s permission.
-
7.
Steal something worth more than $50.
-
8.
Go into a house or building to steal something.
-
9.
Steal something worth less than $50.
-
10.
Act loud, rowdy, or unruly in a public place.
-
11.
Get into a serious fight.
-
12.
Hurt someone badly enough to need bandages or care from a doctor or nurse.
-
13.
Use or threaten to use a weapon to get something from someone.
Rights and permissions
About this article

Cite this article
Walker, D., Holtfreter, K. Adolescent Motherhood, Depression, and Delinquency. J Child Fam Stud 25, 939–948 (2016). https://doi.org/10.1007/s10826-015-0268-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-015-0268-6