
Abstract
Background and Aims
18F-fluorocholine positron emission tomography/computed tomography (18F-FCH PET/CT) is an emerging functional imaging technique in the diagnosis and management of hepatocellular carcinoma (HCC). The aim of this study was to assess the ability of a pre- and post-treatment 18F-FCH PET/CT to predict prognosis and treatment response in early-stage HCC.
Methods
Patients with early- or intermediate-stage HCC planned for locoregional therapy were prospectively enrolled. Baseline demographic and tumor information was collected and baseline and post-treatment 18F-FCH PET/CT performed. Maximum standardized uptake values (SUVmax) were determined for each HCC lesion, and the difference between baseline and post-treatment SUVmax values were compared with progression-free survival outcomes.
Results
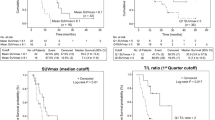
A total of 29 patients with 39 confirmed HCC lesions were enrolled from a single clinical center. Patients were mostly men (89.7%) with hepatitis C or alcohol-related cirrhosis (65.5%) and early-stage disease (89.7%). Per-patient and per-lesion sensitivity of 18F-FCH PET/CT was 72.4% and 59.0%, respectively. A baseline SUVmax < 13 was associated with a superior median progression-free survival compared with an SUVmax of > 13 (17.7 vs. 5.1 months; p = 0.006). A > 45% decrease in SUVmax between baseline and post-treatment 18F-FCH PET/CT (“responders”) was associated with a superior mean progression-free survival than a percentage decrease of < 45% (“non-responders,” 36.1 vs. 11.6 months; p = 0.034).
Conclusions
Baseline and post-treatment 18F-FCH PET/CT predicts outcomes in early-stage HCC undergoing locoregional therapy. This technique may identify patients with an objective response post-locoregional therapy who would benefit from further therapy.




Similar content being viewed by others


Abbreviations
- 18F-FCH PET/CT:
-
18F-fluorocholine positron emission tomography/computed tomography
- HCC:
-
Hepatocellular carcinoma
- SUVmax:
-
Maximum standardized uptake values
- EASL:
-
European Association for the Study of the Liver
- AFP:
-
Alpha fetoprotein
- mRECIST:
-
Modified Response Evaluation Criteria in Solid Tumors
- SIRT:
-
Selective internal radiotherapy
- 18F-FDG:
-
18F-fluorodeoxyglucose
- AASLD:
-
American Association for the Study of Liver Diseases
- BCLC:
-
Barcelona Clinic Liver Cancer
- TACE:
-
Transarterial chemoembolization
- SBRT:
-
Stereotactic body radiotherapy
- MRI:
-
Magnetic resonance imaging
- CT:
-
Computed tomography
- VOI:
-
Volume of interest
- 95% CI:
-
95% confidence interval
- NAFLD:
-
Nonalcoholic liver disease
References
Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136:E359–E386.
Global Burden of Disease Liver Cancer. The burden of primary liver cancer and underlying etiologies from 1990 to 2015 at the global, regional, and national level: results from the global burden of disease study 2015. JAMA Oncol. 2017;3:1683–1691.
Forner A, Reig M, Bruix J. Hepatocellular carcinoma. Lancet. 2018;391:1301–1314.
Goutte N, Sogni P, Bendersky N, et al. Geographical variations in incidence, management and survival of hepatocellular carcinoma in a Western country. J Hepatol. 2017;66:537–544.
Njei B, Rotman Y, Ditah I, Lim JK. Emerging trends in hepatocellular carcinoma incidence and mortality. Hepatology. 2015;61:191–199.
Wallace MC, Preen DB, Short MW, Adams LA, Jeffrey GP. Hepatocellular carcinoma in Australia 1982 to 2014: increasing incidence and improving survival. Liver Int. 2018;39:522–530.
Wallace MC, Preen D, Jeffrey GP, Adams LA. The evolving epidemiology of hepatocellular carcinoma: a global perspective. Expert Rev Gastroenterol Hepatol. 2015;9:765–779.
European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J Hepatol. 2018;69:182–236.
Mehta N, Heimbach J, Harnois DM, et al. Validation of a risk estimation of tumor recurrence after transplant (RETREAT) score for hepatocellular carcinoma recurrence after liver transplant. JAMA Oncol. 2017;3:493–500.
Sapisochin G, Goldaracena N, Laurence JM, et al. The extended Toronto criteria for liver transplantation in patients with hepatocellular carcinoma: a prospective validation study. Hepatology. 2016;64:2077–2088.
Lencioni R, Llovet JM. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis. 2010;30:52–60.
Vincenzi B, Di Maio M, Silletta M, et al. Prognostic relevance of objective response according to EASL criteria and mRECIST criteria in hepatocellular carcinoma patients treated with loco-regional therapies: a literature-based meta-analysis. PLoS One. 2015;10:e0133488.
Seyal AR, Gonzalez-Guindalini FD, Arslanoglu A, et al. Reproducibility of mRECIST in assessing response to transarterial radioembolization therapy in hepatocellular carcinoma. Hepatology. 2015;62:1111–1121.
Wang TH, Huang PI, Hu YW, et al. Combined Yttrium-90 microsphere selective internal radiation therapy and external beam radiotherapy in patients with hepatocellular carcinoma: from clinical aspects to dosimetry. PLoS One. 2018;13:e0190098.
Berriolo-Riedinger A, Becker S, Casasnovas O, Vander Borght T, Edeline V. Role of FDG PET-CT in the treatment management of Hodgkin lymphoma. Cancer Radiother. 2018;22:393–400.
Chowdhury FU, Bradley KM, Gleeson FV. The role of 18F-FDG PET/CT in the evaluation of oesophageal carcinoma. Clin Radiol. 2008;63:1297–1309.
Khan MA, Combs CS, Brunt EM, et al. Positron emission tomography scanning in the evaluation of hepatocellular carcinoma. J Hepatol. 2000;32:792–797.
Wu HB, Wang QS, Li BY, et al. F-18 FDG in conjunction with 11C-choline PET/CT in the diagnosis of hepatocellular carcinoma. Clin Nucl Med. 2011;36:1092–1097.
Hong G, Suh KS, Suh SW, et al. Alpha-fetoprotein and (18)F-FDG positron emission tomography predict tumor recurrence better than Milan criteria in living donor liver transplantation. J Hepatol. 2016;64:852–859.
Glunde K, Bhujwalla ZM, Ronen SM. Choline metabolism in malignant transformation. Nat Rev Cancer. 2011;11:835–848.
Bertagna F, Bertoli M, Bosio G, et al. Diagnostic role of radiolabelled choline PET or PET/CT in hepatocellular carcinoma: a systematic review and meta-analysis. Hepatol Int. 2014;8:493–500.
Talbot JN, Fartoux L, Balogova S, et al. Detection of hepatocellular carcinoma with PET/CT: a prospective comparison of 18F-fluorocholine and 18F-FDG in patients with cirrhosis or chronic liver disease. J Nucl Med. 2010;51:1699–1706.
Bieze M, Klumpen HJ, Verheij J, et al. Diagnostic accuracy of (18) F-methylcholine positron emission tomography/computed tomography for intra- and extrahepatic hepatocellular carcinoma. Hepatology. 2014;59:996–1006.
Chalaye J, Costentin CE, Luciani A, et al. Positron emission tomography/computed tomography with 18F-fluorocholine improve tumor staging and treatment allocation in patients with hepatocellular carcinoma. J Hepatol. 2018;69:336–344.
Bruix J, Sherman M. American association for the study of liver D management of hepatocellular carcinoma: an update. Hepatology. 2011;53:1020–1022.
Hardy LE, Hessamodini H, Wallace M, Francis R. Is FCH PET able to identify foci of infection superiorly to FDG PET? BMJ Case Rep 2017; 2017.
Mazzaferro V, Regalia E, Doci R, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996;334:693–699.
Yao FY, Ferrell L, Bass NM, et al. Liver transplantation for hepatocellular carcinoma: expansion of the tumor size limits does not adversely impact survival. Hepatology. 2001;33:1394–1403.
Treglia G, Giovannini E, Di Franco D, et al. The role of positron emission tomography using carbon-11 and fluorine-18 choline in tumors other than prostate cancer: a systematic review. Ann Nucl Med. 2012;26:451–461.
Lencioni R, Montal R, Torres F, et al. Objective response by mRECIST as a predictor and potential surrogate end-point of overall survival in advanced HCC. J Hepatol. 2017;66:1166–1172.
Gogoi-Tiwari J, Kohn-Gaone J, Giles C, et al. The murine choline-deficient, ethionine-supplemented (CDE) diet model of chronic liver injury. J Vis Exp. 2017;128:e56138.
Raoul JL, Gilabert M, Piana G. How to define transarterial chemoembolization failure or refractoriness: a European perspective. Liver Cancer. 2014;3:119–124.
Sieghart W, Hucke F, Pinter M, et al. The ART of decision making: retreatment with transarterial chemoembolization in patients with hepatocellular carcinoma. Hepatology. 2013;57:2261–2273.
Acknowledgments
The authors would like to thank Elaine Campbell for her help with study management and data collection.
Funding
This study was funded in part by the Cancer and Palliative Care Research and Evaluation Unit Small Grants Scheme of the University of Western Australia and a research grant from the Australian and New Zealand Society of Nuclear Medicine. The sponsors had no role in the conduct of the research; study design; collection, analysis and interpretation of data; writing of the manuscript; or decision to submit the article for publication.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
They authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Wallace, M.C., Sek, K., Francis, R.J. et al. Baseline and Post-treatment 18F-Fluorocholine PET/CT Predicts Outcomes in Hepatocellular Carcinoma Following Locoregional Therapy. Dig Dis Sci 65, 647–657 (2020). https://doi.org/10.1007/s10620-019-05781-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-019-05781-6