
Abstract
Aim
To identify and map the available evidence regarding the implementation of Making Every Contact Count and/or Healthy Conversation Skills for both staff delivering and service users receiving the brief or very brief intervention/s.
Methods
A scoping review approach was used to rapidly map and provide an overview of the relevant literature, identify gaps in knowledge, and inform further, related research. Articles investigating experiences, perceptions and impact of Making Every Contact Count and/or Healthy Conversation Skills were included. Quantitative, qualitative, and mixed methods studies were eligible for inclusion, as were reviews and reports.
Results
Twenty-two articles were included in total. Healthy Conversation Skills training was found to be acceptable, and had a positive impact on staff confidence and competence in supporting behaviour change, across studies. Some positive effects of intervention exposure on the sedentary behaviour and dietary quality of service users were evidenced. Changes in confidence following Making Every Contact Count training were varied, as was perceived acceptability of the intervention for staff. Two studies highlighted positive impacts of the intervention on service user health; however, statistical significance was not reported. The perceived barriers and facilitators of implementation for both interventions mapped mostly to ‘Environmental Context and Resources’ on the Theoretical Domains Framework.
Conclusion
Healthy Conversation Skills is an acceptable and effective behaviour change intervention that could provide a consistent approach to Making Every Contact Count training and evaluation. Further research is warranted to evaluate this approach for more staff and service user groups.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Making every contact count
‘Making Every Contact Count’ (MECC) is a behaviour change initiative that was introduced to NHS policy across the UK to embed chronic disease prevention into everyday practice and improve public health (Health Education England 2018; NHS 2016). This initiative was developed by NHS Yorkshire and Humber in response to the publication of the National Institute for Health and Clinical Excellence (NICE) public health guidance document (NICE 2007). The guidance highlighted the unique position of frontline staff for promoting lifestyle behaviour change and suggested that such health promotion could reduce the burden of non-communicable diseases (NCDs) in the UK. These NCDs, most commonly including cardiovascular disease, cancer, chronic respiratory diseases, and diabetes, contribute to millions of deaths and billions of pounds spent by the NHS annually (World Health Organisation 2013; Scarborough et al. 2011).
MECC aims to target the four major risk factors associated with these NCDs — smoking, alcohol, physical activity, and diet — which are modifiable and amenable to change (Jepson et al. 2010). Since expert knowledge is not required, MECC can be implemented by staff in all roles and is therefore accessible for millions of service users that might not otherwise engage in health-related interventions. In line with competencies described in the NICE behavior change guidance (NICE 2007), staff trained in level 1 MECC are encouraged to deliver very brief interventions (VBIs), which can be as short as 30 seconds and include raising health-related awareness and appropriate signposting (PHE, NHS England, and HEE 2016). Level 2 trained staff are encouraged to deliver brief interventions (BIs), which last approximately 5 to 15 minutes and include health-related discussion, encouragement, and support, with occasional referral to further intervention (PHE, NHS England, and HEE 2016). There is, however, no universal or consistent approach to MECC, as organisations adopt different strategies to meet NICE guidelines (Wills and Ion 2014; Nelson et al. 2013). Variation between models of MECC is thought, by some, to contribute to the paucity of evidence supporting its effectiveness and discrepancies in implementation success (Chisholm et al. 2020; Chisholm et al. 2019).
Theoretical underpinnings of MECC
MECC commonly draws on the COM-B (‘capability’, ‘opportunity’, ‘motivation’ and ‘behaviour’) model of behaviour change (PHE, NHS England, and HEE 2016), a behaviour science approach developed by Michie et al. (2011). This approach is at the hub of the behaviour change wheel (BCW), a behaviour change framework argued to be one of the most comprehensive and conceptually coherent (Michie et al. 2011). As a dual-process model, the COM-B model seeks to consider all factors that shape behaviour, such as individual lifestyle factors, social and community influences, and wider socio-economic, cultural, and environmental conditions (NICE 2014). Whilst traditional approaches, such as the Health Belief Model (Rosenstock 1974), target the conscious and rational processes driving behaviours, the COM-B model recognises that individual choices can also be affected by unconscious, automatic aspects of decision-making (i.e., habits and impulses). They are additionally shaped by both psychological and physical characteristics, and the physical and social context. Michie et al. (2011) therefore argue that capability, opportunity, and motivation should be considered and addressed when attempting to change behaviour, since the physical and mental ability to do something is insufficient without both the motivation to act (consciously/through habit) and an environment that supports the behaviour in question (Atkins and Michie 2013). This model can be used not only to explore behaviour change in service users receiving interventions but also in individuals training in and delivering them. Researchers and policy makers can therefore understand the enablers and barriers of effective implementation and diagnose why desired behaviours affecting implementation processes and outcomes are not occurring (Handley et al. 2016).
There is research to suggest, for example, that healthcare professionals are not routinely delivering MECC, even when they believe that service users could benefit from behaviour change support (Keyworth et al. 2018). Follow-up research has highlighted several barriers to implementation, such as environmental context, beliefs about capabilities, and social influences (Keyworth et al. 2019). All of these ‘domains’ can be mapped to the COM-B model of behaviour (Cane et al. 2012). Other studies that have evaluated several different models of MECC have found similar barriers (Elwell et al. 2014a, 2014b; Nelson et al. 2013; Tinati et al. 2012; Dewhirst and Speller 2015), suggesting that they should be targeted in order to improve implementation nationally.
Healthy conversation skills
‘Healthy Conversation Skills’ (HCS) is the main training component of the Wessex model of MECC and has demonstrated consistency in approach, effectiveness, and acceptability for both staff delivering and service users receiving the intervention (Lawrence et al. 2016; Lawrence et al. 2020; Jarman et al. 2019; Adam et al. 2020; Black et al. 2014). HCS was developed by a multi-disciplinary team from the Medical Research Council Lifecourse Epidemiology Unit (MRC LEU), University of Southampton, to address barriers among young Southampton mothers in relation to health-related behaviour change (Barker et al. 2008; Lawrence et al. 2009; Lawrence et al. 2011). Drawing from Bandura’s Social Cognitive Theory (1986, 1997), HCS training was designed to equip staff with the skills to have productive, person-centred conversations with service users and empower them to take control of their health behaviours by building self-efficacy and sense of control (Butler et al. 2013). Change happens at both an individual and organisational level, since staff build their own self-efficacy during training in order to change their day-to-day practice, before empowering their clients to change their lifestyle behaviours (Black et al. 2014; Barker et al. 2017). Such change at organisational level is evidenced as a key facilitator for effective health promotion (Sturgiss et al. 2017).
HCS training develops four key competencies: (i) asking open discovery questions (‘how’ and ‘what’ questions), (ii) listening instead of making suggestions or giving advice, (iii) reflecting on practice, and (iv) setting goals using SMARTER (specific, measurable, action-oriented, realistic, timed, evaluated, reviewed) planning (Tinati et al. 2012). Studies have highlighted that those trained in these skills have higher levels of confidence and competence in having person-centred, productive, healthy conversations with service users than those who are not trained (Baird et al. 2014; Jarman et al. 2019). These findings have been demonstrated 1 year after implementation, suggesting that skills can be sustained (Lawrence et al. 2016; Baird et al. 2014).
Similarly, HCS has been evidenced as having a positive impact on service users that are exposed to the intervention. Studies have shown that HCS can have positive effects on sedentary behaviour and dietary quality, compared with controls not receiving the intervention (Adam et al. 2020). Moreover, a protective effect of HCS has been demonstrated on intermediate outcomes, such as sense of control (Baird et al. 2014). Generally, service users have found HCS acceptable and have experienced more benefits from their conversations with staff than those in control groups (Lawrence et al. 2020; Jarman et al. 2019).
Most of these published findings have, however, only been reported for staff working with pregnant service users and females from disadvantaged backgrounds (Lawrence et al. 2016; Lawrence et al. 2020; Jarman et al. 2019). Only one paper to date has evaluated HCS within a region’s MECC framework, for just a handful of staff groups (Dewhirst and Speller 2015). Further research is needed to support the use of HCS within this MECC framework for more staff and service users, particularly within services that behaviour change interventions could benefit most.
Rationale for this scoping review
Similarly, there is a paucity of research supporting MECC nationally for a variety of staff and service users. This is despite the purpose of MECC being its accessibility and implementation by all (Lafreniere and McArthur 2019), with public-facing staff having numerous opportunities per day to deliver it (Keyworth et al. 2018). Previous studies have supported and recommended further MECC research, involving a range of healthcare practitioners, in order to address the challenges faced by specific staff groups in delivering MECC during their routine practice (Elwell et al. 2014a, 2014b; Nelson et al. 2013). Others have highlighted the importance of evaluating MECC for more patient groups, in order to assess its true impact on public health (Baird et al. 2014; Dewhirst and Speller 2015; Jarman et al. 2019; Keyworth et al. 2018; Wills and Ion 2014).
Research objective
The purpose of this scoping review is to identify and synthesise MECC evidence in order to establish how this behaviour change intervention is perceived and the impact it is having on a national scale for both staff in public-facing roles and individuals accessing health-related services. A specific focus is the Wessex MECC/HCS approach. This is essential for informing future research and optimizing MECC implementation as it is rolled out further, in line with the UK’s public health policy.
Review questions
-
1.
What are the experiences and perceptions of staff trained in MECC and/or HCS in relation to acceptability, feasibility, facilitators, and barriers to its implementation and delivery?
-
2.
How does MECC and/or HCS training impact staff confidence and/or competence in having ‘healthy’ conversations and delivering MECC and/or HCS?
-
3.
How acceptable is MECC and/or HCS to service users and what impact does the intervention have on self-efficacy, health knowledge, and/or behaviours?
Methods
Scoping reviews employ exploratory review methodologies to rapidly map the main sources and types of evidence available on a well-defined topic, identify gaps within the literature, and inform further investigation (Arksey and O'Malley 2005). In contrast to systematic reviews, which most often aim to answer a focused research question in a systematic manner, scoping reviews allow for the broader mapping of varying evidentiary levels of research to present an overview of a topic (Pham et al. 2014). The purpose of a scoping review is to chart the evidence, mainly according to level of evidence, e.g., RCTs, cohorts, case controls, etc. Scoping reviews can be helpful precursors to a systematic review and can help confirm the relevance of inclusion criteria and identify potential questions, rather than answer a specific question where data are combined in a meta-analysis, as found in a systematic review (Munn et al. 2018). A scoping review was chosen in order to assess all available research for two brief interventions with limited empirical evidence, identify and analyse knowledge gaps, and inform future, related reviews and research. As MECC and HCS are relatively new interventions, it was anticipated that a scoping review could summarise the current evidence base and determine the value of undertaking a full systematic review in the future. The review questions were broad and inclusive, encompassing all models and interpretations of MECC, and a diverse range of individuals delivering, commissioning, training in, and receiving the intervention/s. A protocol was developed and made publicly available on Open Science Framework, prior to the commencement of this review.
The methodological framework for this scoping review was developed based upon that of Arksey and O'Malley (2005), who recommended that methods should be rigorous and transparent at all stages of the scoping review process, an expectation upheld by proponents of systematic reviews. The Joanna Briggs Manual for Evidence Synthesis (Peters et al. 2020) notes that many of the defining characteristics of methodological approach for systematic reviews and scoping reviews are the same; however, critical appraisal (risk of bias assessment) is not usually conducted in the latter. Enhancements proposed by the Joanna Briggs Institute refined scoping review methodological framework (Peters et al. 2020) were employed in the methods of the current review. These consisted of:
-
1.
Defining and aligning the objective/s and question/s
-
2.
Developing and aligning the inclusion criteria with the objective/s and question/s
-
3.
Describing the planned approach to evidence searching, selection, data extraction, and presentation of the evidence
-
4.
Searching for the evidence
-
5.
Selecting the evidence
-
6.
Extracting the evidence
-
7.
Analysis of the evidence
-
8.
Presentation of the results
-
9.
Summarizing the evidence in relation to the purpose of the review, making conclusions and noting any implications of the findings
Inclusion criteria
Inclusion criteria were defined in terms of sample, phenomenon of interest, design and research type, and setting.
-
(i)
Sample
Evidence for this review included participants involved in the delivery, commissioning, or training of MECC and/or HCS, and individuals that received the intervention in accessed services. Many of the staff participating in studies in this review were in public-facing roles. These included any occupation that involves working directly with service users across NHS trusts, local authorities, and other health, social care, and voluntary services. Service users included in this study had received a MECC and/or HCS behaviour change intervention in these settings.
-
(ii)
Phenomenon of interest
This review included any studies that investigated experiences, perceptions, and impact on individuals delivering or receiving a MECC and/or HCS behaviour change intervention. All MECC frameworks were included. Studies focusing on HCS alone were also eligible if they related to the training programme developed by the MRC LEU, University of Southampton.
-
(iii)
Design and research type
This review included qualitative, quantitative and mixed methods studies, incorporating a range of widely recognised methods of data collection and analysis. These included data collection methods such as interviews, surveys, and randomised control trials (RCTs), and data analysis and statistical methods including thematic analysis, content analysis, chi-squared tests, and t-tests. Reviews, reports, and grey literature were included in this review if relevant data could be identified and assessed in order to answer the research questions.
-
(iv)
Setting
Studies were included regardless of the country in which they were conducted or the setting in which data were collected.
Exclusion criteria
Articles containing only description or commentary on MECC and/or HCS were excluded from the review. Articles that were not written in English language were also excluded due to resource constraints.
Search strategy
The following databases were searched from their inception for relevant articles on 21st May 2020:
-
1.
MEDLINE (via Ovid)
-
2.
Embase (via Ovid)
-
3.
AMED (via Ovid)
-
4.
CINAHL
-
5.
Web of Science
-
6.
Cochrane Library
-
7.
SportDiscus
-
8.
OpenGrey
An example of the search strategy used in MEDLINE is shown in the appendix (Appendix Table 3). The search strategy was modified to account for specificities of the other electronic databases.
Reference lists of all included articles were additionally hand-searched, and the first ten pages of Google Scholar, sorted by ‘relevance’, were scanned to identify any material that may have been missed in previous searches. Finally, key authors in the research field were consulted to identify remaining relevant, eligible articles.
Results from the database searches were collated and imported into an Endnote library. All duplicates were removed during the first stage of the data screening process.
Selection of studies
Titles and abstracts of remaining articles were screened individually by one reviewer and five assistants (VH, LRR, BH, NW, LR). The reviewer and assistants piloted the screening using ten articles prior to this. Any discrepancies were discussed and resolved with an external reviewer, if required. Potentially eligible articles were retrieved in full and assessed in detail. Data extraction was undertaken for those that met the full inclusion criteria.
Data extraction and analysis
A data spreadsheet was developed and used to extract relevant data from the included studies. This was initially piloted on several articles by a reviewer to ensure appropriate data were extracted. Extracted data comprised:
-
a)
Publication Information: Paper title, author/s, year of publication, journal
-
b)
Sample: Sample size, participant characteristics
-
c)
Phenomenon of interest: Aims, intervention (MECC/HCS), key findings, recommendations
-
d)
Study design: Design, research type
-
e)
Study setting: Setting type (i.e., NHS, local authority), location
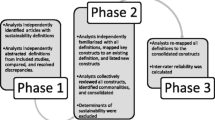
One reviewer employed inductive, thematic analysis (Braun and Clarke 2006) to analyse qualitative data in order to identify common themes regarding the acceptability, feasibility, barriers, and facilitators of intervention implementation. Consistent with the six-stage process of thematic analysis (Braun and Clarke 2006; Braun and Clarke 2019), the first stage of the analytic process involved the reviewer familiarising herself with the data. Next, the entire data set was coded and data within each code were collated. Thirdly, initial themes were generated using these codes, reviewed and refined. Themes were defined and given clear names and, finally, write-up began.
Inductive codes relating to barriers and facilitators of MECC and/or HCS implementation were mapped to the Theoretical Domains Framework (TDF). The TDF links to the larger, meta-framework known as the BCW (mentioned earlier), which also incorporates the COM-B model (Michie et al. 2011). The fourteen-domain TDF (Appendix Table 5) was deemed to be the most suitable analytical framework, as it prompts an analysis of environmental (e.g., resources), social (e.g., interpersonal influences), cognitive (e.g., decision processes), and affective (e.g., optimism) influences on healthcare professional practice (Cane et al. 2012). Hence, it can be used to identify retrospectively factors contributing to the successes and/or challenges of intervention implementation (Nilsen 2015) and, by doing so, theoretically inform future research.
Data presentation
A narrative summary describing how the results relate to the review objectives and questions is given in the following section. Characteristics of the included studies (supplementary resource 1) are presented in tabular form, in a manner that aligns with scoping review guidelines as per the Joanna Briggs Institute (Peters et al. 2020). Quantitative results, including p-values, were included in this table in order to display statistically significant findings.
Results
Study selection
The initial review searches yielded a total of 617 articles from a range of electronic databases and grey literature. One hundred and thirty-nine duplicates were removed, and a further 445 ineligible articles were excluded by the reviewers during abstract screening. Thirty-three full texts of potentially relevant articles were retrieved for detailed eligibility assessment. Of these, 12 were excluded due to the inclusion criteria not being met and one was excluded due to the reviewers being unable to gain access to the article. A further six articles were excluded as they were duplicates of others that met full inclusion criteria. Reasons for exclusion are specified in the appendix (Appendix Table 4). A review of full-text reference lists retrieved six articles, and an additional two articles were retrieved following consultation with experts in the research field, bringing the total count of eligible articles included in this scoping review to 22 (see Fig. 1).

Search results, study selection and inclusion process. Adapted from Moher et al. (2009)
Study characteristics
Of those included, seven articles were quantitative, seven were qualitative, and eight were mixed-methods studies. The most common research design employed was the qualitative interview, accounting for 27% of the total included articles (n = 6). This was followed by the before and after evaluation design (18% of total, n = 4), pilot/randomised controlled trial (14% of total, n = 3), non-randomised controlled trial (9% of total, n = 2), prospective survey (9% of total, n = 2), feasibility evaluation (9% of total, n = 2), retrospective survey (5% of total, n = 1), service evaluation (5% of total, n = 1) and content analysis study (5% of total, n = 1). Most articles focused on general MECC (64% of total, n = 14) and the remaining articles focused on HCS (36% of total, n = 8). Of the latter articles, the vast majority of staff participants were health and social care practitioners. All service users were mothers or pregnant women. General MECC articles involved a range of staff participants, including nurses, midwives, public health practitioners, physiotherapists, general practitioners, specialist doctors, and MECC/strategic leads. Service user participants were attending either a gastroenterology service or an MSK physiotherapy service. Some studies did not specify the number of participants involved (Moss and Bancroft 2019) or their type (Lafreniere and McArthur 2019). All articles were published from 2012 onwards.
Healthy Conversation Skills
Staff
Seven studies in total evaluated the HCS intervention for staff. The majority of these studies recruited participants from Sure Start Children’s Centres (SSCCs) in Southampton, Gosport, and Havant (Baird et al. 2014; Black et al. 2014; Lawrence et al. 2016; Tinati et al. 2012). Participants were in a variety of health and social care roles, and worked to support women from disadvantaged backgrounds. Other studies recruited research nurses, midwives (Lawrence et al. 2020), and registered dieticians (Adam et al. 2020; Jarman et al. 2019) who delivered HCS to pregnant women. The final study involved eight distinct teams from two NHS Trusts and a local council in the South of England (Dewhirst and Speller 2015). These teams included therapy services, diabetes services, occupational health services, a minor injuries unit, heart failure and respiratory unit, and a local area housing office. Three of seven studies incorporated quantitative research methods to describe the implementation of HCS (Lawrence et al. 2016) and assess changes in confidence and competence in having ‘healthy conversations’ (Baird et al. 2014; Black et al. 2014; Lawrence et al. 2016). The designs of these studies included two non-randomised controlled studies (Baird et al. 2014; Lawrence et al. 2016) and a before and after study (Black et al. 2014). The remaining four studies used mixed methods to evaluate the acceptability of HCS (Jarman et al. 2019; Lawrence et al. 2020), feasibility of its implementation (Dewhirst and Speller 2015; Lawrence et al. 2020) and associated barriers and facilitators (Tinati et al. 2012; Dewhirst and Speller 2015). These studies were described as a pilot RCT (Jarman et al. 2019), RCT (Lawrence et al. 2020), feasibility evaluation (Dewhirst and Speller 2015), and content analysis study (TInati et al. 2012).
Acceptability
HCS was considered largely acceptable to staff. In one study, there were significant increases in perceived usefulness of HCS in supporting change (Dewhirst and Speller 2015), suggesting that learned skills were bringing additional perceived value to conversations. The same study also highlighted a significant increase in perceived importance of participants’ roles in supporting behaviour change following HCS training. Studies reported trainees rating the value of HCS training highly, at 8/10 (Lawrence et al. 2016) and 9/10 (Dewhirst and Speller 2015).
Three studies presented qualitative data relating to perceived acceptability of the HCS intervention (Dewhirst and Speller 2015; Lawrence et al. 2016; Lawrence et al. 2020). Thematic analysis identified four themes, including (i) benefits of HCS training, (ii) benefits to the organisation, (iii) benefits to staff, and (iv) benefits to the service user.
-
(i)
Benefits of HCS training
HCS training was considered acceptable to participants. Training content was reviewed positively by participants across studies (Dewhirst and Speller 2015; Lawrence et al. 2020; Lawrence et al. 2016). They referred to useful examples and tips given in training, sessions being interactive and non-didactic, and the programme following a structured and empowering framework.
Participants also valued being able to practise and enhance their skills during training, which included observing others and evaluating their own techniques in order to improve (Dewhirst and Speller 2015).
-
(ii)
Benefits to the organisation
The HCS intervention was also considered acceptable for the organisations in which participants worked (Dewhirst and Speller 2015). Participants viewed HCS as positively contributing to changing cultures, impacting both service and organisational changes.
Some valued HCS in fitting with current service provision, complementing government policy and the idea that prevention is part of the healthcare professional role.
Finally, participants felt that HCS could contribute to improvements in cost savings and workforce health, which they believed could lead to substantial organisational benefits.
-
(iii)
Benefits to staff
Participants across studies identified many benefits of HCS for both themselves and within their departments. These included benefits in their own communications with clients, involving more productive conversations (Dewhirst and Speller 2015; Lawrence et al. 2020), improvements in professional roles and connections with other services (Dewhirst and Speller 2015; Lawrence et al. 2016), improved relationships within teams, including learning from others (Lawrence et al. 2020; Dewhirst and Speller 2015), and benefits to participants’ and their families’ lifestyles (Dewhirst and Speller 2015).
-
(iv)
Benefits to the service user
The HCS intervention was also considered acceptable to deliver to patients and service users. Participants valued that the intervention is person-centred and is therefore guided by the service user, allowing them to explore their own health behaviours (Dewhirst and Speller 2015). They felt the patient experience was improved by the intervention, particularly for service users who had repeat appointments (Dewhirst and Speller 2015). In addition to this, participants felt that HCS contributed to positive changes in relationships between themselves and their service users, having the potential to transform the way they provide health-related support (Dewhirst and Speller 2015; Lawrence et al. 2020). Finally, the intervention was felt to have multiple positive impacts on the service user, including improved health, debt management, and increased access to support (Dewhirst and Speller 2015).
Barriers and facilitators to implementation
Three main themes were identified during thematic analysis in relation to perceived barriers and facilitators to implementing HCS, including (i) practical context, (ii) attitudes towards implementation, and (iii) relevance and use of skills. Barriers and facilitators were mapped to seven TDF domains. The most prominent domains were ‘Environmental Context and Resources’ and ‘Social/ Professional Role and Identity’ (Table 1).
-
(i)
Practical context
Time was considered a barrier by many participants, as they felt this was limited and found it difficult to fit healthy conversations into their usual schedules (Dewhirst and Speller 2015; Lawrence et al. 2020; Tinati et al. 2012). In contrast, finding opportunities to have these healthy conversations and fitting them into natural conversation flow were considered facilitators of implementing the intervention (Dewhirst and Speller 2015; Tinati et al. 2012).
Resource limitations were also identified as a practical barrier to HCS implementation (Dewhirst and Speller 2015). These included inadequate referrals and recording systems in order to signpost service users to relevant services and to evaluate the impact of healthy conversations. Having follow-up appointments with service users to enable the continuation of healthy conversations and check progress, access to signposting and information resources, and recording conversations were identified as key facilitators (Dewhirst and Speller 2015; Jarman et al. 2019).
-
(ii)
Attitudes towards implementation
Staff lacking the confidence to initiate healthy conversations and/or use skills learnt during training was identified as a key barrier to implementation, as was the perception of the intervention being extra work and lack of support from management (Dewhirst and Speller 2015; Tinati et al. 2012). Receptiveness of service users was an additional barrier, including them not wanting to make a change or engage with healthy conversations (Dewhirst and Speller 2015; Tinati et al. 2012; Jarman et al. 2019).
In contrast, staff feeling confident in having healthy conversations (i.e., by practising skills, particularly SMARTER planning), having a good relationship with service users to initiate these conversations, and feeling supported and motivated by senior staff to implement HCS were all key facilitators (Jarman et al. 2019; Dewhirst and Speller 2015; TInati et al. 2012).
-
(iii)
Relevance and use of skills
Difficulty in not reverting back to the ‘norm’ within roles was identified as a barrier in relation to the use of HCS skills (Jarman et al. 2019). This included avoiding simply giving advice, which was perceived as meeting the usual expectations of the service users. Facilitators included use of the skills for exploring individual contexts (Jarman et al. 2019), skill relevance and ease of use, and seeing the benefits of using the skills (Tinati et al. 2012).
HCS training had a positive impact on the confidence and competence of staff in having health-related conversations. High competence was observed in studies assessing the short-term, medium-term, and long-term impacts of training, suggesting that skills developed during training were sustained.
Short-term impacts of HCS training were assessed in most studies using pre-post training evaluation forms that were distributed to trainees before and directly after the programme (Dewhirst and Speller 2015; Black et al. 2014; Lawrence et al. 2016). In all studies, there were significant increases in the number of open discovery questions used to respond to health-related statements, and significant decreases in giving information or making suggestions from pre- to post-training. This shift reflects an increase in ability to have an empowering, person-centred conversation. Two studies reported that participant confidence levels for supporting behaviour change increased significantly from pre- to post-training (Dewhirst and Speller 2015; Black et al. 2014). A significant positive relationship between levels of competence and overall confidence was also observed (Black et al. 2014), suggesting that those scoring highest on competence in using open discovery questions felt more confident in having conversations about health behaviours.
Studies that assessed medium-term impacts of HCS demonstrated that participants maintained at least some competence several weeks after training. The majority of participants had moderate to high competency in finding opportunities to have healthy conversations (Lawrence et al. 2016) and asking open discovery questions (Black et al. 2014; Lawrence et al. 2016) from 4 to 12 weeks post-training. One study found that, after training, the competence of a registered dietician increased throughout visits with service users (Jarman et al. 2019). As the study progressed, the dietician asked more open discovery questions and listened more, therefore their service users spent more time speaking. Despite this, some studies highlighted that there was limited evidence to suggest that these open discovery questions were used to support SMARTER goal setting (Lawrence et al. 2016; Jarman et al. 2019; Dewhirst and Speller 2015), indicating use of and competence in this particular skill was minimal. In contrast, a later study evidenced the high competence levels of its participants in HCS, 26 weeks into the intervention, including SMARTER goal setting (Lawrence et al. 2020). The authors reported that participants supported their service users to set more goals in the later stages of the study.
The long-term impacts of HCS training were assessed in two studies which compared intervention and control groups (Lawrence et al. 2016; Baird et al. 2014). In both studies, staff in the intervention groups used skills to support behaviour change in service users significantly more than those in control groups. This finding was observed 1 year post training. One study (Lawrence et al. 2016) reported a significant difference between groups in use of skills 1 (creating opportunities for healthy conversations), 2 (use of open discovery questions), and 4 (listening instead of making suggestions/giving information), but not skill 5 (SMARTER planning).
Service users
Four studies in total incorporated service users to evaluate HCS. All participants were either pregnant mothers or parents accessing Sure Children’s Centres in the Wessex region, England (Baird et al. 2014; Lawrence et al. 2020) or Alberta, Canada (Adam et al. 2020; Jarman et al. 2019). Two of four studies used quantitative research methods to assess changes in measures such as gestational weight gain (Adam et al. 2020), dietary quality (Adam et al. 2020; Baird et al. 2014), physical activity (Adam et al. 2020), level of self-esteem (Baird et al. 2014), and sense of control (Baird et al. 2014). The design of these studies included a pilot RCT (Adam et al. 2020) and non-randomised controlled study (Baird et al. 2014). The remaining two studies were described as a pilot RCT (Jarman et al. 2019) and an RCT (Lawrence et al. 2020). They incorporated mixed methods to assess perceived acceptability of the HCS intervention (Jarman et al. 2019; Lawrence et al. 2020), the use of HCS to aid behaviour change goals, and perceived feasibility of using HCS during routine maternity care (Lawrence et al. 2020).
There were no statistical differences between gestational weight gain or concordance with gestational weight gain guidelines of pregnant women receiving the HCS intervention and those in an active or passive control group, who did not receive HCS (Adam et al. 2020). These results were reported by the authors as reflecting the challenges of maintaining weight gain within the Institute of Medicine (IOM) guidelines and improving weight outcomes during pregnancy, particularly for those who are overweight or obese at conception (Jarman et al. 2016). Similarly, no statistical differences were found in any studies between the self-reported physical activity of the HCS intervention groups and active control groups at any time-point (Adam et al. 2020; Baird et al. 2014). One study did report a statistically significant improvement in the activity levels of the intervention group between baseline and follow-up; however, this was not predicted by self-efficacy or sense of control (Baird et al. 2014). Instead, changes in physical activity were predicted by the women being employed at follow-up. The authors thus concluded that these improvements were not associated with intervention exposure. A statistical difference between intervention and control groups was, however, reported in mean time spent being sedentary at 34 weeks’ gestation (Adam et al. 2020). Women receiving HCS in the intervention group reported being sedentary for a mean of 3 metabolic equivalent (MET) hours per week less than those in the active control group, suggesting that HCS had some positive effect on pregnant women’s activity.
Changes in dietary quality varied between studies. Pregnant women who interacted with a HCS-trained research dietitian significantly improved their dietary quality score between baseline and 34 weeks gestation (Adam et al. 2020). In the same study, the scores of those not receiving HCS did not significantly change between study visits. In contrast, disadvantaged women accessing Sure Children’s Centres had statistically significant declines in dietary quality between baseline and 18-month follow-up (Baird et al. 2014); a finding that was significantly predicted by educational attainment. These results were similar to those reflected in the control group, who had not received the HCS intervention. The self-efficacy and sense of control of these participants also significantly declined, but this decline was significantly smaller in the intervention group than the control group. Moreover, a significant association between increased exposure to HCS and a smaller decline in sense of control was reported. This suggested some protective effect of HCS on these intermediate outcomes.
Findings from studies assessing the acceptability of HCS showed that pregnant women were generally in favour of the intervention (Lawrence et al. 2020; Jarman et al. 2019) and felt it should be included within routine care (Lawrence et al. 2020). Women receiving HCS found the intervention acceptable, and experienced more benefits from their conversations with healthcare professionals than those in control groups. These benefits included feeling empowered and encouraged to think about improving health behaviours (Lawrence et al. 2020) and feeling as though the healthcare professional was interested in them and their pregnancy (Lawrence et al. 2020; Jarman et al. 2019). Those receiving HCS recalled discussing plans for change and strategies for overcoming barriers to change (Lawrence et al. 2020), and felt that being involved in the study had helped to change at least one lifestyle habit (Jarman et al. 2019). In comparison, individuals in control groups did not report having made any plans for behaviour change as a result of talking to the healthcare professionals.
MECC
Staff
Thirteen studies in total evaluated MECC for staff. Participants were recruited from a variety of locations within the UK, including Birmingham (Elwell et al. 2014a, 2014b), Salford (Lafreniere and McArthur 2019), Greater Manchester (Moss and Bancroft 2019), Yorkshire and Humber (Nelson et al. 2013), Gloucestershire (Tucker 2019), Wales (Webster 2018) and Ireland (Mulroe et al. 2017). Other studies recruited participants from multiple areas (Chisholm et al. 2019; Chisholm et al. 2020; Keyworth et al. 2019; Wills and Ion 2014) or did not specify (Wills and Kelly 2017). Most participants were in a variety of roles and working with different types of service user. Others were stakeholders involved in the design, commissioning, training, or evaluation of MECC (Wills and Ion 2014; Nelson et al. 2013; Chisholm et al. 2019). Several studies did not detail participant roles (Moss and Bancroft 2019; Lafreniere and McArthur 2019; Tucker 2019). Seven studies used qualitative methods (Chisholm et al. 2019; Elwell et al. 2014a, 2014b; Keyworth et al. 2019; Mulroe et al. 2017; Nelson et al. 2013; Wills and Ion 2014), two used quantitative methods (Wills and Kelly 2017; Webster 2018), and three used mixed methods (Lafreniere and McArthur 2019; Chisholm et al. 2020; Tucker 2019) to evaluate perceived acceptability, barriers, and facilitators of implementing/ delivering MECC. Six studies additionally explored the impact of MECC on staff competence (Tucker 2019) and confidence (Chisholm et al. 2020; Lafreniere and McArthur 2019; Wills and Kelly 2017; Webster 2018; Moss and Bancroft 2019). There were six interview designs (Wills and Ion 2014; Nelson et al. 2013; Keyworth et al. 2019; Elwell et al. 2014a, 2014b; Chisholm et al. 2019), three before and after studies (Moss and Bancroft 2019; Webster 2018; Wills and Kelly 2017), one prospective survey (Chisholm et al. 2020), one retrospective survey (Lafreniere and McArthur 2019), one feasibility study (Mulroe et al. 2017), and one service evaluation (Tucker 2019).
Acceptability
MECC was mostly acceptable to staff. One study reported MECC as being most valued by participants, compared to two other interventions that also aimed to improve health and wellbeing (Wills and Kelly 2017). These interventions included a step-recording accelerometer and an online personal wellness tool. Another study found an increase of 17% from pre to post training in participants strongly agreeing the importance of MECC (Webster 2018).
Thematic analysis of qualitative data relating to perceived acceptability of MECC identified three themes: (i) training value, (ii) engagement levels, and (iii) changing culture.
-
(i)
Training value
There were mixed results with regard to the acceptability of training to participants.
Training was considered relevant by participants in one study (Tucker 2019), who felt that it was applicable to practice. These individuals received MECC ‘plus’ training, which was adapted for Integrated Community Teams. In contrast, some participants (mostly nurses and midwives) who engaged in an online behaviour change skills module felt that this MECC training was not relevant or relatable to day-to-day practice (Chisholm et al. 2020).
Despite bringing new knowledge whilst reconsolidating that learnt previously for some, others felt that the online training content was confusing and complex (Chisholm et al. 2020). Stakeholders involved in the training, delivery, or commissioning of MECC, however, felt that training content was flexible and pitched at the right level (Nelson et al. 2013).
In one study, it was agreed by public health practitioners that at least some standardisation of MECC training, based on evidenced efficacy, would enhance programmes and reduce ambiguity over training objectives (Chisholm et al. 2019).
The ‘Train the Trainer’ programme was considered valuable and a way of providing organisations with capacity to deliver MECC (Nelson et al. 2013).
-
(ii)
Engagement levels
Staff across studies felt that staff were supportive of MECC (Chisholm et al. 2019; Lafreniere and McArthur 2019). In one study, it was noted that frontline staff were more willing to take part and were more optimistic about MECC’s sustainability compared to managers (Lafreniere and McArthur 2019).
Many staff also acknowledged the idea that MECC should involve everybody. Participants viewed MECC as being the role of everyone (Wills and Ion 2014; Elwell et al. 2014a), engaging many in order to have a greater impact (Nelson et al. 2013), and including non-professional staff (Nelson et al. 2013).
-
(iii)
Changing culture
Staff valued MECC as supporting a cultural change within organisations (Wills and Ion 2014). This included contributing to whole system change and reorienting services to prevention.
Barriers and facilitators to implementation
Four main themes were identified during thematic analysis in relation to perceived barriers and facilitators to implementing MECC; (i) evaluating MECC, (ii) system-level influencers, (iii) staff capacity and (iv) attitudes towards MECC. Barriers and facilitators were mapped to six TDF domains. The most prominent domain for both barriers and facilitators was ‘Environmental Context and Resources’ (Table 2).
-
(i)
Evaluating MECC
Difficulty in evaluating MECC for service users was reported as a barrier to staff adopting and implementing MECC (Chisholm et al. 2019), as was the lack of evidence of impact in general (Wills and Ion 2014; Elwell et al. 2014b). In contrast, a facilitator to implementation was being able to refer patients to specialist services (Chisholm et al. 2019). This was considered a feasible and meaningful way to evaluate MECC success. Similarly, staff having ongoing follow-ups with service users was considered a facilitator to MECC implementation (Nelson et al. 2013).
-
(ii)
System level influencers on MECC implementation
A lack of resources was identified as a system-level barrier to MECC implementation (Chisholm et al. 2019; Wills and Ion 2014), including money and resource for training and education. Organisational culture was another reported barrier (Nelson et al. 2013; Chisholm et al. 2019; Keyworth et al. 2019), including lack of endorsement from senior managers.
Facilitators included (1) advocates and champions for MECC (Chisholm et al. 2019; Wills and Ion 2014), (2) supporting infrastructure for staff (Chisholm et al. 2019), (3) resources, such as a sum of money to assist with effective implementation (Wills and Ion 2014; Keyworth et al. 2019; Elwell et al. 2014b), and (4) having an implementation plan in place (Wills and Ion 2014). Another facilitator was perceived benefits to the organisation, such as saving money and reducing hospital admissions (Elwell et al. 2014b).
-
(iii)
Staff capacity
Lack of time was identified as a barrier to MECC implementation by many participants (Elwell et al. 2014b; Keyworth et al. 2019; Mulroe et al. 2017), as was workload pressure (Mulroe et al. 2017; Keyworth et al. 2019).
-
(iv)
Attitudes towards MECC
Staff lacking confidence in delivering MECC was identified as a key barrier (Elwell et al. 2014a; Keyworth et al. 2019), as was the perception that MECC is extra work and not part of the role (Nelson et al. 2013; Keyworth et al. 2019). Other barriers included the perception that MECC might offend service users (Nelson et al. 2013; Elwell et al. 2014a) and service users not being receptive or ready to change (Mulroe et al. 2017; Keyworth et al. 2019; Elwell et al. 2014a).
Facilitators included (1) high staff engagement (Chisholm et al. 2019; Wills and Ion 2014), (2) the perception that staff are advocates for healthy lifestyles and initiating discussions (Keyworth et al. 2019), (3) the professional–patient relationship to facilitate health-related discussions (Keyworth et al. 2019;Wills and Ion 2014), and (4) incentives to create staff buy-in (Nelson et al. 2013).
MECC training had a mostly positive impact on staff across studies. Findings in relation to confidence were relatively consistent, despite participants being trained using different MECC frameworks. Only one study attempted to evaluate levels of competence in MECC skills or MECC-style conversations (Tucker 2019). It highlighted that 83% of staff who initially felt they lacked knowledge in healthy lifestyles had successfully altered their practice 2 months following MECC training.
Two studies reported an increase in participants’ self-efficacy/confidence in having health-related conversations following online MECC training (Chisholm et al. 2020; Moss and Bancroft 2019). Another reported an increase in confidence in having MECC-style conversations across staff groups; however, those trained at level 1 (VBI) felt more confident than those at level 2 (BI), and were more likely to incorporate MECC into day-to-day work (Lafreniere and McArthur 2019).
Two studies reported mixed results in relation to participant confidence following training. One reported that some participants had no confidence at all in discussing alcohol, smoking, and weight (Wills and Kelly 2017). In contrast, high confidence was reported in discussing exercise and diet. The other study reported confidence with MECC skills decreasing from pre-training to post-training (Webster 2018). In contrast, confidence in their healthy lifestyle knowledge base, approach to health conversations, and responding to disengagement from service users increased.
Service users
Only two studies in total incorporated service users to evaluate the national MECC initiative. Participants were recruited from two different locations in the UK; Worcestershire and Bury, Greater Manchester. They were attending an outpatient gastroenterology clinic (Davies et al. 2014) and musculoskeletal (MSK) physiotherapy service (Moss and Bancroft 2019) respectively. One study was defined as a prospective study, incorporating mixed methods (Davies et al. 2014), and the second study was a quality improvement study, using quantitative methods (Moss and Bancroft 2019). Both assessed the impact of implementing a MECC-style intervention on service user health. No studies assessed the acceptability of MECC to service users.
Both studies (Moss and Bancroft 2019; Davies et al. 2014) reported the impact of MECC on service users’ health; however, findings were not reported as statistically significant. One study reported that 75% of service users that received MECC scored highly in confidence and readiness to change following the intervention (Davies et al. 2014). These individuals had previously scored positive on the Alcohol Use Disorders Identification Test (AUDIT-C). Those receiving the extended intervention demonstrated a decrease in AUDIT-C scores and reduced alcohol unit consumption. The second study reported an increase in referrals to a local exercise scheme of 70% in the year following MECC implementation (Moss and Bancroft 2019). A total of 73% of MSK service users that were referred were still physically active 12 months later.
Discussion
Main findings
The purpose of this review was to identify and map all available evidence relating to the implementation of MECC and HCS for both staff delivering and service users receiving the intervention. Findings aimed to inform future research and optimise further implementation, since MECC remains a prominent strategy to meet NICE behaviour change guidance (NICE 2007; Nelson et al. 2013).
HCS training had a positive impact on both staff competence and confidence in supporting behaviour change with service users. Competence was demonstrated in the short, medium, and long term, particularly in using open discovery questions, which is indicative of a productive, person-centred healthy conversation (Black et al. 2014). Significant differences in the use of skills to support behaviour change were highlighted between staff who had received HCS training and those who had not, 1 year after implementation. SMARTER goal setting was, however, implemented less often across studies both in the medium and long term: a finding that could be due to a need for ongoing support for trainees to acquire and practise the skill (Lawrence et al. 2016). These findings highlighted that skills developed during HCS training can be successfully sustained and changes in practice can persist (Lawrence et al. 2016), however, further follow-up and support for staff is needed to build confidence and competence in using SMARTER goal setting.
The HCS programme was considered acceptable to staff. Quantitative results demonstrated high ratings of perceived HCS value and a significant increase in perceived usefulness of behaviour change conversations from pre- to post-training. This suggests that skills developed during training were bringing additional value to conversations. Qualitative results showed that participants felt HCS training was useful, interactive, and empowering, and they valued being able to evaluate their own use of skills and learn from observing others. Benefits were observed for the organisation, including HCS contributing to a changing culture, which fits with the NHS Five Year Forward view (NHS England 2014). Staff felt that HCS training also contributed many benefits to their communications with service users and within their professional roles and personal lives, such as their own and their families’ lifestyles. This suggests that HCS could have a positive impact beyond the workplace and might contribute to health and wellbeing on a larger scale. Finally, staff perceived HCS as being acceptable and highly beneficial for the service users they support, having multiple potential impacts, including improved health and access to support. Some felt that delivering HCS could improve the patient experience, particularly for those who have repeat appointments with staff. Individuals accessing services regularly may therefore benefit most from HCS, potentially due to the consistent exposure to healthy conversations and extended support in lifestyle behaviour change. This has been supported by a study that demonstrated the protective effect that increased exposure to HCS has on sense of control, as discussed later (Baird et al. 2014).
Three themes were identified in relation to the barriers and facilitators of HCS implementation, including practical context, attitudes towards implementation, and relevance and use of skills. Inductive codes were mapped to seven TDF domains in total but ‘Social/Professional Role and Identity’ and ‘Environmental Context and Resources’ were the most prominent, suggesting that these domains should be targeted for enhanced future implementation of HCS. Time and resource constraints were key barriers to implementing HCS in relation to the environmental context, whereas having access to resources and finding opportunities to have healthy conversations were facilitators. This is consistent with evidence in the MECC literature and beyond, which suggests that the work environment, time, and resource limitations can hinder the delivery of a range of behaviour change interventions (Um et al. 2013; Glowacki et al. 2019). behaviour change techniques (BCTs) may be useful in addressing barriers associated with the Environmental Context and Resources domain (Michie et al. 2014; Cane et al. 2015). For example, restructuring the physical or social environment to include signposting resources, and providing prompts and cues to remind staff to schedule healthy conversations into appointments (Keyworth et al. 2019; Cane et al. 2015). Participants additionally felt that it was difficult not reverting back to the ‘norm’ in their traditionally advice-giving role, and some felt that HCS was perceived as being extra work. These were barriers associated with Social/ Professional Role and Identity on the TDF. Cane et al. (2015) found that no BCTs were significantly assigned to this domain by 18 behaviour change experts. The COM-B model can, however, be applied here to identify relevant BCTs. ‘Social/Professional Role and Identity’, for example, was mapped onto both the automatic and reflective motivation components of the COM-B model by behaviour change experts (Cane et al. 2012). These components have been linked with various intervention functions on the Behaviour Change Wheel, including education and persuasion (Michie et al. 2011). Several BCTs serve these functions, including ‘information about social and environmental consequences’ and ‘information about health consequences’ (Michie et al. 2014). They have been highlighted as potential BCTs for targeting barriers associated with ‘Social/Professional Role and Identity’ in other MECC-related research (Keyworth et al. 2019) and should be explored further to enhance future HCS implementation.
The impacts of HCS on service users were mixed, potentially due to the differences between participant groups. No significant differences were observed between pregnant women who did and did not receive the HCS intervention in gestational weight gain, concordance with gestational weight gain guidelines, or physical activity. However, there were some positive effects on sedentary behaviour in intervention participants. The lack of impact on gestational weight gain reflected the difficulties experienced by many women during pregnancy in improving weight outcomes and adhering to IOM weight-gain guidelines, as evidenced in several large RCTs (Syngelaki et al. 2019; Shieh et al. 2018). Evidence suggests that these difficulties are even more prominent for those that are overweight or obese before pregnancy (Jarman et al. 2016); therefore, it could be useful to support women to improve their health behaviours using HCS prior to conception. There was variation between studies in relation to changes in dietary quality as a result of HCS. Improvements were observed for pregnant women in Alberta, Canada, but declines in dietary quality were reported for participants attending SSCCs in Southampton, and these were significantly predicted by educational attainment. Discrepancies between results could therefore have been associated with differences between participants groups; however, educational attainment was not measured in the pregnant women. Future research could use this measure to assess its relationship with the impact of HCS across service user groups.
Declines were also observed in those attending SSCCs for intermediate outcomes, including self-efficacy and sense of control. However, the decline in sense of control was significantly less marked for those who had more exposure to HCS during the study period. This suggests that the intervention had a protective effect on this intermediate outcome, which is evidenced as being associated with better dietary quality and higher physical activity levels (Greaves et al. 2011; Ashford et al. 2010). The authors reported that, under more optimal circumstances and if repeated exposure was ensured, HCS could have potential to improve health outcomes for women accessing these services. Service users across studies did, however, find HCS acceptable, and experienced more benefits from their conversations with trained staff than those not trained in HCS, including feeling empowered. Such empowerment enables individuals to be active players in their own health (Guarneri et al. 2017) and is key to improving outcomes (Barker et al. 2011), providing support for HCS as an acceptable, person-centred, and effective approach to health behaviour change.
MECC studies were conducted nationwide and involved a wide range of staff trained in various local models. However, some did not specify where participants were recruited or what job roles they had. The involvement of service users in studies was very limited, highlighting the need for further research to assess the intervention in relation to its public reach and impact.
Only one study highlighted staff competence in delivering MECC; however, the statistical significance of findings was not reported (Tucker 2019). Four studies in total measured changes in confidence in supporting behaviour change, and mixed results were observed. Two studies highlighted increases in confidence pre- to post-training, suggesting that the programme successfully enhanced the self-efficacy of participants in delivering brief or very brief health-related interventions (BIs/VBIs). In contrast, two studies reported staff decreasing in confidence with their MECC skills or experiencing differing levels of confidence in discussing alcohol, smoking, weight, diet, and exercise. The latter has been evidenced in several studies that have reported the perceived challenges healthcare professionals face in raising health-related conversations regarding weight in particular. These challenges have been associated with the fear of disconnect and damage to the professional–patient relationship (McGowan, 2016; Bradbury et al. 2018), or even due to the healthcare professional seeing him/herself as being overweight (Brown and Thompson 2007). Training aimed at increasing skills and confidence in discussing weight in particular may enhance levels of engagement in MECC for lifestyle topics such as diet and exercise.
MECC was considered mostly acceptable to staff; however, discrepancies between perceptions of the value of training were observed (Nelson et al. 2013; Tucker 2019; Chisholm et al. 2020). Findings suggested that perceived acceptability of MECC training varies, depending upon staff groups and the model or programme of training they are exposed to, and some standardisation of MECC programmes could reduce ambiguities in the results of future evaluations. Staff were, however, supportive of MECC, acknowledged that it was part of everyone’s role, and saw the initiative as contributing to an organisational culture change which was more focused on prevention. Again, this complements the NHS Five Year Forward View: a plan for change within the NHS to improve public health, which highlights prevention as one of its three central themes (NHS England 2014).
Thematic analysis identified four main themes in relation to the barriers and facilitators to MECC implementation. These included evaluating MECC, system level influencers, staff capacity, and attitudes towards MECC. Despite barriers and facilitators being mapped to six TDFs in total, the majority were related to the ‘Environmental Context and Resources’ domain — a finding also observed in the HCS literature. This should therefore be targeted for future enhancement of MECC implementation. Workload, time constraints, lack of evidence of impact, lack of resources, and organisational culture were key barriers relating to this domain. As mentioned previously, workload, time, and resources constraints have been evidenced consistently as hindrances to behaviour change delivery (Um et al. 2013; Glowacki et al. 2019). Moreover, an organisational culture that is resistant to change has been evidenced as a barrier even for those that are motivated and competent in the use of interventions (Williams et al. 2015). High staff engagement, having a supportive infrastructure for staff, follow-ups with service users, and referrals to specialist services were, however, identified as facilitators to MECC implementation. The latter has been regarded as a feasible and common measure for evaluating the impact of MECC on service users (Chisholm et al. 2019). Moreover, improvements in health behaviours have been evidenced following MECC referrals (Moss and Bancroft 2019). Further research is warranted to explore the most effective methods of evaluating the local impact of MECC which may, in turn, encourage its delivery.
No studies evaluated the acceptability of MECC for service users, and only two assessed its impact on health outcomes. Moreover, there were no statistically significant findings reported. This highlights a considerable gap in the MECC literature compared to that of HCS, and further empirical research to establish the true impact of the intervention on public health is warranted.
Limitations and strengths
There are three key limitations to this review that must be acknowledged. Firstly, despite an exhaustive search in scientific databases, grey literature, and reference lists of identified studies, the possibility of having missed relevant studies cannot be ruled out. Secondly, raw data from the included studies could not be accessed; therefore, information about experiences, barriers, and facilitators of MECC reported by the authors was relied upon for data extraction and coding. Finally, there are currently no consistent methods of measuring the impact and perceptions of MECC, which could have contributed to some ambiguity in findings. Discrepancies in perceptions, experiences, and impacts of MECC are highly likely to be related to differences in training models and intervention aims. The development and introduction of some standardisation of training and aims could help tackle challenges associated with the evaluation of MECC as a behaviour change intervention. However, this review is the first to collate data from MECC and HCS interventions, so can inform future development and implementation of these examples of brief interventions for tackling lifestyle behaviour change at a population level.
Conclusion
There are gaps in the evidence base for both HCS and MECC, warranting further investigation of these behaviour change interventions. Despite several studies providing support for HCS in relation to acceptability and impact, these have involved only a small number of staff groups and service users. Further research to evaluate HCS for participants in a variety of roles/ accessing different services is needed. Such research could promote HCS as a component of MECC that can be effectively implemented by those beyond the Wessex region. This would facilitate a consistent method of MECC training and evaluation that could be adopted by other NHS trusts and organisations across the UK.
Data availability
Availability of data and material: All data generated or analysed during this study are available within the article (and its supplementary information files).
Code availability
N/A
References
Adam LM, Jarman M, Barker M, Manca DP, Lawrence W, Bell RC (2020) Use of healthy conversation skills to promote healthy diets, physical activity and gestational weight gain: results from a pilot randomised controlled trial. Patient Educ Couns 103(6):1134–1142
Arksey H, O'Malley L (2005) Scoping studies: towards a methodological framework. Int J Soc Res Methodol 8(1):19–32
Ashford S, Edmunds J, French DP (2010) What is the best way to change self-efficacy to promote lifestyle and recreational physical activity? A systematic review with meta-analysis. Br J Health Psychol 15(2):265–288
Atkins L, Michie S (2013) Changing eating behaviour: what can we learn from behavioural science? Nutr Bull 38(1):30–35
Baird J, Jarman M, Lawrence W, Black C, Davies J, Tinati T et al (2014) The effect of a behaviour change intervention on the diets and physical activity levels of women attending sure start Children’s Centres: results from a complex public health intervention. BMJ Open 4(7):e005290
Bandura A (1986) Social foundations of thoughts and action: a social cognitive theory. Prentice–Hall, Englewood Cliffs
Bandura A (1997) Self-efficacy: the exercise of control. Freeman, New York
Barker M, Lawrence W, Skinner TC, Haslam C, Robinson SM, Barker D (2008) Constraints on the food choices of women with lower educational attainment. Public Health Nutr 11:1229–1237
Barker M, Baird J, Lawrence W, Jarman M, Black C, Barnard K et al (2011) The Southampton Initiative for Health: a complex intervention to improve the diets and increase the physical activity levels of women from disadvantaged communities. J Health Psychol 16(1):178–191
Barker ME, Baird J, Tinati T, Vogel C, Strömmer S, Rose T et al (2017) Translating developmental origins: improving the health of women and their children using a sustainable approach to behaviour change. Healthcare 5:17–30
Black C, Lawrence W, Cradock S, Ntani G, Tinati T, Jarman M et al (2014) Healthy conversation skills: increasing competence and confidence in front-line staff. Public Health Nutr 17(3):700–707
Bradbury D, Chisholm A, Watson PM, Bundy C, Bradbury N et al (2018) Barriers and facilitators to health care professionals discussing child weight with parents: a meta-synthesis of qualitative studies. Br J Health Psychol 23(3):701–722
Braun V, Clarke V (2006) Using thematic analysis in psychology. Qual Res Psychol 3(2):77–101
Braun V, Clarke V (2019) Reflecting on reflexive thematic analysis. Qual Res Sport Exerc Health 11(4):589–597
Brown I, Thompson J (2007) Primary care nurses’ attitudes, beliefs and own body size in relation to obesity management. J Adv Nurs 60(5):535–543
Butler CC, Simpson SA, Hood K, Cohen D, Pickles T, Spanou C et al (2013) Training practitioners to deliver opportunistic multiple behaviour change counselling in primary care: a cluster randomised trial. BMJ 346:f1197
Cane J, O’Connor D, Michie S (2012) Validation of the theoretical domains framework for use in behaviour change and implementation research. Implement Sci 7(1):37
Cane J, Richardson M, Johnston M, Ladha R, Michie S (2015) From lists of behaviour change techniques (BCTs) to structured hierarchies: comparison of two methods of developing a hierarchy of BCTs. Br J Health Psychol 20(1):130–150
Chisholm A, Ang-Chen P, Peters S, Hart J, Beenstock J (2019) Public health practitioners’ views of the ‘making every contact count’ initiative and standards for its evaluation. J Public Health 41(1):e70–e77
Chisholm A, Byrne-Davis L, Peters S, Beenstock J, Gilman S, Hart J (2020) Online behaviour change technique training to support healthcare staff ‘make every contact count’. BMC Health Serv Res 20:1–11
Davies E, Kings A, Cornford-Hill M, Southwell C, Prabhakaran S, Haldane T et al (2014) PTH-029 lifestyle screening and brief interventions in a gastroenterology clinic. Gut 6:A221–A221
Dewhirst S, Speller V (2015) Wessex making every contact count (MECC) pilot: evaluation report. University of Southampton, Southampton, UK
Elwell L, Powell J, Wordsworth S, Cummins C (2014a) Health professional perspectives on lifestyle behaviour change in the paediatric hospital setting: a qualitative study. BMC Pediatr 14(1):1–8
Elwell L, Powell J, Wordsworth S, Cummins C (2014b) Health professional perspectives on lifestyle behaviour change in the paediatric hospital setting: a qualitative study. BMC Pediatr 14(1):71
Glowacki K, Weatherson K, Faulkner G (2019) Barriers and facilitators to health care providers’ promotion of physical activity for individuals with mental illness: a scoping review. Ment Health Phys Act 16:152–168
Greaves CJ, Sheppard KE, Abraham C, Hardeman W, Roden M, Evans PH, Schwarz P (2011) Systematic review of reviews of intervention components associated with increased effectiveness in dietary and physical activity interventions. BMC Public Health 11(1):1–12
Guarneri MR, Brocca MD, Piras L (2017) Patient’s empowerment and behaviour change: complementary approaches in EU projects PALANTE and PEGASO. eHealth 360:359–369
Handley MA, Gorukanti A, Cattamanchi A (2016) Strategies for implementing implementation science: a methodological overview. Emerg Med J 33(9):660–664
Health Education England (2018) Making every contact count: case studies. Health Education England, London. http://www.makingeverycontactcount.co.uk/implementing/case-studies/. Accessed 15 June 2020
Jarman M, Yuan Y, Pakseresht M, Shi Q, Robson PJ, Bell RC (2016) Patterns and trajectories of gestational weight gain: a prospective cohort study. CMAJ Open 4(2):E338
Jarman M, Adam L, Lawrence W, Barker M, Bell RC (2019) Healthy conversation skills as an intervention to support healthy gestational weight gain: experience and perceptions from intervention deliverers and participants. Patient Educ Couns 102(5):924–931
Jepson RG, Harris FM, Platt S, Tannahill C (2010) The effectiveness of interventions to change six health behaviours: a review of reviews. BMC Public Health 10(1):538
Keyworth C, Epton T, Goldthorpe J, Calam R, Armitage CJ (2018) Are healthcare professionals delivering opportunistic behaviour change interventions? A multi-professional survey of engagement with public health policy. Implement Sci 13(1):122
Keyworth C, Epton T, Goldthorpe J, Calam R, Armitage CJ (2019) ‘It's difficult, I think it's complicated’: health care professionals’ barriers and enablers to providing opportunistic behaviour change interventions during routine medical consultations. Br J Health Psychol 24(3):571–592
Lafreniere KC, McArthur A (2019) Enhancing existing communication channels for large-scale health interventions: making every contact count in the United Kingdom. In: Basil D, Diaz-Meneses G, Basil M. (eds). Social marketing in action. Springer, Heidelberg, pp 247–256
Lawrence W, Skinner C, Haslam C, Robinson S, Inskip H, Barker D et al (2009) Why women of lower educational attainment struggle to make healthier food choices: the importance of psychological and social factors. Psychol Health 24(9):1003–1020
Lawrence W, Keyte J, Tinati T (2011) A mixed-methods investigation to explore how women living in disadvantaged areas might be supported to improve their diets. J Health Psychol 17(6):785–798
Lawrence W, Black C, Tinati T, Cradock S, Begum R, Jarman M et al (2016) ‘Making every contact count’: evaluation of the impact of an intervention to train health and social care practitioners in skills to support health behaviour change. J Health Psychol 21(2):138–151
Lawrence W, Vogel C, Strömmer S, Morris T, Treadgold B, Watson D et al (2020) How can we best use opportunities provided by routine maternity care to engage women in improving their diets and health? Matern Child Nutr 16(1):e12900
McGowan BM (2016) A practical guide to engaging individuals with obesity. Obesity facts, 9(3): 182-192.
Michie S, Van Stralen MM, West R (2011) The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci 6(1):42
Michie S, Atkins L, West R (2014) The behaviour change wheel: a guide to designing interventions. Silverback, London
Moher D, Liberati A, Tetzladd J, Altman DG, The PRISMA Group (2009) Preferred reporting for systematic reviews and meta-analyses: the PRISMA statement. Open Med 3(3):123–130
Moss C, Bancroft D (2019) Developing an evidence-based making every contact count (MECC) model of practice within MSK physiotherapy services. Physiotherapy 105:e169
Mulroe J, Collins C, Cuddihy J, Fawsitt R, Gleeson M, Jennings S et al (2017) Making Every Contact Count (MECC)—chronic disease risk factor and brief advice recording. Int J Integr Care 17(5):A159
Munn Z, Peters MD, Stern C, Tufanaru C, McArthur A, Aromataris E (2018) Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol 18(1):1–7
National Institute for Health and Care Excellence (2014) Behaviour change: individual approaches. NICE, London. https://www.nice.org.uk/guidance/PH49. Accessed 15 June 2020
National Institute of Health and Clinical Excellence (2007) Behaviour change at population, community and individual levels (Public Health Guidance 6). NICE, London
Nelson A, De Normanville C, Payne K, Kelly MP (2013) Making every contact count: an evaluation. Public Health 127(7):653–660
NHS (2016) 2017/18 NHS standard contract. NHS, London. https://www.england.nhs.uk/nhs-standard-contract/17-18/. Accessed 15 June 2020
NHS England (2014) The forward view into action: planning for 2015/16. NHS, London. https://www.england.nhs.uk/wp-content/uploads/2014/12/forward-view-plning.pdf. Accessed 18 June 2020
Nilsen P (2015) Making sense of implementation theories, models and frameworks. Implement Sci 10(1):53
Peters MDJ, Godfrey C, McInerney P, Munn Z, Tricco AC, Khalil H (2020) Chapter 11: scoping reviews. In: Aromataris E, Munn Z (eds) JBI manual for evidence synthesis. JBI, Adelaide, South Australia. https://doi.org/10.46658/JBIMES-20-12
Pham MT, Rajić A, Greig JD, Sargeant JM, Papadopoulos A, McEwen SA (2014) A scoping review of scoping reviews: advancing the approach and enhancing the consistency. Res Synth Methods 5(4):371–385
Public Health England, NHS England, and Health Education England (2016) Making Every Contact Count Consensus Statement. Public Health England, NHS England, Health Education England, London. http://mecc.yas.nhs.uk/media/1014/making_every_contact_count_consensus_statement.pdf. Accessed 18 June 2020
Rosenstock IM (1974) Historical origins of the Health Belief Model. Health Educ Monogr 2(4):328–335
Scarborough P, Bhatnagar P, Wickramasinghe KK, Allender S, Foster C, Rayner M (2011) The economic burden of ill health due to diet, physical inactivity, smoking, alcohol and obesity in the UK: an update to 2006–07 NHS costs. J Public Health 33(4):527–535
Shieh C, Cullen DL, Pike C, Pressler SJ (2018) Intervention strategies for preventing excessive gestational weight gain: systematic review and meta-analysis. Obes Rev 19(8):1093–1109
Sturgiss E, Haesler E, Elmitt N, Van Weel C, Douglas K (2017) Increasing general practitioners' confidence and self-efficacy in managing obesity: a mixed methods study. BMJ Open 7(1):e014314
Syngelaki A, Sequeira Campos M, Roberge S, Andrade W, Nicolaides KH (2019) Diet and exercise for preeclampsia prevention in overweight and obese pregnant women: systematic review and meta-analysis. J Matern Fetal Neonatal Med 32(20):3495–3501
Tinati T, Lawrence W, Ntani G, Black C, Cradock S, Jarman M et al (2012) Implementation of new healthy conversation skills to support lifestyle changes–what helps and what hinders? Experiences of Sure Start Children’s Centre staff. Health Soc Care Commun 20(4):430–437
Tucker C (2019) Increasing the number of healthy lifestyle conversations that a multi-disciplinary community team has with its patients. Physiotherapy 105:e143–e144
Um IS, Armour C, Krass I, Gill T, Chaar BB (2013) Weight management in community pharmacy: what do the experts think? Int J Clin Pharm 35(3):447–454
Webster S (2018) G435 (P) making every contact count—a paediatric pilot training programme in Wales. Arch Dis Child 103:A177–A178
Williams B, Perillo S, Brown T (2015) What are the factors of organisational culture in health care settings that act as barriers to the implementation of evidence-based practice? A scoping review. Nurs Educ Today 35(2):e34–e41
Wills J, Ion V (2014) Implementing ‘making every contact count’: a scoping review. London South Bank University, London
Wills J, Kelly M (2017) What works to encourage student nurses to adopt healthier lifestyles? Findings from an intervention study. Nurs Educ Today 48:180–184
World Health Organization (2013) Global action plan for the prevention and control of noncommunicable diseases 2013–2020. WHO, Geneva. http://www.who.int/nmh/publications/9789241597418/en/index.html. Accessed 22 June 2020
Acknowledgements
The authors would like to acknowledge the contribution of those that assisted with screening in this review; Bethany Hawkings, Violet Henderson, Louise Reeves, Lara Romero Riego, and Natasha Williams.
Funding
PhD studentship funded by University of Bath and Health Education England.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. The review methodology was developed by Rachel Perry and Amelia Parchment. Data collection and analysis were performed by Amelia Parchment. The first draft of the manuscript was written by Amelia Parchment and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Ethics approval
Ethical approvals were not required for this research.
Consent to participate
N/A
Consent for publication
N/A
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
ESM 1
(DOCX 34 kb)
Appendix
Appendix
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Parchment, A., Lawrence, W., Perry, R. et al. Making Every Contact Count and Healthy Conversation Skills as very brief or brief behaviour change interventions: a scoping review. J Public Health (Berl.) 31, 1017–1034 (2023). https://doi.org/10.1007/s10389-021-01653-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10389-021-01653-4