
Abstract
Purpose
This study delves into the combined cognitive bias hypothesis in depression, exploring the interaction between negative attention, interpretation and memory biases. We aimed to assess whether modifying attention and interpretation bias would lead to congruent changes in memory bias, and to what extend and depth this causal effect can be.
Method
Ninety-nine undergraduates underwent either a positive (PT) or negative (NT) four-day attention and interpretation bias training. A set of well-established post-training assessments including free recall, recognition, autobiographic memory, and self-reference encoding tasks were used to evaluate memory bias. Affective states were measured pre- and post-training.
Results
Compared to PT, participants in NT correctly retrieved more negative trained stimuli, and falsely recognized more negative synonyms of trained terms. NT also exhibited an enhanced retrieval of negative autobiographical memory. No significant differences were found between NT and PT in self-referential encoding and retrieval bias, or affective states.
Discussion
The results suggested an extensive and strong transfer effect from attention and interpretation bias modification to different facets of memory bias, being found in retrieving trained emotional stimuli, in memory intrusion of negative synonyms, and in autobiographic memory recall. The findings underscored the causality between three biases, supporting the combined cognitive bias hypothesis. It might also suggest an effective new approach to modify memory bias via attention and interpretation bias training.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Depression, as underscored by cognitive theories and empirical evidence, is marked by emotional cognitive biases. This suggests a preference for processing negative information over neutral or positive information (for a review, see Mathews & MacLeod, 2005; Gotlib & Joormann, 2010; LeMoult & Gotlib, 2019). Individuals with depression tend to allocate attention to negative rather than positive or neutral information (attention bias; Peckham et al., 2010), interpret emotionally ambiguous situations negatively (interpretation bias; Wisco & Nolen-Hoeksema, 2010), and recall negative information more easily and frequently compared to positive or neutral information (memory bias; Matt et al., 1992; Williams et al., 2007; Everaert et al., 2022). Empirical research underscores that these biases are not merely characteristics of depression, but actively contribute to the onset and development of its symptoms (Sumner et al., 2010; Wells & Beevers, 2010; Blackwell & Holmes, 2010).
These studies offer a detailed understanding of the role of each bias in depression. However, they often overlook the potential interplay among the three biases, crucial for understanding the complex cognitive underpinnings of depression. Cognitive models of depression (Beck, 2008; Clark et al., 2000; Ingram, 1984; Williams et al., 1988; Joormann, 2007, 2010), along with the Combined Cognitive Bias Hypothesis (Hirsch et al., 2006; Everaert et al., 2012), postulate a deeply interconnected relationship between attention, interpretation, and memory biases. These biases are suggested to be correlated and interactive, collectively influencing depression. It is emphasized that specific negative cognitive biases can act as catalysts, exerting influence over other biases and intensifying their negative nature. Notably, memory biases are posited to be influenced by earlier processes of attention and interpretation (Ingram, 1984; Williams et al., 1988; Joormann, 2007, 2010). That is, prolonged focus on negative information (attributed to attention bias) and in-depth negative analysis (arising from interpretation bias) enhance the encoding of such negative information, subsequently boosting its retrieval (manifesting as memory bias). Exploring this causal pathway aspires to both augment and refine our understanding of the cognitive underpinnings of depression. This holistic perspective could set the stage for developing interventions that are both precise and adept at targeting the most initial and foundational cognitive biases.
To our surprise, only a few studies have delved into these proposed causal relationships. These investigations often employ Cognitive Bias Modification methods (CBM; for a review, see Hertel & Mathews, 2011) to modify targeted cognitive biases, then assess the subsequent transfer effects on other biases through established cognitive bias assessments. For instance, three studies (Tran et al., 2011; Joormann et al., 2015; Salemink et al., 2010) trained participants to consistently interpret ambiguous scenarios in either a negative or positive manner. Subsequent memory bias assessment involved participants freely recalling the scenarios they had previously interpreted. Findings from these studies highlighted better recall for scenarios interpreted in a manner aligned with the training condition, implying a causal influence of interpretation bias modification on memory bias. Other studies utilized attention bias modification. Participants were randomized into two training conditions: one group received a task directing their attention away from negative stimuli, while the other group participated in a task that intentionally oriented them towards negative stimuli (Daches et al., 2019), or a placebo task (Woolridge et al., 2021; Blaut et al., 2013). Memory bias was assessed by viewing and recalling a set of emotionally charged words or pictures. The results revealed that those trained to divert attention from negative stimuli exhibited a reduced recall of negative stimuli in the memory bias assessment, suggesting a causal effect from attention to memory bias.
While current studies provide insights into the impact of attention and interpretation training on memory bias, the exploration has been relatively circumscribed. Firstly, the existing literature tends to focus on the isolated impact of either attention or interpretation bias on memory bias. This approach potentially neglects the intricate interactions among the three biases, as highlighted by Everaert et al. (2012). An unexamined bias might potentially influence the outcomes, leading to an incomplete understanding of the observed interactions. For a more comprehensive understanding of how these biases interact, it is important to employ a design examining all three concurrently, shedding light on their causal effects.
Secondly, existing research primarily evaluates participants’ ability to recall specific emotional stimuli they were directly exposed to during experiments, indicating a causal effect on memory bias limited to the immediately processed experimental context. This narrow focus raises pivotal questions about the scope of memory bias influenced by attention and interpretation training: Does the transformation in memory bias remain constrained within the parameters of the experiment? Is there a more extensive memory bias, exhibiting an enhanced recall of emotional content embedded in participants’ personal narratives? For example, studies could explore whether participants, in line with their training, recall a greater volume of emotional content from their personal lexicon, and even draw upon recalling real-life events with similar emotional undertones. Affirmation of this would signify a memory bias transformation that not only transcends the constrained boundaries of the experimental context but also infiltrates deeper realms, influencing memory intrusions and autobiographical recollections. This could lead to a better understanding of the pervasive impacts of attention and interpretation bias training on memory bias.
Another important aspect of memory bias is the enhancing effect of self-referential information in biased encoding and retrieval. Self-referential memory bias is deeply rooted in cognitive self-schemas (Strube et al., 1986; Dobson & Shaw, 1987)—latent memory-based knowledge structures that develop during childhood and reflect one’s beliefs and generalizations about oneself (Markus, 1977). Does modification of attention and interpretation bias also affect selective self-referent memory bias? Unpacking this would not only illuminate the profound causal impact of attention and interpretation bias on memory bias but also provide a first lead on the possible modification of underlying self-schemas.
The present study explored the scope and depth of the potential causal effect of attention and interpretation bias on memory bias. We employed the mouse-based contingent attention training (MCAT; Sanchez-Lopez et al., 2019), a CBM task established for its efficacy in modifying and measuring attention and interpretation biases (Sanchez-Lopez et al., 2019; Blanco et al., 2023). This unified design, which incorporated both attention and interpretation biases into one training task, could avoid the error variance associated with applying multiple training tasks (e.g., stimuli consistency across tasks, operating sequence of tasks). Moreover, this integrated approach, targeting two biases together, is anticipated to yield pronounced transfer effects on memory bias, providing insights into the extent and depth of the transfer effect on memory biases.
Following the training, a set of well-established memory bias assessments was applied. Consistent with earlier studies, our initial step was to examine the free recall of the emotional stimuli used in MCAT training. This aimed to assess whether information processed at the stages of attention and interpretation would be more effectively recalled. Following this, we implemented a recognition task to evaluate participants’ tendency to falsely recall unexposed emotional stimuli. For example, an individual may falsely recognize certain information as familiar not because it was encountered during MCAT training, but due to its resemblance to something that aligns with their preexisting beliefs, leading to false recognition. The autobiographical memory test was used to evaluate recall tendencies toward real-life events, while the self-referential encoding and incidental recall task assessed memory bias related to self-relevant emotional words (For a detailed methodological illustration, refer to Method 2.4). We hypothesized a congruence between the training (positive or negative) and subsequent memory biases across all evaluations. Confirmation of this hypothesis would underscore a significant, far-reaching causal impact of attention and interpretation biases on memory bias, enhancing our understanding of their interactive dynamics.
Method
Participants
This study received approval from the Ethics Committee of the Faculty of Social Science at Radboud University and was preregistered at aspredicted (https://aspredicted.org/SDG_45T). Since it’s the first time to assess the transfer effect from MCAT to memory bias, there was no existing data to precisely estimate the required sample size from previous studies. Therefore, we referred to standard practices in MCAT to estimate the required power. Based on a previous study using MCAT (Sanchez-Lopez et al., 2019), we calculated an observed effect size for attention bias (i.e., disengagement from positive to negative stimuli), yielding a Cohen’s d value of 0.51. A t-test power analysis with G*Power (Faul et al., 2007) indicated that a sample size of 49 participants per group would be necessary to achieve a power of 0.8, assuming an alpha level of 0.05. Accordingly, we aimed to recruit a minimum of 98 participants.
Participants were recruited via the SONA participant system of Radboud University. All participants provided informed consent prior to their participation. Upon completion of the study, they received either 2.5 to 3 course credits or financial compensation ranging from €25 to €30, depending on the time spent of their participation. Inclusion criteria required participants to be native Dutch speakers, as the experimental materials were presented in Dutch. Individuals scoring 28 or higher on the Beck Depression Inventory-II (BDI-II; Beck et al., 1996; Dutch version: Does, 2002) were excluded to avoid potential harm to individuals with severe depression symptoms. This selection criterion, along with the fact that participants primarily exhibited mild depressive symptoms, allowing for the manipulation of targeted cognitive biases towards positive versus negative, thereby enabling an examination of the subsequent transfer effects on memory bias.
Participants were randomly assigned to either the Positive Training (PT) or Negative Training (NT) condition. Fifty participants completed the first and last day of the experiment sessions in a laboratory setting, while the two in-between days were conducted online (lab setting). However, due to university laboratory closures amid the Covid-19 pandemic, the subsequent half of our participants completed the entire four-day experiment online, facilitated by video calls between them and the research team (online setting). The lab setting experiment began in May 2019, shifted to an online setting in December 2020, and was completed in March 2021. There was one participant dropped out from the online setting, resulting in a final sample of 99 participants (80 female; age M = 21.58, SD = 4.48; BDI-II M = 7.43, SD = 6.96), with fifty in PT and forty-nine in NT. These conditions were balanced across both the lab setting (NPT = 23, NNT = 27) and online setting (NPT = 27, NNT = 22).
Questionnaires
Beck Depression Inventory-II
The BDI-II measured the severity of depressive symptoms with 21 items rated on a scale from 0 to 3. This questionnaire is a widely used measure to assess depression, with high levels of reliability and validity in non-clinical samples (Storch et al., 2004). The internal consistency in this study was α = 0.90.
Anxiety Sensitivity Index
The Anxiety Sensitivity Index (ASI; Reiss et al., 1986; Dutch version: Vujanovic et al., 2007) is a self-report questionnaire designed to assess anxiety sensitivity. The questionnaire consists of 16 items with answer possibilities ranging on a five-point Likert scale from 1 (barely) to 5 (very much). A sum score of all items was used to index the level of anxiety sensitivity. This questionnaire has good reliability and validity among non-clinic samples (Vujanovic et al., 2007). The internal consistency in the present study was α = 0.88.
Brief State Rumination Inventory
The Brief State Rumination Inventory (BSRI; English and Dutch version: Marchetti et al., 2018) is a self-report questionnaire that assesses state rumination. The questionnaire consists of 8 items with answer possibilities that could be indicated on a slide ranging from 0 (totally disagree) to 100 (totally agree). A sum score was used to indicate the level of state rumination. It is a reliable and valid measure to assess state rumination in undergraduate samples (Marchetti et al., 2018). The internal consistency in this study was α = 0.90.
Positive and Negative Affect Schedule
The Positive and Negative Affect Schedule (PANAS; Watson et al., 1988; Dutch version: Engelen et al., 2006) is a self-report questionnaire that consists of 20-item scales to measure both positive and negative affect. Ten items assessed the positive affect, and another 10 items assessed the negative affect. Each item is rated on a five-point Likert scale ranging from 1 (not at all) to 5 (very much). The sum score was calculated separately for positive affect and negative affect subscales. These measures have proven to be reliable within non-clinical populations (Crawford & Henry, 2004). The internal consistency in this study was α = 0.83.
Mood States Rating
Before and after each attention and interpretation bias training session, participants were asked to rate their mood states on a visual analog scale with 9 points ranging from 1 (not at all) to 9 (very much). The positive and negative moods were assessed separately as they represented different dimensions (Watson & Tellegen, 1985).
Intervention: Mouse-Based Contingent Attention Training (MCAT)
Participants completed four sessions of MCAT over four consecutive days. As depicted in Fig. 1, each MCAT session comprised two phases: a baseline assessment phase and a modification phase. The MCAT assessment phase assessed participants’ pre-training attention and interpretation biases. Participants were presented with a 6-word long emotional scrambled sentence (e.g., “born loser a I winner was”). They could freely view and unscramble the sentence to form a grammatically correct and meaningful statement, either positively or negatively (“I was born a winner” or “I was born a loser”), by excluding one of the two emotional target words (“winner”, “loser”). The assessment included 12 trials, all describing a self-relevant situation allowing for both positive and negative interpretations. A mouse-contingent moving window technique (Sanchez-Lopez et al., 2019) monitored attention to each word. We recorded the attention duration on positive and negative target words and the number of correctly constructed positive and negative sentences. Consistent with a previous study (Sanchez-Lopez et al., 2019), the following formulas were used to calculate attention and interpretation biases:

Schematic presentation of the MCAT procedure
After the MCAT baseline assessment phase, participants underwent the MCAT modification phase, consisting of 8 training blocks, each containing 6 trials. The training intentionally regulated participants’ attention allocation towards positive or negative words and facilitated congruent interpretations, based on their assigned training condition (PT or NT). The procedure was similar to the assessment but with several manipulations. First, participants received online gaze-contingent feedback on their attentional performance during the reading section. Specifically, a blue or yellow square framed the positive or negative words. Participants in PT were instructed to pay attention to the blue-framed word and use it to construct a sentence, while those in NT were instructed to use the yellow-framed word. Second, participants’ performance was computed and presented to them after each training block (e.g., the proportion of attention duration on blue over yellow words and sentences constructed using blue over yellow words). Participants could compare their actual performance to ensure they were regulating their attention and interpretation according to their training condition.
The four MCAT sessions utilized different stimuli, totaling 4 sessions x 12 trials for baseline stimuli and 4 sessions x 48 trials for training stimuli across all sessions. To ensure that the order of the trials did not affect participants’ performance on later memory bias assessment, the order of the trials in both the baseline assessment and modification phases was randomized across participants and conditions. Additionally, to counterbalance any potential order effects, the four training sessions (sessions A, B, C, and D) were presented to participants in a counterbalanced order. Participants received one of four different training orders during their four training days: ABCD, BCDA, CDBA, or DABC. The split-half reliability coefficient of the MCAT assessment at baseline was commendable, with coefficients of 0.63, 0.98, 0.70, and 0.78 for sessions A, B, C, and D, respectively. It is important to note that the counterbalance of the session order and the randomization of trial orders might potentially reduce the reliability estimates we could obtain.
Transfer Measures to Memory Bias
Free Recall MCAT Stimuli
Participants were instructed to recall as many of the blue squared (positive) and yellow squared (negative) words they had been exposed to during the previous four days of MCAT training. Participants were given an unlimited amount of time to type in the words they remembered. Spelling errors were permitted. Conform previous research (Everaert et al., 2014), we calculated the free recall bias as such: The number of correctly recalled negative MCAT words was divided by the total number of correctly recalled positive and negative MCAT words. This free recall bias score served as an index of the participant’s ability to recall negative relative to positive trained stimuli.
Recognition MCAT Trained and new Stimuli
A recognition task was implemented at the post-training assessment. The task consisted of 128 words; each was presented for 5 s. Participants were instructed to indicate whether they had seen the presented word during the past four days of MCAT training. They had 8 s to give a response by pressing either “J” for “yes” or “F” for “no” on the keyboard.
The 128 stimuli consisted of three types of words: (a) MCAT emotional words which were trained to process; (b) new emotional words that were synonyms of the MCAT emotional words (e.g., using “joyful” instead of “cheerful”) which were never presented during the training; and (c) new words that had similar looking to the MCAT emotional words but had a neutral meaning (e.g., using “complement” instead of “compliment”), and had never been shown during the training. This structure of stimuli not only assessed the participants’ recognition bias on the trained MCAT emotional words, but also probed for any potential training-congruent false recognition of relevant yet never-seen stimuli such as synonyms and similar-looking words. The task contained 64 MCAT emotional training stimuli (32 of positive and 32 negative), and 64 new stimuli comprising 32 synonyms (16 negative and 16 positive), and 32 similar-looking words (derived from 16 negative and 16 positive MCAT training words). The order of the words was fixed, with the restriction that no more than two words of the same emotion would be presented consecutively. This was done to prevent any potential biases that may have arisen from the order of presentation.
Recognition bias was separately computed for the MCAT emotional words, synonyms, and similar-looking words. Mirroring the approach in the free recall task, recognition bias for the MCAT emotional target words was determined by dividing the number of recognized negative MCAT words by the cumulative count of both recognized positive and negative MCAT words. The same formula was applied to calculate the false recognition bias concerning synonyms and similar-looking words.
Autobiographical Recall Task
Following each MCAT training session, participants undertook an autobiographical recall task (hence conducted four times in total). Participants were asked to recall and type in the description of a personal event from the previous day that evoked an emotional feeling. To determine the valence of the recalled events, two researchers, blind to the study’s conditions, independently evaluated them using a 9-point scale, ranging from 1 (very negative) to 9 (very positive). This method aligns with procedures employed in prior research (Visser et al., 2020). For each event, an average score derived from the two independent ratings was computed. In this study, inter-rater reliability was outstanding, evidenced by an alpha coefficient of 0.95. To calculate autobiographical memory bias, an overall mean score from the four events was determined for each participant.
The Self-Referential Encoding and Incidental Recall Task
The self-referential encoding and incidental recall task (SRET; Gotlib et al., 2004) was performed at post-training assessment. It was used to evaluate explicit memory biases for emotional words that are relevant to the self and were incidentally learned. During the SRET, participants were shown a series of 24 adjectives (12 negative and 12 positive) one at a time for 8 s each. The words were chosen from the Dutch translation of the Affective Norms for English Words (ANEW; Bradley & Lang, 1999). To make the encoding self-referential, participants were asked to indicate whether each word described themselves by pressing either the J (yes) or F (no) key on the keyboard during the display. After the encoding phase, participants completed a brief non-verbal distraction task, comprising Raven matrices and simple math calculations. Then, they were asked to recall as many words as possible from the previous computer task within three minutes. Spelling errors were permitted.
To calculate the SRET bias, the number of correctly recalled negative words that were endorsed as self-relevant was divided by the total number of correctly recalled positive and negative words that were endorsed as self-relevant. This calculation was done in line with the method used by Gotlib et al. (2004).
Procedure
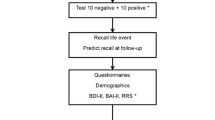
Figure 2 provides an overview of the experimental procedure. Before engaging in the study, all participants completed the BDI-II as prescreening. On the first experiment day, participants provided their informed consent and then proceeded to complete the questionnaires including ASI, BSRI, and PANAS, culminating in the first MCAT session. On both the subsequent second and third experimental days, participants undertook the respective MCAT sessions. On the fourth experiment day, participants completed the final MCAT session, which was then followed by the post-test assessment encompassing the PANAS, the free recall task, the recognition task, and the SRET. The autobiographical recall task was executed after each MCAT session. Before and after every MCAT session, participants assessed their positive and negative mood states.

Experiment procedure
Statistical Analyses
We used independent t-tests to compare the demographic and baseline variable differences between PT and NT groups. This encompassed age, gender, depression symptoms, anxiety sensitivity, state rumination, as well as initial attention and interpretation biases, which were assessed on the first experiment day before the commencement of the MCAT training.
To check if the attention and interpretation bias were successfully manipulated in the trained directions, we implemented independent t-tests comparing attention and interpretation bias assessed on the last training day, represented the post-training metrics. As the study’s main interest was to assess the transfer effect from MCAT to memory bias, independent t-tests were conducted to compare the difference between the PT and NT on the post-training assessments of memory bias including free recall bias, recognition biases, SRET bias, and autobiographic recall bias.
To examine the impact of MCAT training on positive and negative affect and mood states, our first step was to employ repeated measures ANOVAs for the data of PANAS, based on a 2 (conditions: PT, NT) × 2 (times: pre- and post-training) design. Subsequently, we applied independent t-tests to compare the positive and negative mood states assessed before and after each training session, between PT and NT.
As mentioned before, the experiment was carried out in both lab and online environments due to COVID-19 restrictions. To account for potential variances between these two settings, we employed an independent t-test to analyze differences in baseline variables including demographics, symptomatology, symptoms, attention and interpretation biases at baseline. Moreover, to assess the potential difference on the MCAT training impact on attention, interpretation, and memory bias between lab setting and online setting, we executed a 2 (conditions: PT, NT) × 2 (settings: lab setting, online setting) ANOVA. For this analysis, the data was drawn from attention and interpretation bias evaluated on the fourth training day, as well as free recall and autobiographical recall biases.
All statistical analyses were performed using SPSS. For the t-tests, we reported effect sizes in terms of Cohen’s d (where d: 0.2 signifies a small effect; 0.5 indicates a medium effect; and 0.8 represents a large effect). For ANOVAs, effect sizes were documented in terms of partial eta square (ƞp2: 0.01 = small effect; 0.05 = medium effect; 0.16 = large effect). Greenhouse-Geisser’s procedure was used to correct the degrees of freedom when sphericity was violated in the ANOVAs. The complete dataset, analysis scripts, and study materials can be accessed through the Radboud Data Repository (https://doi.org/10.34973/5pck-pz44).
Results
Sample Characteristics
Table 1 presents the comparison of demographics and baseline variables between the PT and NT conditions. The PT did not significantly differ from the NT in terms of age, gender identification ratio, (χ2 = 0.21, p = .351), depression symptoms, anxiety sensitivity, state rumination, or baseline attention or interpretation bias. This means that both conditions had similar characteristics in these areas at the start of the study.
Manipulation Check
The attention and interpretation bias assessed on the fourth training day were compared between PT and NT. As shown in Table 2, participants in the NT exhibited stronger negative attention and interpretation biases compared to the PT at post-training, indicating that the attention and interpretation bias was manipulated successfully in the training direction.
Transfer Effect on Memory Bias
As shown in Table 2, we compared memory bias indices between the PT and NT, encompassing free recall bias, recognition bias, autobiographical recall bias, and SRET bias. Frist, participants in NT were observed to recall and recognize a higher ratio of negative MCAT emotional words than those in PT. Moreover, compared to PT, the NT group falsely recognized more negative synonyms as previously encountered. However, no statistically significant differences were detected between the two training conditions when it came to falsely recognizing similar-looking words. Notably, a pronounced training-congruent bias in autobiographical memory emerged: NT participants recalled real-life events more negatively than PT. However, it should be noted that there was no discernible difference between NT and PT concerning SERT performance. Both groups recalled a comparable proportion of negative words.
These results highlighted the causal effects of attention and interpretation bias modification on different facets of memory bias, including the retrieval of trained emotional stimuli, relevant but new emotional stimuli, and real-life events. However, they also exposed the limited transfer effect on SRET bias. These important results were discussed in turn.
Transfer Effect on Affect and Mood State
Positive and Negative Affect Assessed by PANAS
The repeated ANOVA on the positive affect outcomes did not show a significant main effect of training condition (F(2,87) = 0.04, p = .847, ƞp2 < 0.001), nor time (F(20,88) = 0.56, p = .455, ƞp2 = 0.006), nor a condition × time-interaction (F (83,52) = 2.25, p = .137, ƞp2 = 0.024). Similarly, as for negative affect, no significant main effects of condition (F (58,60) = 1.40, p = .240, ƞp2 = 0.015), nor time (F (14,67) = 0.97, p = .328, ƞp2 = 0.010), nor a condition × time-interaction (F (3,35) = 0.22, p = .639, ƞp2 = 0.002) were found.
Positive and Negative Mood State
As depicted in Fig. 3, after each training session, the positive mood was uplifted in PT and declined in NT, while the opposite pattern was observed for negative mood. This trend indicates that mood changes align with the training condition after each session. However, this effect was relatively weak. First, the mood state consistently reverted to its initial level at the start of the subsequent experiment day, before the onset of a new training session. Second, the impact of training on mood state appeared to diminish across sessions. The post-session positive mood was significantly different between PT and NT only in the first three sessions, while the post-session negative mood showed a significant difference only in the first two sessions.

Positive and negative mood changes across 4 sessions in two conditions
Overall, these results suggest that the MCAT training had a limited effect on affect and mood changes. Detailed descriptions and t-test comparisons of the pre- and post-training PANAS scores, as well as the pre- and post-session positive and negative mood, between PT and NT, can be found in the supplement.
Comparing the Lab and Online Experiment Settings
As detailed in Table 3, we compared the sample characteristics between participants in the lab setting and online setting. There were no significant differences on gender ratio (χ2 = 3.01, p = .083), depressive symptom levels, or baseline attention and interpretation biases. Nevertheless, notable differences emerged in age, anxiety sensitivity, and state rumination. Participants who undertook the online setting (during the onset of COVID-19 pandemic) were younger and displayed higher levels of anxiety sensitivity and state rumination compared to those who participated in the lab setting (before the onset of COVID-19 pandemic).
The two-way ANOVA (2 conditions x 2 experimental settings) for the MCAT training effect indicated no main effect of the experiment settings on attention bias (F (427,86) = 1.43, p = .235, ƞp2 = 0.015), nor interpretation bias (F (427,86) = 1.43, p = .235, ƞp2 = 0.015). The transfer effect was found not significant on free recall bias (F (6,57) = 0.03, p = .867, ƞp2 = 0), nor autobiographic recall bias (F (0.61) = 0.51, p = .477, ƞp2 = 0.006). The results indicated that the MCAT training effect did not differ between lab and online experiment settings.
Discussion
Our findings provide compelling evidence supporting the causal effects of attention and interpretation bias training on diverse aspects of memory bias. Specifically, we observed a training-congruent memory bias in recalling MCAT emotional stimuli that were trained to process, in falsely recognizing unexposed emotional stimuli as seen before, and in recalling emotional life events from autobiographical memory. However, the MCAT training effect did not transfer to self-referential encoding and recall. These results extend our understanding of this causal effect by revealing the extent and depth of the transfer effect. These results were discussed in turn.
The first foundational discovery is the presence of a training-congruent memory bias concerning the recall and recognition of MCAT emotional training stimuli. This finding aligns with existing literature (Tran et al., 2011; Joormann et al., 2015; Salemink et al., 2010), suggesting a causal relationship between attention and interpretation bias and memory bias when processing the same information. This phenomenon can be attributed to the MCAT training that necessitated heightened attention towards target stimuli, fostering deep engagement and analysis on this information to arrive at a congruent interpretation. This, in turn, facilitated congruent encoding and subsequent retrieval of specific information.
Further enriching the findings, our data revealed a generalized memory bias wherein NT group exhibited a proclivity to falsely recognized more negative synonyms (of MCAT emotional stimuli) as seen before, even if they weren’t exposed to these stimuli before. The presence of this false recognition bias suggests that heightened attention and interpretation on specific stimuli might induce memory intrusions for related content. Interestingly, this effect wasn’t present when participants recognized another type of new stimuli: the similar looking, yet emotionally neutral words, generated from MCAT emotional stimuli. This phenomenon finds resonance with existing literature emphasizes the role of emotional congruence in memory retrieval (Matt et al., 1992; Everaert et al., 2013, 2014, 2017). It’s possible that this generalized memory bias was specific to those stimuli that had the same emotional valence as the information processed at earlier stages (i.e., attention and interpretation). Another interpretive angle emerges from the examination of the encoding mechanisms. Previous research has demonstrated that memory recall benefits from two processes during learning: semantic processing and perceptual processing (Hyde & Jenkins, 1969; Craik & Tulving, 1975; Craik & Lockhart, 1972; Belmore, 1981; Brown & Lloyd-Jones, 2006). Within our study’s framework, semantic processing appears dominant during attention and interpretation process. Thus, participants likely emphasized the inherent meanings (i.e., synonym), over the superficial visual aspects (i.e., similar-looking words) of the stimuli during recognition. These results provide detailed insight into how the processing bias on specific information at stage of attention and interpretation regulated the later memory process: the information with inherent meaning and emotional valence being better encoded in and retrieved from memory.
Notably, we also observed a transfer effect from attention and interpretation bias training to emotional autobiographical memory retrieval, marking a significant expansion on existing knowledge. This indicates that the influence of the attention and interpretation process extends beyond the recall of experimentally prepared lexical materials to encompass real-life events stored in autobiographical memory. One plausible explanation for this phenomenon is that participants, through repeated engagement in constructing self-relevant positive or negative scenarios during attention and interpretation bias training, activated latent memory schemas. To illustrate, constructing a sentence such as “I was born a loser” might have activated underlying dysfunctional schemas about failure and helpless, in turn facilitating access to autobiographical memories such as “I tripped on stage during my solo show, audience were gasping and whispering”. Emotional autobiographical memory is inherently tied to an individual’s past experiences and, importantly, the emotional tone attached to those experiences (Holland & Kensinger, 2010). Our observations suggest that modifications in attention and interpretation biases might have the potential to reshape the way individuals recall their personal histories. This has profound implications, especially in the context of therapeutic approaches for individuals who suffer from negative recollections of past events.
Yet, these findings support both near and far transfer effect on memory bias, extending from the retrieval of trained stimuli to the occurrence of false memory intrusions and the broader recall of autobiographical memories. These results together suggest the potential therapeutic advantages of addressing negative memory bias through training in attention and interpretation biases. It should be noted that while there have been attempts to develop effective modification directly targeting memory bias, only a few of them found the expected results (but see, Vrijsen et al., 2019; Visser et al., 2020). Considering the well-documented foundational role of memory biases in depression (Matt et al., 1992; Watkins et al., 1992; Evereart et al., 2022), such an approach might be instrumental in alleviating associated symptoms. Additionally, as our study highlights a causal interconnection between attention, interpretation, and memory biases, it advocated for a holistic cognitive bias modification approach. Such an integrated method, targeting multiple interacted biases, may pave the way for more effective interventions in emotional disorders.
Contrary to prior research suggesting a transfer effect on encoding and retrieving new emotional stimuli (Blaut et al., 2013; Daches et al., 2019; Woolridge et al., 2021), our data did not align. We found no significant differences in SRET performance between the PT and NT groups, raising questions about the assertion that modifying attentional behaviors, especially in directing attentional resources towards specific stimuli, influences the way of encoding (Blaut et al., 2013; Daches et al., 2019). This lack of alignment could be attributed to the intrinsic role of self-schema in SRET. SRET performance relies on how congruent stimuli are with one’s established self-beliefs and -reference in line with one’s schemata (Strube et al., 1986; Dobson & Shaw, 1987; Markus, 1977; Derry & Kuiper, 1981). Given the enduring nature of these self-schema, it’s conceivable that the MCAT training was insufficient in precipitating any significant shifts in these deeply rooted cognitive structures—self schemata, leading to an absence of training-congruent modifications in the SRET. It should be mentioned that NT recalled slightly more negative words than PT during SRET, though the effect was marginal (d = -0.22). This suggests the potential for more intensive MCAT training to exert a stronger influence on the encoding and retrieval of self-referent emotional content.
Furthermore, the MCAT training only had a subtle impact on emotional affect and mood states. Our participants were primarily healthy, processing strong mood repair capabilities (Diener et al., 2015). The potential benefits of PT might have reached a ceiling effect, making them less noticeable. Meanwhile, any detrimental mood shifts from NT might have been rapidly counteracted. Such outcomes imply that the transfer effects of attention and interpretation bias on memory bias were not merely due to fleeting mood changes, but rather underpinned by shifts in information processing tendencies and more profound cognitive dynamics.
Several limitations should be noted. First, owing to the Covid-19 pandemic, data was collected both in lab and online settings, introducing a possible confound to our study. Participants in the online setting exhibited a higher degree of state rumination in comparison to their counterparts who were in the lab setting before the pandemic, which is consistent with previous research highlighting the psychological impact of the pandemic (Elbay et al., 2020; Salari et al., 2020; Varma et al., 2021). However, key baseline variables such as depression symptoms and cognitive biases, as well as the training effect on attention, interpretation and memory biases, remained consistent across two settings. This consistency implies that MCAT training is adaptable outside lab conditions, providing a practical tool for cognitive bias interventions. Recent work by Blanco et al. (2023) also indicated the efficacy of online MCAT in reducing cognitive biases and related symptoms. Second, the composition of our sample primarily consists of undergraduates, with a predominant representation of females, relatively young, highly educated and mostly white, which might limit the generalizability of the research findings. For future research, it is advisable to assess the applicability of these findings in a more diverse population.
Despite these constraints, our research highlights a strong and extensive causal effect from attention and interpretation bias to memory bias. This finding bolsters existing cognitive models and the CCB, providing clinical implications on the interventions. Future research focusing on the interrelationships among cognitive biases will benefit from the insights presented in this study.
References
Beck, A. T. (2008). The evolution of the cognitive model of depression and its neurobiological correlates. American Journal of Psychiatry, 165(8), 969–977.
Beck, A. T., Steer, R. A., & Brown, G. (1996). Beck depression inventory–II. Psychological assessment.
Belmore, S. M. (1981). Imagery and semantic elaboration in hypermnesia for words. Journal of Experimental Psychology: Human Learning and Memory, 7(3), 191.
Blackwell, S. E., & Holmes, E. A. (2010). Modifying interpretation and imagination in clinical depression: A single case series using cognitive bias modification. Applied Cognitive Psychology: The Official Journal of the Society for Applied Research in Memory and Cognition, 24(3), 338–350.
Blanco, I., Boemo, T., Martin-Garcia, O., Koster, E. H., De Raedt, R., & Sanchez-Lopez, A. (2023). Online contingent attention training (OCAT): Transfer effects to cognitive biases, rumination, and anxiety symptoms from two proof-of-principle studies. Cognitive Research: Principles and Implications, 8(1), 1–19.
Blaut, A., Paulewicz, B., Szastok, M., Prochwicz, K., & Koster, E. (2013). Are attentional bias and memory bias for negative words causally related? Journal of Behavior Therapy and Experimental Psychiatry, 44(3), 293–299.
Bradley, M. M., & Lang, P. J. (1999). Affective norms for English words (ANEW): Instruction manual and affective ratings (Vol. 30, No. 1, pp. 25–36). Technical report C-1, the center for research in psychophysiology, University of Florida.
Brown, C., & Lloyd-Jones, T. J. (2006). Beneficial effects of verbalization and visual distinctiveness on remembering and knowing faces. Memory & Cognition, 34(2), 277–286.
Clark, D. A., Beck, A. T., Alford, B. A., Bieling, P. J., & Segal, Z. V. (2000). Scientific foundations of cognitive theory and therapy of depression.
Craik, F. I., & Lockhart, R. S. (1972). Levels of processing: A framework for memory research. Journal of Verbal Learning and Verbal Behavior, 11(6), 671–684.
Craik, F. I., & Tulving, E. (1975). Depth of processing and the retention of words in episodic memory. Journal of Experimental Psychology: General, 104(3), 268.
Crawford, J. R., & Henry, J. D. (2004). The positive and negative affect schedule (PANAS): Construct validity, measurement properties and normative data in a large non-clinical sample. British Journal of Clinical Psychology, 43(3), 245–265.
Daches, S., Mor, N., & Hertel, P. (2019). Training to inhibit negative content affects memory and rumination. Cognitive Therapy and Research, 43(6), 1018–1027.
Derry, P. A., & Kuiper, N. A. (1981). Schematic processing and self-reference in clinical depression. Journal of Abnormal Psychology, 90(4), 286.
Diener, E., Kanazawa, S., Suh, E. M., & Oishi, S. (2015). Why people are in a generally good mood. Personality and Social Psychology Review, 19(3), 235–256.
Dobson, K. S., & Shaw, B. F. (1987). Specificity and stability of self-referent encoding in clinical depression. Journal of Abnormal Psychology, 96(1), 34.
Elbay, R. Y., Kurtulmuş, A., Arpacıoğlu, S., & Karadere, E. (2020). Depression, anxiety, stress levels of physicians and associated factors in Covid-19 pandemics. Psychiatry Research, 290, 113130.
Engelen, U., De Peuter, S., Victoir, A., Van Diest, I., & Van den Bergh, O. (2006). Verdere validering van de positive and negative affect schedule (PANAS) en vergelijking van twee Nederlandstalige versies. Gedrag en Gezondheid, 34(2), 61–70.
Everaert, J., Koster, E. H., & Derakshan, N. (2012). The combined cognitive bias hypothesis in depression. Clinical Psychology Review, 32(5), 413–424.
Everaert, J., Tierens, M., Uzieblo, K., & Koster, E. H. (2013). The indirect effect of attention bias on memory via interpretation bias: Evidence for the combined cognitive bias hypothesis in subclinical depression. Cognition & Emotion, 27(8), 1450–1459.
Everaert, J., Duyck, W., & Koster, E. H. (2014). Attention, interpretation, and memory biases in subclinical depression: A proof-of-principle test of the combined cognitive biases hypothesis. Emotion, 14(2), 331.
Everaert, J., Grahek, I., Duyck, W., Buelens, J., Van den Bergh, N., & Koster, E. H. (2017). Mapping the interplay among cognitive biases, emotion regulation, and depressive symptoms. Cognition and Emotion, 31(4), 726–735.
Everaert, J., Vrijsen, J. N., Martin-Willett, R., van de Kraats, L., & Joormann, J. (2022). A meta-analytic review of the relationship between explicit memory bias and depression: Depression features an explicit memory bias that persists beyond a depressive episode. Psychological Bulletin, 148(5–6), 435.
Faul, F., Erdfelder, E., Lang, A. G., & Buchner, A. (2007). G* power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods, 39(2), 175–191.
Gotlib, I. H., & Joormann, J. (2010). Cognition and depression: Current status and future directions. Annual Review of Clinical Psychology, 6, 285–312.
Gotlib, I. H., Kasch, K. L., Triall, S., Joormann, J., Arnow, B. A., & Johnson, S. L. (2004). Coherence and specificity of information-processing biases in depression and social phobia. Journal of Abnormal Psychology, 113(3), 386.
Hertel, P. T., & Mathews, A. (2011). Cognitive bias modification: Past perspectives, current findings, and future applications. Perspectives on Psychological Science, 6(6), 521–536.
Hirsch, C. R., Clark, D. M., & Mathews, A. (2006). Imagery and interpretations in social phobia: Support for the combined cognitive biases hypothesis. Behavior Therapy, 37(3), 223–236.
Holland, A. C., & Kensinger, E. A. (2010). Emotion and autobiographical memory. Physics of life Reviews, 7(1), 88–131.
Hyde, T. S., & Jenkins, J. J. (1969). Differential effects of incidental tasks on the organization of recall of a list of highly associated words. Journal of Experimental Psychology, 82(3), 472.
Ingram, R. E. (1984). Toward an information-processing analysis of depression. Cognitive Therapy and Research, 8(5), 443–477.
Joormann, J. (2010). Cognitive inhibition and emotion regulation in depression. Current Directions in Psychological Science, 19(3), 161–166.
Joormann, J., Talbot, L., & Gotlib, I. H. (2007). Biased processing of emotional information in girls at risk for depression. Journal of Abnormal Psychology, 116(1), 135.
Joormann, J., Yoon, K. L., & Zetsche, U. (2007b). Cognitive inhibition in depression. Applied and Preventive Psychology, 12(3), 128–139.
Joormann, J., Waugh, C. E., & Gotlib, I. H. (2015). Cognitive bias modification for interpretation in major depression: Effects on memory and stress reactivity. Clinical Psychological Science, 3(1), 126–139.
LeMoult, J., & Gotlib, I. H. (2019). Depression: A cognitive perspective. Clinical Psychology Review, 69, 51–66.
Marchetti, I., Mor, N., Chiorri, C., & Koster, E. H. (2018). The brief state rumination inventory (BSRI): Validation and psychometric evaluation. Cognitive Therapy and Research, 42(4), 447–460.
Markus, H. (1977). Self-schemata and processing information about the self. Journal of Personality and Social Psychology, 35(2), 63.
Mathews, A., & MacLeod, C. (2005). Cognitive vulnerability to emotional disorders. Annu Rev Clin Psychol, 1, 167–195.
Matt, G. E., Vázquez, C., & Campbell, W. K. (1992). Mood-congruent recall of affectively toned stimuli: A meta-analytic review. Clinical Psychology Review, 12(2), 227–255.
Peckham, A. D., McHugh, R. K., & Otto, M. W. (2010). A meta-analysis of the magnitude of biased attention in depression. Depression and Anxiety, 27(12), 1135–1142.
Reiss, S., Peterson, R. A., Gursky, D. M., & McNally, R. J. (1986). Anxiety sensitivity, anxiety frequency and the prediction of fearfulness. Behaviour Research and Therapy, 24(1), 1–8.
Salari, N., Hosseinian-Far, A., Jalali, R., Vaisi-Raygani, A., Rasoulpoor, S., Mohammadi, M., & Khaledi-Paveh, B. (2020). Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Globalization and Health, 16(1), 1–11.
Salemink, E., Hertel, P., & Mackintosh, B. (2010). Interpretation training influences memory for prior interpretations. Emotion, 10(6), 903.
Sanchez-Lopez, A., De Raedt, R., van Put, J., & Koster, E. H. (2019). A novel process-based approach to improve resilience: Effects of computerized mouse-based (gaze) contingent attention training (MCAT) on reappraisal and rumination. Behaviour Research and Therapy, 118, 110–120.
Storch, E. A., Roberti, J. W., & Roth, D. A. (2004). Factor structure, concurrent validity, and internal consistency of the Beck depression inventory—second edition in a sample of college students. Depression and Anxiety, 19(3), 187–189.
Strube, M. J., Berry, J. M., Lott, C. L., Fogelman, R., Steinhart, G., Moergen, S., & Davison, L. (1986). Self-schematic representation of the type A and B behavior patterns. Journal of Personality and Social Psychology, 51(1), 170.
Sumner, J. A., Griffith, J. W., & Mineka, S. (2010). Overgeneral autobiographical memory as a predictor of the course of depression: A meta-analysis. Behaviour Research and Therapy, 48(7), 614–625.
Tran, T. B., Hertel, P. T., & Joormann, J. (2011). Cognitive bias modification: Induced interpretive biases affect memory. Emotion, 11(1), 145.
van der Does, A. J. W. (2002). BDI-II-NL. Handleiding. De Nederlandse Versie Van De Beck Depression Inventory-2nd edition. Harcourt Test.
Varma, P., Junge, M., Meaklim, H., & Jackson, M. L. (2021). Younger people are more vulnerable to stress, anxiety and depression during COVID-19 pandemic: A global cross-sectional survey. Progress in Neuro-Psychopharmacology and Biological Psychiatry, 109, 11023.
Visser, D. A., Tendolkar, I., Schene, A. H., van de Kraats, L., Ruhe, H. G., & Vrijsen, J. N. (2020). A pilot study of smartphone-based memory bias modification and its effect on memory bias and depressive symptoms in an unselected population. Cognitive Therapy and Research, 44(1), 61–72.
Vrijsen, J. N., Dainer-Best, J., Witcraft, S. M., Papini, S., Hertel, P., Beevers, C. G., & Smits, J. A. (2019). Effect of cognitive bias modification-memory on depressive symptoms and autobiographical memory bias: Two independent studies in high-ruminating and dysphoric samples. Cognition and Emotion, 33(2), 288–304.
Vujanovic, A. A., Arrindell, W. A., Bernstein, A., Norton, P. J., & Zvolensky, M. J. (2007). Sixteen-item anxiety sensitivity index: Confirmatory factor analytic evidence, internal consistency, and construct validity in a young adult sample from the Netherlands. Assessment, 14(2), 129–143.
Watkins, P. C., Mathews, A., Williamson, D. A., & Fuller, R. D. (1992). Mood-congruent memory in depression: Emotional priming or elaboration? Journal of Abnormal Psychology, 101(3), 581.
Watson, D., & Tellegen, A. (1985). Toward a consensual structure of mood. Psychological Bulletin, 98(2), 219.
Watson, D., Clark, L. A., & Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect: The PANAS scales. Journal of Personality and Social Psychology, 54(6), 1063.
Wells, T. T., & Beevers, C. G. (2010). Biased attention and dysphoria: Manipulating selective attention reduces subsequent depressive symptoms. Cognition & Emotion, 24(4), 719–728.
Williams, J. M. G., Watts, F. N., MacLeod, C., & Mathews, A. (1988). Cognitive psychology and emotional disorders. John Willey and Sons Ltd.
Williams, J. M. G., Barnhofer, T., Crane, C., Hermans, D., Raes, F., Watkins, E., et al. (2007). Autobiographical memory specificity and emotional disorder. Psychological Bulletin, 133(1), 122–148.
Wisco, B. E., & Nolen-Hoeksema, S. (2010). Interpretation bias and depressive symptoms: The role of self-relevance. Behaviour Research and Therapy, 48(11), 1113–1122.
Woolridge, S. M., Harrison, G. W., Best, M. W., & Bowie, C. R. (2021). Attention bias modification in depression: A randomized trial using a novel, reward-based, eye-tracking approach. Journal of Behavior Therapy and Experimental Psychiatry, 71, 101621.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic Supplementary Material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zhang, Z., Vrijsen, J., Sanchez-Lopez, A. et al. Attention and Interpretation Bias Modification Transfers to Memory Bias: Testing the Combined Cognitive Bias Hypothesis. Cogn Ther Res (2024). https://doi.org/10.1007/s10608-024-10478-w
Accepted:
Published:
DOI: https://doi.org/10.1007/s10608-024-10478-w