
Abstract
Objectives
The EQ-5D-5L is a generic preference-based quality-of-life measure for which the corresponding Portuguese population value set was only recently developed. This study sought to establish EQ-5D-5L population norms for Portugal and to identify significant relationships with sociodemographic variables.
Methods
The research was based on a representative sample of Portugal’s general population (n = 1006) aged 18 or older. The sample was stratified by gender, age group, and geographical region. The respondents were interviewed by telephone and asked to value their own state of health using both the EQ-5D-5L description system and the EuroQol-Visual Analogue Scale (EQ VAS).
Results
The estimated mean EQ-5D-5L index for Portugal’s general population is 0.887 (standard error [SE] = 0.0051), and the EQ VAS score was estimated as 76.0 (SE = 0.640). One-third of the population reported being in the best health state (11111). Women, individuals 70 years old or more and people with low education or a chronic disease reported a lower EQ-5D-5L index score (p < 0.001). Residents in the Azores and the Algarve reported higher health utility scores.
Conclusions
The EQ-5D-5L Portuguese population norms obtained can be used as reference scores. These norms are consistent with other countries’ population norms. The findings facilitate clinical, economic, and policy decision-making processes and provide a fuller understanding of the Portuguese population’s health-related quality of life.
Similar content being viewed by others

Introduction
The EQ-5D is a generic preference-based quality-of-life measure that provides supporting data for clinical and policy decisions. EQ-5D utility values can easily be converted into quality-adjusted life years (QALY) and used to conduct cost–utility analysis in economic evaluations [1].
The five-level (5L) EQ-5D version was introduced by the EuroQol Group a few years ago. The new instrument expands the descriptive system from 3 to 5 severity levels within each of the 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression) [2]. The revised measure produces a total of 3125 distinct health states, identifying each health state by a five-digit code expressing each dimension’s severity level, with 11111 representing the best and 55555 the worst possible health states [2].
In 2019, a value set was derived for the Portuguese population’s preferences, assigning societal values to all 3125 health states generated by the EQ-5D-5L [1]. Portugal’s Infarmed (i.e., National Authority of Medicaments and Health Products) currently recommends, in its official methodological guidelines for economic evaluations of health technologies, that decision-makers use a Portuguese value set and the EQ-5D-5L rather than other measures to assess health-related quality of life (HRQoL) [3].
Population norms can function as reference values that facilitate comparisons among patients with specific conditions with data on the average person of a similar age and/or gender within the same community [4]. Normative data are a useful guide for those seeking to interpret the outcomes of health economic evaluations. EQ-5D-5L population norms have been developed for multiple countries and regions [4], namely, Europe [5,6,7,8,9,10,11,12,13,14,15], Asia [16,17,18,19,20,21,22], the Americas [23,24,25,26,27], and Oceania [28, 29].
The EQ-5D-3L population norms for Portugal were estimated a few years ago [30]. As Portugal did not yet have population norms for the EQ-5D-5L, the present study focused on obtaining the relevant nationally representative normative data defined by gender, age group, and geographical region to establish the EQ-5D-5L population norms for Portugal.
Methods
Sampling design
The target population was 8.7 million Portuguese adults, aged 18 and older [31]. The current research’s aim was to estimate the EQ-5D-5L mean index value for the subpopulations of interest defined by gender (two categories), age group (four groups), and region (seven regions). Thus, stratified random sampling was applied to gather a representative sample of the general population. In addition, the global sample was proportionally allocated to each stratum, which facilitated statistical analysis, since all the sampling units had equal probabilities of being selected for the sample [32].
The sample size calculation [32: 128] used the population size of each stratum in the Portuguese 2011 census [31] and auxiliary information from the EQ-5D-3L population norms survey [30]. Assuming a 95% confidence level and a maximum absolute sampling error of 0.015 (i.e., equivalent to a relative sampling error of 1.9%), the global sample was set at 998 individuals. This sample could be used to estimate the overall EQ-5D-5L mean index.
A final sample of 1006 individuals was ultimately surveyed, which was proportionally allocated to the 56 strata.
The survey was conducted between November 2015 and January 2016 by a market research company. Four trained interviewers collected the data via telephone interviews using a Computer-Assisted Telephone Interviewing system. Mobile and landline telephone numbers were selected using a computer algorithm to ensure a random sample using the Random Digit Dialing method. Among people living in the dialed household, a person with the birthday nearest the interview date was specifically contacted.
Calls were made between 6 and 10 pm when residents were most likely to be at home. Up to two callbacks were made after the first call if no one answered or the line was busy. The interviewee was given the option of scheduling the interview on another day and/or at a different time to ensure each individual’s cooperation. Only one interview was conducted per household.
Each respondent answered the survey questionnaire after that person’s eligibility was confirmed based on the target population and sampling design. The telephone interview script was developed for this study by the market research company and, on average, each telephone call lasted 14 min. The company ran a pilot test of the entire survey process in October 2015. The company started the fieldwork only after the research team evaluated the test’s results and found them acceptable.
The survey consisted of three parts. The first was a general welcome extended to the respondents. After the interviewees passed the eligibility check, the interviewers explained the study’s purpose, and the respondents were asked if they agreed to participate in the survey. All interviewees were also informed that no wrong answers existed and that their data would remain anonymous and confidential.
The second part was the survey questions. The data collection instrument included three sections: the EQ-5D-5L Portuguese version that included both the EQ-5D-5L description system and the EuroQol-Visual Analogue Scale (EQ VAS), the Short Form-12 Health Survey (SF-12) Portuguese version and sociodemographic questions. The topics covered by all the questionnaire’s sections were explained to the respondents before the questions were asked to provide a context for the survey. The scales were also carefully presented with each question. As the SF-12 does not fall within the scope of this manuscript, its results are not presented here.
The last part was a general thank you for the interviewee’s cooperation and a goodbye. At this stage, the interviewees were also informed that they might be contacted again in the future for quality control purposes. The survey quality control and monitoring were based on direct supervision and a third party listening to telephone calls for 10% of the global sample. In addition, 10% of the sample was randomly cross-questioned by telephone.
The principles of anonymity, confidentiality, and individual privacy were ensured throughout the research. No incentive (i.e., monetary or non-monetary) was offered to the respondents. The National Data Protection Commission approved the study (i.e., Deliberation no. 1737).
Statistical analysis
The data analysis was conducted in three stages. First, the Portuguese value set [1] was used to derive the EQ-5D-5L index. Second, descriptive statistics were generated to profile the sample. Finally, inferential statistics techniques were applied to estimate the EQ-5D-5L parameters of interest (e.g., mean, quartiles, and proportions). The EQ-5D-5L index and answers’ distribution across the dimensions were analyzed globally and by sociodemographic characteristics. All inferential analyses considered the survey’s specific sampling design. Direct comparisons were also made between the EQ VAS results from the 5L and the EQ VAS data from the EQ-5D-3L Portuguese population norms [30]. The ceiling effect was analyzed globally and by sociodemographic groups. To further inspect the strength of the ceiling effect, EQ VAS scores for both the 3L and the 5L were compared within the respondents that reported full health (11111).
No adjustments were needed to compensate for unequal selection probabilities when estimating the EQ-5D-5L parameters at the strata level, but corrections had to be made when estimating these parameters at the level of other domains (e.g., those defined by marital status and chronic disease). In the latter case, the sampling weights were adjusted using domain estimation methods [33]. The correlation between the EQ-5D-5L index and EQ VAS scores was evaluated based on Spearman’s rank correlation coefficient (ρ). Since these scores have trouble adjusting to a symmetric distribution (e.g., a normal distribution), the differences between subgroups defined by sociodemographic variables were assessed using the Welch’s tests.
To deeper analyze the health problems reported by the Portuguese population, we have also observed the distribution of responses given in levels 2 and 3, as well as 4 and 5, in the EQ-5D dimensions. The objective was to see what dimensions are hampered simultaneously.
All data analyses were performed using IBM SPSS Statistics version 27 software.
Results
Sample
The sample’s main characteristics are shown in Table 1. This profile matches the general population’s characteristics in terms of gender, age group, and region (i.e., the stratification variables), and the profile is similar regarding other variables (i.e., marital status, employment status, and household). However, the sample has a larger proportion of individuals with a post-secondary and higher education diploma (i.e., bachelor’s, master’s, or doctoral degree) than the general population does.
The majority of the respondents were female (53.4%). Most respondents were middle-aged or older as the participants aged between 30 and 49 years were the sample’s largest age group (35.1%). The majority were married or living with a partner (57.9%). and close to half of the respondents (45.8%) indicated that they had a low level of education. In addition, 51.1% reported that they were employed and 27.3% were retired. Most respondents lived in a household with 3–4 members (48.7%) and the majority did not have a chronic disease (53.5%). Finally, about a third of the participants said their net monthly earnings fell between €1000 and €1999 (34.6%).
Norms
The most frequent health level reported by the Portuguese population for all EQ-5D-5L dimensions is ‘no problems’. More specifically, Table 2 shows that 91.2% of the population selected the ‘no problems’ option in the self-care dimension, while about three-quarters have no problems in the mobility and usual activities’ dimensions. A full 60.9% also have no problems with anxiety and/or depression, and 45.9% do not experience pain and/or discomfort.
The results further highlight that one-third of the population has ‘slight problems’ with pain and/or discomfort. This study overall detected a lower percentage of individuals with no problems in all EQ-5D-5L dimensions compared to the Portuguese population norms previously established for the EQ-5D-3L [30]. That is, the present findings include 74.9 versus 83.3% for mobility, 91.2 versus 95.2% for self-care, 75.9 versus 83.7% for usual activities, 45.9 versus 55.3% for pain and/or discomfort, and 60.9 versus 65.6% for anxiety and/or depression.
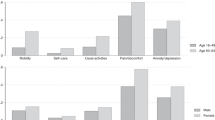
The estimated frequencies of each EQ-5D-5L dimension by gender and age group are presented in supplementary material Table S1. The results reveal that Portuguese women report more problems than men do in all EQ-5D-5L dimensions. The biggest difference between these gender groups appears in the pain/discomfort dimension and the smallest divergence in self-care. The findings also show that that older groups report more severe problems than younger respondents do. The increase of the number of problems along with the increase of age in all dimensions was expected, but these differences are most pronounced in the mobility, usual activities, and pain/discomfort dimensions. However, some dimensions worsen quickly than others, as can be inferred from the graphs included in Supplementary material S2. For instance, dimensions mobility and usual activities seem to degrade with age quicker than the others. On the other hand, self-care and anxiety/depression worsen slower with age.
Table 3 lists the most frequently reported EQ-5D-5L health states. In total, 184 health states out of a total of 3125 were reported by the surveyed individuals, three-quarters of whom selected the top 18 health states in Table 3. One-third of the population reported the best health state (i.e., 11111), for which a EQ-5D-5L index score of 1.000 and mean EQ VAS score of 86.5 were estimated. The next three most frequently reported health states are 11121 (12.2%), 11122 (7.1%), and 11112 (6.2%). The mean EQ-5D-5L index scores estimated for these health states are 0.959, 0.923, and 0.964, respectively, while the EQ VAS scores are 81.6, 78.3, and 84.7.
Table 4 presents the overall EQ-5D-5L population norms (EQ-5D-5L index and EQ-5D VAS) and by main sociodemographic characteristics. The estimated mean EQ-5D-5L index score for Portugal’s general population is 0.887 (SE = 0.0051), and the overall mean EQ VAS score is 76.0 (SE = 0.640). These index scores are moderately positively correlated (ρ = 0.57; p < 0.001). As expected, the Kolmogorov–Smirnov test confirmed that each distribution does not even roughly follow a normal distribution (both with p < 0.001).
Half of the general population reported an EQ-5D-5L index score greater than or equal to 0.959, while about one-third reported the highest utility score (EQ-5D-5L index = 1.000). Table 4 further shows that women have a statistically significantly lower mean EQ-5D-5L index score than men do (0.863 vs 0.914; p < 0.001). The mean EQ-5D-5L index scores show a statistically significant difference between individuals in varied age groups (p < 0.001). More specifically, the mean EQ-5D-5L score for individuals aged 18–29 is 0.962, while the score for individuals aged 70 years and older is 0.790.
Table 4 also reveals that the mean EQ-5D-5L index score differs significantly by geographical region, marital status, education, and chronic disease (all with p < 0.001). For instance, people living in the Azores and the Algarve report higher utility scores than individuals living in the other regions do. Furthermore, people with a low level of education or a chronic disease have the smallest utility scores. The mean EQ-5D-5L and EQ VAS index scores by other sociodemographic characteristics are listed in Supplementary Material Table S3.
Table 5 shows the distribution of health problems (responses given in levels 2–3 or 4–5) in each EQ-5D dimensions. Considering levels 2–3 of mobility, minor problems were found in 21.4% of the respondents, with 23.8% also reporting minor problems in self-care, 53.7% in usual activities, 72.9% in pain/discomfort, and 48.1% in anxiety/depression. Of the individuals who reported levels 2–3 in self-care, more than half also reported 2 or 3 on mobility, usual activities, pain-discomfort, and anxiety-depression. On the other hand, of the individuals who reported 2–3 in usual activities, less than 30% reported this level of problems in the self-care and more than a half in the other EQ-5D dimensions. Most individuals who reported 2–3 on pain/discomfort do not have the same level of severity in the remaining dimensions. It is also worth noting that of the individuals who reported 2–3 in anxiety/depression, only in dimension pain/discomfort, there was more than half of the individuals reporting this level of problems. The same rational applies to the other dimensions and levels.
Additionally, the Spearman rank correlation coefficients show, as expected, that all dimensions are moderately-to-strongly associated. The association is higher between dimensions mobility/self-care, mobility/usual activities, self-care/usual activities, and usual activities/pain and/or discomfort, showing that reported problems in functional dimensions, such as mobility or self-care, may hamper problems in other dimensions.
As already seen before, most of the problems occur in the dimension pain/discomfort and anxiety/depression, which gives to the Portuguese values a higher relative importance for these two dimensions comparing to other more functional ones. This means that, in the Portuguese value set, the disutility we obtain when we skip levels in more functional dimensions (mobility, self-care, and usual activities) is much lower when compared to pain/discomfort or anxiety/depression. This phenomenon is not always reported in other countries [34].
Comparison of EQ-5D-5L and EQ-5D-3L results
Table 4 also includes the EQ VAS data from the EQ-5D-3L Portuguese population norms [30]. Although the EQ-5D descriptive system of both instruments is different, the EQ VAS remains the same. As expected, there are no statistically significant differences in overall EQ VAS according to the version of the EQ-5D (p = 0.240).
Table 6 presents the comparison of EQ VAS 5L in the population that reports full health in this study with the EQ VAS 3L in the population that reported full health in the EQ-5D-3L Portuguese population norms [30]. It also shows the ceiling effect for both the 5L and the 3L [30].
The results reveal a lower ceiling effect for the 5L version as compared to the 3L version as a lower proportion of the population reported ‘no problems’ for each dimension for the 5L compared with the 3L for the general population sample [30]. However, a considerable proportion of the population indicated that they are in full health (33.2%). More than one-fifth of the Portuguese population also evaluated their health as above 90 on the EQ VAS scale, and 9.3% chose ‘the best health you can imagine’, suggesting that the ceiling effect is consistent with the EQ VAS scores.
Table 6 also shows that the reported EQ VAS is similar in both studies as was expected, since the EQ VAS is presented in the same way in both versions of the instruments.
Discussion
This study sought to estimate normative EQ-5D-5L values for Portugal and to examine various sociodemographic variables’ relationships with the data based on a representative sample of Portugal’s general population. Comparisons of the results with other countries need to be made with caution as researchers adopt different methodologies that are then implemented in specific cultural settings. The findings for each country should, at least in part, take these cultural differences into account.
The estimated mean EQ-5D-5L index for Portugal’s general population is 0.887 and 76.0 for the EQ VAS, and the results show that both index scores are strongly negatively or left skewed. These scores are consistent with those found for other countries or regions [e.g., 5, 8, 11, 12, 14, 22, 25, 28, 29] and with the previous Portuguese EQ-5D-3L norms study [30]. Portuguese health utility scores are somewhat lower than those for various other nations [e.g., 9, 10, 16, 17, 23, 26].
The relative lower scores found in the present study are not surprising. Traditional cultural patterns tend to incline the Portuguese population toward reporting lower health status and quality-of-life values than those of other countries—even when the respondents have similar health indicators to those of other nations [33]. However, about one-third (33.3%) of the population registered ‘no problems’ across all dimensions (i.e., health status 11111). More than one-fifth of the population also valued their health above 90 on the EQ VAS. The second most frequently reported health status (12.2%) was 11121, namely, only mild pain or discomfort, with exactly the same frequency as found for the United States (US) [27].
Comparisons between the EQ-5D-5L results with the EQ-5D-3L populations norms study [30] were made. As expected, the EQ VAS overall results were similar, as well as the EQ VAS results within individuals reporting full health.
This ceiling effect was previously observed in young Portuguese adults [35] and the general population by Craig et al. [36]. Overall, the present study’s percentages are higher than those for Quebec (20.8%) [25] or Slovenia [15] and similar to the US estimates [27] but better than the figures for other countries, which generally have percentages greater than 40% [e.g., 7, 8, 10, 12, 14, 16, 20, 23, 28]. The Portuguese population’s lower ceiling effect may thus represent a substantial increase in the EQ-5D-5L’s sensitivity as compared to that of the EQ-5D-3L. Studies conducted elsewhere have also shown that the EQ-5D-5L’s discriminatory power has increased compared to the EQ-5D-3L [35]. The current results are, therefore, similar with those of prior research (e.g., Germany [8]).
The present study additionally detected heterogeneity across dimensions. For instance, pain/discomfort is the dimension in which more people selected severe or extreme scores, with the mobility dimension coming next. This behavior is similar to that of other European countries [e.g., 15], as well as of the US [27] and South Australia [28].
In addition, females, older individuals, less educated citizens, and patients with chronic conditions report having a statistically significant lower EQ-5D-5L index score. Similar findings have again been reported for various other countries (e.g., [5, 8, 18, 25]). In contrast, males in Ireland [9] and China [16] present lower scores.
Strengths and limitations
The present research’s most obvious strength is its large sample, which is representative of the Portuguese population and stratified by gender, age group, and geographical region. However, the sample suffers from an overrepresentation of highly educated individuals, as happened in a parallel study of Bulgarians [6]. Regardless of this issue, the current sample facilitated an exploration of how specific sociodemographic variables affect EQ-5D-5L index scores.
Another potential limitation is that survey interviews, particularly the one conducted by phone, can be associated with biases, such as the ones derived from non-uniform interviews. To reduce this risk, the data were collected by a market research company that applied a strict methodology based on a Computer-Assisted Telephone Interviewing system with Random Digit Dialing of mobile and landline numbers.
Finally, given that these data were collected in a pre-COVID era, it may be seen as a potential limitation of this study. However, this may also strength the importance of this kind of studies. In fact, researchers that aim at studying the impact of outbreaks such as COVID-19 will be able to compare their findings with the HRQoL of the Portuguese general population (e.g., [37]).
Conclusion
This study derived the Portuguese population norms for the EQ-5D-5L based on a representative sample of Portugal’s general population aged 18 or older. The scores obtained can be used as a reference point for a preference-based quality-of-life measure in policy-related decision-making processes, thereby facilitating the assessment of disease burden and the monitoring of health status and inequalities over time. The norms defined provide benchmarks that help ensure more valid interpretations of general populations’ health and comparisons between studies. From this point onward, researchers can also use and interpret QALYs for Portugal’s general adult population particularly when conducting cost-effectiveness and/or utility analysis or resource allocation studies focused on HRQoL.
Data availability statement
The data that support the findings of this study are available from the corresponding author, LNF, upon reasonable request.
References
Ferreira, P.L., Antunes, P., Ferreira, L.N., et al.: A hybrid modelling approach for eliciting health state preferences: the Portuguese EQ-5D-5L value set. Qual. Life Res. 28, 3163–3175 (2019)
Herdman, M., Gudex, C., Lloyd, A., Janssen, M., Kind, P., Parkin, D., et al.: Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 20(10), 1727–1736 (2011)
Perelman, J., Soares, M., Mateus, C., Duarte, A., Faria, R., Ferreira, L., Saramago, P., Veiga, P., Furtado, C., Caldeira, S., Teixeira, M.C., Sculpher, M.: Methodological guidelines for economic evaluation studies of health technologies. INFARMED—National Authority of Medicines and Health Products, I.P., Lisbon. https://www.infarmed.pt/web/infarmed-en/human-medicines (2019). Accessed 25 June 2021
Szende, A., Janssen, B., Cabases, J.: Self-Reported Population Health: An International Perspective Based on EQ-5D. Springer, Dordrecht (2014)
Van Wilder, L., Charafeddine, R., Beutels, P., Bruyndonckx, R., Cleemput, I., Demarest, S., De Smedt, D., Hens, N., Scohy, A., Speybroeck, N., Van der Heyden, J., Yokota, R., Van Oyen, H., Bilcke, J., Devleesschauwer, B.: Belgian population norms for the EQ-5D-5L, 2018. Qual. Life Res. (2021). https://doi.org/10.1007/s11136-021-02971-6
Encheva, M., Djambazov, S., Vekov, T., et al.: EQ-5D-5L Bulgarian population norms. Eur. J. Health Econ. 21, 1169–1178 (2020)
Feng, Y., Devlin, N., Herdman, M.: Assessing the health of the general population in England: how do the three- and five-level versions of EQ-5D compare? Health Qual. Life Outcomes 13, 1–16 (2015)
Grochtdreis, T., Dams, J., König, H.H., Konnopka, A.: Health-related quality of life measured with the EQ-5D-5L: estimation of normative index values based on a representative German population sample and value set. Eur. J. Health Econ. 20(6), 933–944 (2019)
Hobbins, A., Barry, L., Kelleher, D., O’Neill, C.: The health of the residents of Ireland: population norms for Ireland based on the EQ-5D-5L descriptive system—a cross sectional study. HRB Open Res. 1, 22 (2018)
Scalone, L., Cortesi, P.A., Ciampichini, R., Cesana, G., Mantovani, L.G.: Health related quality of life norm data of the Italian general population: results using the EQ-5D-3L and EQ-5D-5L instruments. Epidemiol. Biostat. Public Health 12(3) (2015)
Hołownia-Voloskova, M., Tarbastaev, A., Golicki, D.: Population norms of health-related quality of life in Moscow, Russia: the EQ-5D-5L-based survey. Qual. Life Res. 30, 831–840 (2021). https://doi.org/10.1007/s11136-020-02705-0
Golicki, D., Niewada, M.: EQ-5D-5L Polish population norms. Arch. Med. Sci. 13(1), 191–200 (2017)
Garcia-Gordillo, M.A., Adsuar, J.C., Olivares, P.R.: Normative values of EQ-5D-5L: in a Spanish representative population sample from Spanish health survey, 2011. Qual. Life Res. 25(5), 1313–1321 (2016)
Hernandez, G., Garin, O., Pardo, Y., et al.: Validity of the EQ-5D-5L and reference norms for the Spanish population. Qual. Life Res. 27, 2337–2348 (2018)
Prevolnik Rupel, V., Ogorevc, M.: EQ-5D-5L Slovenian population norms. Health Qual. Life Outcomes 18, 333 (2020). https://doi.org/10.1186/s12955-020-01584-w
Yabg, Z., Busschbach, J., Liu, G., et al.: EQ-5D-5L norms for the urban Chinese population in China. Health Qual. Life Outcomes 16, 210 (2018)
Wong, E.L., Cheung, A.W., Wong, A.Y., Xu, R.H., Ramos-Goñi, J.M., Rivero-Arias, O.: Normative profile of health-related quality of life for Hong Kong general population using preference-based instrument EQ-5D-5L. Value Health 22(8), 916–924 (2019)
Shiroiwa, T., Fukuda, T., Ikeda, S., et al.: Japanese population norms for preference-based measures: EQ-5D-3L, EQ-5D-5L, and SF-6D. Qual. Life Res. 25(3), 707–719 (2016)
Abdin, E., Subramaniam, M., Vaingankar, J.A., Luo, N., Chong, S.A.: Measuring health-related quality of life among adults in Singapore: population norms for the EQ-5D. Qual. Life Res. 22(10), 2983–2991 (2013)
Kim, T.H., Jo, M.W., Lee, S.I., et al.: Psychometric properties of the EQ-5D-5L in the general population of South Korea. Qual. Life Res. 22(8), 2245–2253 (2013)
Emrani, Z., Akbari Sari, A., Zeraati, H., et al.: Health-related quality of life measured using the EQ-5D-5L: population norms for the capital of Iran. Health Qual. Life Outcomes 18, 108 (2020). https://doi.org/10.1186/s12955-020-01365-5
Nguyen, L.H., Tran, B.X., Le, Q.N.H., Tran, T.T., Latkin, C.A.: Quality of life profile of general Vietnamese population using EQ-5D-5L. Health Qual. Life Outcomes 15(1), 199 (2017)
Guertin, J.R., Feeny, D., Tarride, J.-E.: Age- and sex-specific Canadian utility norms, based on the 2013–2014 Canadian community health survey. CMAJ 190(6), E155–E161 (2018)
Bailey, H.H., Janssen, M.F., Varela, R.O., Moreno, J.A.: EQ-5D-5L population norms and health inequality in Colombia. Value Health Reg. Issues 26, 24–32 (2021). https://doi.org/10.1016/j.vhri.2020.12.002
Poder, T.G., Carrier, N., Kouakou, C.R.C.: Quebec health-related quality-of-life population norms using the EQ-5D-5L: decomposition by socio-demographic data and health problems. Value Health 23(2), 251–259 (2020)
Augustovski, F., Rey-Ares, L., Irazola, V., Garay, O.U., Gianneo, O., Fernández, G., et al.: An EQ-5D-5L value set based on Uruguayan population preferences. Qual. Life Res. 25, 323–333 (2016)
Jiang, R., Bas Janssen, M.F.B., Pickard, A.S.: US population norms for the EQ-5D-5L and comparison of norms from face-to-face and online samples. Qual. Life Res. 30, 803–816 (2021). https://doi.org/10.1007/s11136-020-02650-y
McCaffrey, N., Kaambwa, B., Currow, D.C., Ratcliffe, J.: Health-related quality of life measured using the EQ-5D-5L: South Australian population norms. Health Qual. Life Outcomes 14(1), 133 (2016)
Sullivan, T., Turner, R.M., Derrett, S., Hansen, P.: New Zealand population norms for the EQ-5D-5L constructed from the personal value sets of participants in a national survey. Value Health 24(9), 1308–1318 (2021)
Ferreira, L.N., Ferreira, P.L., Pereira, L.N., Oppe, M.: EQ-5D Portuguese population norms. Qual. Life Res. 23(2), 425–430 (2014)
Portuguese Statistical Office. (2012). Census 2011 Resultados Definitivos—Portugal. Lisbon, INE
Xufre, P., Pereira, L.N., Coelho, P.S., Pinheiro, J.A.: As Sondagens: Princípios, Metodologias e Aplicações, 2nd edn. Escolar Editora, Lisboa (2021)
Eurostat: Quality of Life. https://ec.europa.eu/eurostat/web/products-eurostat-news/-/wdn-20210831-1. Accessed 27 June 2021
Devlin, N., Roudijk, B., Ludwig, K. (eds.): Value Sets for EQ-5D-5L: A Compendium, Comparative Review & User Guide. Springer, Cham (2022)
Ferreira, L.N., Ferreira, P.L., Ribeiro, F.P., Pereira, L.N.: Comparing the performance of the EQ-5D-3L and the EQ-5D-5L in young Portuguese adults. Health Qual. Life Outcomes 14, 89 (2016)
Craig, B.M., Pickard, A.S., Lubetkin, E.I.: Health problems are more common, but less severe when measured using newer EQ-5D versions. J. Clin. Epidemiol. 67(93), 99 (2014). https://doi.org/10.1016/j.jclinepi.2013.07.011
Ferreira, L.N., Pereira, L.N., Brás, M., Ilchuk, K.: Quality of life under COVID-19 quarantine. Qual. Life Res. 30, 1389–1405 (2021). https://doi.org/10.1007/s11136-020-02724-x
Acknowledgements
The authors are thankful to the anonymous reviewers for their constructive comments and suggestions which have considerably improved an earlier version of the article. CinTurs is financed by National Funds provided by FCT - Foundation for Science and Technology through project UIDB/04020/2020. CEISUC/CIBB is financed by national funds through FCT - Foundation for Science and Technology through project UIDP/04539/2020.
Funding
This study was funded by a grant from Pfizer.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no competing interests to declare that are relevant to the content of this article.
Ethical approval for human subject research
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This study was reviewed and approved by the (Portuguese) National Data Protection Commission (ref. 1737/2015). The anonymity and confidentiality of the participants were preserved.
Informed consent
Informed consent was obtained from all individual participants included in the study. Participants were informed about their freedom for refusal.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ferreira, P.L., Pereira, L.N., Antunes, P. et al. EQ-5D-5L Portuguese population norms. Eur J Health Econ 24, 1411–1420 (2023). https://doi.org/10.1007/s10198-022-01552-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10198-022-01552-9