
Abstract
Infections with carbapenemase-producing Gram-negative bacteria are related to increased morbidity and mortality, yet little is known regarding infections caused by non-beta-lactamase mediated carbapenem-resistant bacteria. Our objective was to identify risk factors for, and the clinical impact of infections caused by carbapenem-resistant carbapenemase-negative Enterobacterales and Pseudomonas aeruginosa. This retrospective matched case-control study was performed at the University Hospital of Basel, Switzerland, in 2016. We focused on other resistance mechanisms by excluding laboratory-confirmed carbapenemase-positive cases. Carbapenem resistance was set as the primary endpoint, and important risk factors were investigated by conditional logistic regression. The clinical impact of carbapenem resistance was estimated using regression models containing the resistance indicator as explanatory factor and adjusting for potential confounders. Seventy-five cases of infections with carbapenem-resistant, carbapenemase-negative bacteria were identified and matched with 75 controls with carbapenem-susceptible infections. The matched data set was well-balanced regarding age, gender, and comorbidity. Duration of prior carbapenem treatment (OR 1.15, [1.01, 1.31]) correlated with resistance to carbapenems. Our study showed that patients with carbapenem-resistant bacteria stayed 1.59 times (CI [0.81, 3.14]) longer in an ICU. The analyzed dataset did not provide evidence for strong clinical implications of resistance to carbapenems or increased mortality. The duration of prior carbapenem treatment seems to be a strong risk factor for the development of carbapenem resistance. The higher risk for a longer ICU stay could be a consequence of a carbapenem resistance. In contrast to carbapenemase-producers, the clinical impact of carbapenamase-negative, carbapenem-resistant strains may be limited. Trial registration: The study design was prospectively approved by the local Ethics Commission on 10.08.2017 (EKNZ BASEC 2017-00222).
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Carbapenems are important beta–lactam antibiotics due to their broad spectrum of action. This allows the treatment against a wide range of antimicrobial resistant bacteria, including leading pathogens of hospital-acquired infections such as extended-spectrum beta-lactamase (ESBL)- (Paterson 2000) or AmpC-producing Enterobacterales (Metsini et al. 2018), and non-fermenting Gram-negative bacteria including Pseudomonas aeruginosa (Lautenbach et al. 2010). Carbapenem resistance has been associated with increased mortality rates, prolonged hospital stays, and higher hospitalization costs (Adams et al. 2020; Correa et al. 2013). Therefore, resistance against carbapenems is critical for treatment and patient management (Ferstl et al. 2017; Schwaber et al. 2008).
Several studies have examined risk factors for the development of carbapenem resistance. They suggest that the previous use of antibiotics and in particular of carbapenems prior to hospital stay, admission to the intensive care unit (ICU), required assistance in activities of daily living, and usage of central catheters favor the acquisition or selection of resistant strains (Correa et al. 2013; Jeon et al. 2008; Schwaber et al. 2008; Wang et al. 2016).
Four mechanisms of carbapenem resistance are recognized: production of carbapenem-hydrolyzing β-lactamases, expression of efflux pumps, mutations that influence penicillin-binding proteins (PBPs), and change of functional porins (Papp-Wallace et al. 2011). Most of the clinical studies focus on plasmid-acquired carbapenemases. Although it has been shown that deletions or single nucleotide polymorphisms cause changes in the aminoacid sequence and subsequent structure of the porin protein (Sanbongi et al. 2009), the clinical aspects of porin loss are not well investigated. The OprD porin protein of P. aeruginosa is strongly linked with carbapenem resistance (Sanbongi et al. 2009; Yoneyama and Nakae 1993). Additional studies further reported the importance of variations in porin expression in Enterobacterales (Doumith et al. 2009; Lavigne et al. 2013). Further mechanisms may evolve subsequently under the ongoing selective pressure induced by the broad use of carbapenems (Li et al. 2012).
The objective of this study was to identify the clinical determinants of carbapenemase-negative, carbapenem-resistant Enterobacterales as well as P. aeruginosa, and to explore the clinical implications of these resistances in a low-endemic setting of carbapenemases.
Methods
Design, setting, and ethics
The University Hospital Basel (USB) in Switzerland is a tertiary care hospital with a capacity of 855 beds and approximately 38,000 admissions per year. In Switzerland, carbapenemases in Enterobacterales are rare on a stable low level and constitute 142 isolates during 2016 in the whole country (Federal Office of Public Health and Federal Food Safety and Veterinary Office 2018). The study design was approved by the local Ethics Commission (EKNZ BASEC 2017-00222).
In this retrospective case-control study, we included as potential cases all hospitalized adult patients at the USB in 2016, who received antimicrobial susceptibility testing for Enterobacterales or P. aeruginosa. The Enterobacterales group included the following species: Citrobacter freundii group, Enterobacter cloacae group, Klebsiella aerogenes, Escherichia coli, Serratia marcescens, and Klebsiella pneumoniae group. Furthermore, species with resistances to the carbapenems ertapenem, imipinem, or meropenem were selected for further analysis. Due to weak activity of ertapenem against P. aeruginosa (Papp-Wallace et al. 2011), the susceptibility testing of P. aeruginosa was performed on imipenem and meropenem. Cases with a pheno- or genotypically confirmed carbapenemase-positive isolate were excluded. Hospitalization below 24 h, insufficient documentation in the chart record, or multiple admissions for a single case were defined as additional exclusion criteria. In case of repeated bacterial isolates from the same patient, the first resistant isolate was taken.
To each of the carbapenem-resistant, carbapenemase-negative cases, a carbapenem-sensitive control was exactly matched according to the following criteria: bacterial species, ward type (medical, surgical, obstetrics and gynecology, and intensive care unit), and isolation source (blood, urine, respiratory material, and superficial swabs or deep tissue biopsies). The prioritized control was replaced with an alternative control in case of multiple selection, insufficient information, or hospitalization below 24 h.
In the primary analysis, the carbapenem resistance was set as the primary endpoint, and the most important risk factors were investigated. The clinical implications were examined in the secondary analysis regarding the endpoints: all-cause mortality during hospital stay (within 30 days after resistance test (RT)), total intensive care unit stay (days), hospital stay duration (days), rehospitalization at USB (yes/no), and duration of antibiotic treatment (days).
Patient data collection
Data for all patients were gathered retrospectively by chart review. This included associated patient data separately for the time frame before and after the isolates were identified. The following information was collected: adapted Charlson comorbidity index (Charlson et al. 1994), transplantations, demographic information, and resistance profile of the isolate to other antibiotics. Previous intake of acetylsalicylic acid or antacids (at admission), previous surgical interventions (3 months prior to the RT), previous hospitalizations (1 month prior to the RT), and foreign body (in situ at the time of the RT) such as urinary catheter were recorded. The following data were gathered separately for the time frame before and after susceptibility testing as well as during the whole period: duration of antibiotic intake split into common antibiotic subgroups (1 month prior to the RT; RT till discharge), and duration of hospitalization and intensive care unit stay. Different variables like within-hospital mortality and rehospitalization at the USB (<1 month after discharge) completed the data base.
The data were recorded in an electronic case report form with the support of the freeware “Epidata” (version 4.2.0.0.) (EpiData Association 2017).
Antibiotic susceptibility testing
We included all bacterial isolates found during routine diagnostics at the ISO-accredited diagnostic microbiology laboratory (Fig. 1). Antimicrobial susceptibility testing was performed according to EUCAST guidelines. Bacterial isolates were identified using MALDI-TOF mass spectrometry (Bruker Microflex, Bremen, Germany) with the mass-spectrum library and the MALDI Biotyper 3 software (OC 3.1, Bruker Daltonics) at standard conditions. Alternatively, we used the biochemical profile from VITEK2 (bioMérieux, Marcy-l’Étoile, France) for identification. Antimicrobial susceptibility profile was generated using the Gram-negative AST card (N242) on the VITEK 2 (bioMérieux) instrument. We used EUCAST recommendations for screening for carbapenemase production (Giske et al. 2013).
For screening purposes, we used specific selective chromogenic culture plates: CARBA-ID for carbapenemases (bioMérieux) and ESBL-ID for ESBL (bioMérieux) (Hinić et al. 2017). Identification of colonies growing on screening plates was performed using MALDI-TOF MS, followed by a phenotypic and/or genotypic confirmation of the corresponding resistance mechanism.
For phenotypic confirmation we used (i) the KPC, MBL, and OXA-48 confirm kit (ROSCO, Taastrup, Denmark) or (ii) for Metallo-Beta-Lactamases also a combined dual E-Test® MBL IP/IPI (bioMérieux) was used. These tests are based on a ratio interpretation by a MIC or inhibition zone, resulting from a combination of the carbapenem antibiotic with and without a carbapenemase inhibitor.
For genotypic confirmation, we used the following tests: (i) Xpert Carba-R (Cepheid, Sunnyvale, California) covering KPC, NDM, VIM, IMP-1, and OXA-48;(ii) eazyplex SuperBug CRE (Amplex, Gars am Inn, Germany) covering KPC, NDM, OXA-48, OXA-181, VIM, and the ESBL genes of the CTX-M-1 and CTX-M-9 group (Hinić et al. 2015) or whole genome sequencing.
Statistics
Matching
Matching was done using R (version 3.3.0) and the MatchIt software package (Daniel et al. 2011; R Core Team 2016). Every carbapenem-resistant case was matched to five non-resistant controls by corresponding bacterial species, ward, and source of bacterial isolation (i.e., material category). Subsequently, a nearest neighbor analysis sorted the matched controls by the date the isolates were taken and prioritized controls that were closer to the date of the corresponding case. As the statistics was performed with one prioritized control per case, the remaining 4 controls were used as alternative options.
Outcomes and analysis
Prior to analysis, we determined an analytical plan following standard statistical procedures at the Clinical Trial Unit. The primary objective of this case-control study was to identify the determinants of non-carbapenemase mediated carbapenem resistance. For an overview, the baseline characteristics were summarized. Median, standardized mean difference (SMD), and standard deviation are shown unless otherwise indicated. When comparing two groups, the SMD measures the difference between the group means of a variable in terms of the average standard deviation of this variable within the two groups (Austin 2011).
Since we were dealing with an exactly matched data set, the primary analysis was based on conditional logistic regression, estimated using the R package survival (version 2.44-1.1) (Pearce 2016). Beforehand, the five potentially most important risk factors for a resistance were selected by the investigators: carbapenem treatment duration before RT (days), hospital stay duration before RT (days), ICU stay duration before RT (days), surgery before RT (yes/no), and Charlson comorbidity index (numeric score). To identify further relevant predictors among the baseline characteristics, we performed an automated variable selection based on Akaike’s information criterion (AIC) using the R package MASS (version 7.3-51.4). Using all patients with completely observed data, we performed a forward variable selection and a backward selection as sensitivity analysis. In addition, we conducted sensitivity analysis using two pragmatic imputation methods.
The average impact of carbapenem resistance on the secondary endpoints was estimated using regression models containing the resistance indicator as explanatory factor and controlling for further potential confounders. For the secondary endpoint death during hospital stay, we used logistic regression models, while the outcome total intensive care unit stay duration was analyzed with a hurdle model (Zeileis 2008). The results for hospital stay duration and duration of antibiotic treatment were obtained using (generalized) linear regression models. For each secondary outcome, we estimated one model controlling for a minimal set of potential confounders identified by the investigators and compared this with a model adjusting for a more comprehensive set of covariates.
Results
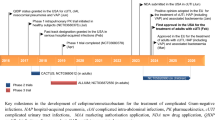
During the study period 3,426 isolates of Enterobacterales and P. aeruginosa were tested for carbapenem susceptibility. Out of this cohort, 90 patients were identified with bacteria carrying one or more resistances to the carbapenems ertapenem, imipinem, or meropenem and selected for further analysis. Four of these 90 cases were tested positive for carbapenemases and subsequently excluded. Reasons for additional exclusions were hospitalization below 24 h, insufficient documentation in the chart record, or multiple admissions for a single case (Fig. 1). Eight controls were replaced due to their multiple selection or insufficient information.

Flow diagram of the matching and exclusion process for the case-control study of carbapenem-resistant Enterobacterales and P. aeruginosa in Switzerland, 2016
We finally included retrospective data of 75 resistant cases matched with 75 controls sensitive to carbapenems. As the analysis could only be performed with completely observed variables, each analysis was performed with a different number of subjects. Depending on the selected potential predictors for each analysis, cases and controls with at least one incomplete variable had to be excluded. The variables were incomplete in case the information in the patient chart did not allow a statement. For example, as the information was taken from in hospital patient charts, no statement could be made about the mortality within 30 days where a patient left the hospital during this period without readmission.
Table S1 of the supplementary material shows the structure of the matching criteria. Forty-three (57.3%) of all 75 cases were tested positive to carbapenem-resistant P. aeruginosa. Moreover, respiratory material was the most common isolation site with 31/75 (41.3%) cases and 30/75 (40%) isolates were detected in patients hospitalized on a medical ward.
Primary analysis: determinants of carbapenem resistance
We performed the primary analysis on the complete 73 cases and 71 controls. The primary analysis is based on those 144 subjects for whom all potential predictors (listed in Table 1) were completely observed. This restriction is necessary because we compared estimated models to identify the most relevant predictors using the AIC here. All the variables for the primary analysis were of general character (age, sex, comorbidity, etc.) or referred to the time frame of the clinical management prior to when the isolates were sampled (treatment with antibiotics, surgical interventions, etc).
Table 1 provides an overview of the analyzed data set. Even though the matching did not explicitly account for age, gender, and comorbidities, the matched data set seems to be well-balanced regarding the variables age (SMD 0.128), gender (SMD 0.093), and Charlson comorbidity index (SMD 0.040). The standardized mean differences of the variables between the group of patients with carbapenem-resistant bacteria and the group with carbapenem-sensitive bacteria are low.
Next, we performed an automated variable selection to identify further relevant variables associated with resistance beside the five pre-selected by the investigators (1st to 5th variable in Table 2). Table 2 shows the odds ratios estimated in the model selected by a forward search. Four additional predictors were selected into the model, which has an improved AIC of 75.61 compared to 87.15 without additional predictors. The duration of carbapenems treatment prior to detecting the resistance appears to be a relevant exposure with an estimated odds ratio of 1.15. This implies that with each day of carbapenems treatment the chances of a resistance to these antibiotics increase by this factor. In addition, we found that resistance to other antibiotics is a strong association (OR 8.33, CI [1.73, 40.13], p-value 0.008), while acetylsalicylic acid seems to be associated with a reduction of resistance to carbapenems. Further, the treatment with cephalosporins before the resistance appears to be linked to a higher risk of carbapenem resistance with an Odds ratio of 1.28.
The performed susceptibility analysis yielded similar results.
Secondary analysis: clinical implications
The secondary objective was to explore the implications of an infection with carbapenem-resistant, carbapenemase-negative bacteria with respect to a number of clinical outcomes. The descriptive analysis of the secondary endpoints contained the initial dataset of 75 cases and 75 controls. Further secondary analyses are based on 128 to 149 subjects, depending on whether the corresponding endpoints and predictors were completely observed.
Table 3 shows the results of the descriptive analysis of the secondary endpoints. Twelve patients from the sensitive cohort died within 30 days after the antibiotic susceptibility testing had been conducted, and seven deaths of resistant cases were reported. The duration of the whole hospitalization stays and in the ICU was longer in the resistant group. With a day average of 8.6 for cases and 4.5 for controls, the total duration of ICU stays almost half.
Regression models containing the resistance indicator as explanatory factor and controlling for further potential confounders were used to analyze mortality rates in detail. Controlling was conducted with a minimal and an extensive set of confounders. Based on the performance on AIC, one approach was selected and presented in Tables 4 and 5.
With an odds ratio of 0.44 (CI [0.14, 1.36]), the models did not show an association of carbapenem resistance and mortality. As shown in Table 4, the time spent in an ICU during the hospitalization appears to be the most important characteristic associated with dying in hospital.
The association between the length of a potential ICU stay and suffering from an infection with carbapenem-resistant bacteria was assessed using a hurdle model. The model indicates that patients with carbapenem-resistant bacteria tend to stay 1.59 times (CI [0.81, 3.14]) longer in an ICU, when admitted. Potential confounders were included, and the corresponding results are listed in Table 5.
Separate analysis was performed with no remarkable result on duration of total hospitalization stay, rehospitalization at USB, and antibiotic treatment. Adjusted linear regression models did not indicate a difference between patients with carbapenem-resistant bacteria and patients with a carbapenem-sensitive infection.
Discussion
Most of the previous published literature focused on resistances due to carbapenemases, but very little data exist on the determinants and implications of other possible resistance mechanisms such as porin loss or efflux pump activity in a wider range of Gram-negative bacteria. Therefore, carbapenemase-positive isolates were excluded in this study. The objective of this study was to identify the clinical determinants of carbapenemase-negative, but carbapenem-resistant Enterobacterales, as well as P. aeruginosa, and to explore the clinical implications of these resistances in a low-endemic setting of carbapenemases. Our analysis shows that the duration of prior carbapenem treatment correlates with resistance to carbapenem. Furthermore, the data indicates that patients with carbapenem-resistant bacteria tend to stay longer in an ICU ward.
With 43 patients suffering from an infection of carbapenem-resistant, carbapenemase-negative P. aeruginosa, more than half of the included cases were caused by this pathogen. This is not surprising, considering that P. aeruginosa is one of the major nosocomial pathogens and has a well-known resistance mechanism due to porin loss (Sanbongi et al. 2009; Yoneyama and Nakae 1993).
Differences concerning comorbidities between the resistant and the sensible cohort could not be shown. A possible explanation might be that the quantification using the Charlson comorbidity index is lacking in completeness and specificity for infection-relevant comorbidities. For instance, several cases with cystic fibrosis could not be taken into full account due to the index being focused more on chronic respiratory diseases like COPD that are common in the average population. As we are dealing with a carbapenem-resistant subgroup with stated higher prevalence for cystic fibrosis, this could confound the index values (Oliver et al. 2000).
Our first question sought to identify determinants of carbapenem resistance in carbapenemase-negative Gram-negative bacteria. Our models indicate nine predictors with variable evidence. In general, it seems that the development of resistances is the result of numerous interfering risk factors. The analysis of these nine predictors implies that the duration of carbapenem treatment is an important risk factor. Another result is the robust correlation of resistance to carbapenems with resistances to other antibiotics (summing up resistances to aminoglycosides and fluoroquinolones). The multi-resistant bacteria as well as the gradual escalation resulting in the use of carbapenems as antibiotics of last resort explain this temporal association. A strong relationship between the intake of different antibiotics and resistance to carbapenems has been reported in various studies (Adams et al. 2020; Jeon et al. 2008; Schwaber et al. 2008). Interestingly, together with carbapenems, the intake of cephalosporins seems to be associated with a resistance to carbapenems. Kwak et al. stated this association before among carbapenem-resistant Klebsiella pneumoniae (Kwak et al. 2005). The exact molecular mechanism was not explored in that study and neither in ours. The increased intake of cephalosporins may correlate with the overexpression of extended-spectrum beta-lactamase (ESBL) or AmpC genes what potentially lead on its own to the resistance of carbapenems or triggered an escalation towards carbapenem treatment (Majewski et al. 2016; Rizi et al. 2023; Wilson and Török 2018). Furthermore, our data suggest the association between the duration of hospitalization in the ICU and the development of resistant species. This seems to be consistent with other research (Schwaber et al. 2008).
We found that the intake of aspirin may be associated with decreased risk of resistance to carbapenems. In discordance with this suggestion, previous investigations (Bandara et al. 2016; Ochs et al. 1999; Zimmermann and Curtis 2018) have indicated that the intake of acetylsalicylic acid is leading to more resistances. Our data could not corroborate the findings of an in vitro study that showed the reduction of OprD porin in P. aeruginosa outer membranes and increase of resistance to carbapenems due to acetyl salicylate (Ochs et al. 1999). In addition, another paper investigated the outer membrane proteomic profile of a P. aeruginosa isolate and found that some porins were downregulated in presence of salicylic acid in vitro (Bandara et al. 2016). It remains unclear if this in vitro observation is clinically meaningful. In our study, it could be that the intake of acetylsalicylic acid is associated indirectly with a lower exposure to carbapenem antibiotics. Further studies are needed to explore the potential impact of co-medication on antibiotic resistance.
Next, we examined the clinical impact of carbapenem resistance. The analyzed dataset does not provide evidence for strong clinical implications of a resistance to carbapenems. The results of the secondary analysis propose that patients suffering from infection with carbapenem-resistant bacteria have longer ICU stays. As a stay in the ICU increases hospitalization costs dramatically, this may confirm the association of carbapenem resistance and higher hospitalization costs in earlier research (Adams et al. 2020). The results of the descriptive analysis regarding the hospital stay duration could not be confirmed with models considering multiplicative effects. In this case, we could not support evidence from previous observations (Adams et al. 2020).
Evidence for an increased mortality could not be demonstrated. This may be explained by a previous study which suggests poorer outcomes for carbapenem resistance due to carbapenemases compared with resistance of non-carbapenemase-producing Enterobacterales (Tamma et al. 2017).
However, these results need to be interpreted with caution. Our study has the following limitations: retrospective data with absence of further follow up after the stay in the hospital of tertiary care and limited number of patients. The limited number of patients from a single center in Switzerland and the exclusion of carbapenemase-positive cases may lead to reduced generalizability, especially in other endemic settings (European Centre for Disease Prevention and Control 2018; Federal Office of Public Health and Federal Food Safety and Veterinary Office 2018). We cannot rule out the possibility of confounding due to unmeasured variables, e.g., other interventions like ERCP. Also, we could not perform detailed molecular analysis such as transcriptomics to fully understand the reason for the carbapenem resistance, e.g., overexpression of ESBL or AmpC genes. Nevertheless, we focus in detail on an important group of microbiologically and clinically relevant bacterial strains with carbapenem resistance in absence of carbapenemases.
In conclusion, the duration of prior carbapenem treatment seems to be a strong risk factor. Furthermore, the higher risk for a longer ICU stay could be a consequence of a carbapenem resistance. Considerably more work, especially with larger cohorts, will be needed to further corroborate risk factors for the development of resistances of non-carbapenemase-producing gram-negative bacteria as well as their clinical implications.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Adams DJ, Susi A, Nylund CM (2020) Clinical characteristics, risk factors, and outcomes of patients hospitalized in the US military health system with carbapenem-resistant Enterobacteriaceae infection. Am J Infect Control 48(6):644–649. https://doi.org/10.1016/j.ajic.2019.10.006
Austin PC (2011) An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav Res 46(3):399–424. https://doi.org/10.1080/00273171.2011.568786
Bandara M, Sankaridurg P, Zhu H, Hume E, Willcox M (2016) Effect of salicylic acid on the membrane proteome and virulence of pseudomonas aeruginosa. Invest Ophthalmol Vis Sci 57(3):1213–1220. https://doi.org/10.1167/iovs.15-18990
Charlson M, Szatrowski TP, Peterson J, Gold J (1994) Validation of a combined comorbidity index. J Clin Epidemiol 47(11):1245–1251
Correa L, Martino MDV, Siqueira I, Pasternak J, Gales AC, Silva CV, Camargo TZS, Scherer PF, Marra AR (2013) A hospital-based matched case-control study to identify clinical outcome and risk factors associated with carbapenem-resistant Klebsiella pneumoniae infection. BMC Infect Dis 13:80–80. https://doi.org/10.1186/1471-2334-13-80
Daniel E, Ho KI, King G, Stuart EA (2011) MatchIt: nonparametric preprocessing for parametric causal inference. J Stat Softw 42:8
Doumith M, Ellington MJ, Livermore DM, Woodford N (2009) Molecular mechanisms disrupting porin expression in ertapenem-resistant Klebsiella and Enterobacter spp. clinical isolates from the UK. J Antimicrob Chemother 63(4):659–667. https://doi.org/10.1093/jac/dkp029
EpiData Association (2017) EpiData Software, 4.2.0.0 edn, Denmark
European Centre for Disease Prevention and Control (2018) Surveillance of antimicrobial resistance in Europe – annual report of the European antimicrobial resistance surveillance network (EARS-Net) 2017. ECDC, Stockholm
Federal Office of Public Health and Federal Food Safety and Veterinary Office (2018) Swiss antibiotic resistance report 2018. Usage of antibiotics and occurrence of antibiotic resistance in bacteria from humans and animals in Switzerland. November 2018. FOPH publication number: 2018-OEG-87
Ferstl PG, Filmann N, Brandt C, Zeuzem S, Hogardt M, Kempf VAJ, Muller M, Waidmann O, Reinheimer C (2017) The impact of carbapenem resistance on clinical deterioration and mortality in patients with liver disease. Liver Int 37(10):1488–1496. https://doi.org/10.1111/liv.13438
Giske GC, Martinez-Martinez L, Cantón R, Stefani S, Skov R, Glupczynski Y, Nordmann P, Wootton M, Miriagou V, Simonsen GS, Zemlickova H, Cohen-Stuart J, Gniadkowski M (2013) EUCAST guidelines for detection of resistance mechanisms and specific resistances of clinical and/or epidemiological importance. European Committee on Antimicrobial Susceptibility Testing PUblisher. https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Resistance_mechanisms/EUCAST_detection_of_resistance_mechanisms_v1.0_20131211.pdf Accessed 4 September 2022
Hinić V, Amrein I, Stammler S, Heckendorn J, Meinel D, Frei R, Egli A (2017) Comparison of two rapid biochemical tests and four chromogenic selective media for detection of carbapenemase-producing Gram-negative bacteria. J Microbiol Methods 135:66–68. https://doi.org/10.1016/j.mimet.2017.01.012
Hinić V, Ziegler J, Straub C, Goldenberger D, Frei R (2015) Extended-spectrum β-lactamase (ESBL) detection directly from urine samples with the rapid isothermal amplification-based eazyplex® SuperBug CRE assay: proof of concept. J Microbiol Methods 119:203–205. https://doi.org/10.1016/j.mimet.2015.10.015
Jeon MH, Choi SH, Kwak YG, Chung JW, Lee SO, Jeong JY, Woo JH, Kim YS (2008) Risk factors for the acquisition of carbapenem-resistant Escherichia coli among hospitalized patients. Diagn Microbiol Infect Dis 62(4):402–406. https://doi.org/10.1016/j.diagmicrobio.2008.08.014
Kwak YG, Choi SH, Choo EJ, Chung JW, Jeong JY, Kim NJ, Woo JH, Ryu J, Kim YS (2005) Risk factors for the acquisition of carbapenem-resistant Klebsiella pneumoniae among hospitalized patients. Microb Drug Resist 11(2):165–169. https://doi.org/10.1089/mdr.2005.11.165
Lautenbach E, Synnestvedt M, Weiner MG, Bilker WB, Vo L, Schein J, Kim M (2010) Imipenem resistance in Pseudomonas aeruginosa: emergence, epidemiology, and impact on clinical and economic outcomes. Infect Control Hosp Epidemiol 31(1):47–53. https://doi.org/10.1086/649021
Lavigne JP, Sotto A, Nicolas-Chanoine MH, Bouziges N, Pages JM, Davin-Regli A (2013) An adaptive response of Enterobacter aerogenes to imipenem: regulation of porin balance in clinical isolates. Int J Antimicrob Agents 41(2):130–136. https://doi.org/10.1016/j.ijantimicag.2012.10.010
Li H, Luo YF, Williams BJ, Blackwell TS, Xie CM (2012) Structure and function of OprD protein in Pseudomonas aeruginosa: from antibiotic resistance to novel therapies. Int J Med Microbiol 302(2):63–68. https://doi.org/10.1016/j.ijmm.2011.10.001
Majewski P, Wieczorek P, Ojdana D, Sieńko A, Kowalczuk O, Sacha P, Nikliński J, Tryniszewska E (2016) Altered outer membrane transcriptome balance with AmpC overexpression in carbapenem-resistant Enterobacter cloacae. Front Microbiol 7:2054. https://doi.org/10.3389/fmicb.2016.02054
Metsini A, Vazquez M, Sommerstein R, Marschall J, Voide C, Troillet N, Gardiol C, Pittet D, Zingg W, The Swissnoso N (2018) Point prevalence of healthcare-associated infections and antibiotic use in three large Swiss acute-care hospitals. Swiss Med Wkly 148:w14617. https://doi.org/10.4414/smw.2018.14617
Ochs MM, McCusker MP, Bains M, Hancock RE (1999) Negative regulation of the Pseudomonas aeruginosa outer membrane porin OprD selective for imipenem and basic amino acids. Antimicrob Agents Chemother 43(5):1085–1090. https://doi.org/10.1128/aac.43.5.1085
Oliver A, Canton R, Campo P, Baquero F, Blazquez J (2000) High frequency of hypermutable Pseudomonas aeruginosa in cystic fibrosis lung infection. Science 288(5469):1251–1254. https://doi.org/10.1126/science.288.5469.1251
Papp-Wallace KM, Endimiani A, Taracila MA, Bonomo RA (2011) Carbapenems: past, present, and future. Antimicrob Agents Chemother 55(11):4943–4960. https://doi.org/10.1128/aac.00296-11
Paterson DL (2000) Recommendation for treatment of severe infections caused by Enterobacteriaceae producing extended-spectrum beta-lactamases (ESBLs). Clin Microbiol Infect 6(9):460–463
Pearce N (2016) Analysis of matched case-control studies. BMJ 352:i969. https://doi.org/10.1136/bmj.i969
R Core Team (2016) R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria
Rizi KS, Aryan E, Youssefi M, Ghazvini K, Meshkat Z, Amini Y, Safdari H, Derakhshan M, Farsiani H (2023) Characterization of carbapenem-resistant Escherichia coli and Klebsiella: a role for AmpC-producing isolates. Future Microbiol 18:215–223. https://doi.org/10.2217/fmb-2021-0211
Sanbongi Y, Shimizu A, Suzuki T, Nagaso H, Ida T, Maebashi K, Gotoh N (2009) Classification of OprD sequence and correlation with antimicrobial activity of carbapenem agents in Pseudomonas aeruginosa clinical isolates collected in Japan. Microbiol Immunol 53(7):361–367. https://doi.org/10.1111/j.1348-0421.2009.00137.x
Schwaber MJ, Klarfeld-Lidji S, Navon-Venezia S, Schwartz D, Leavitt A, Carmeli Y (2008) Predictors of carbapenem-resistant Klebsiella pneumoniae acquisition among hospitalized adults and effect of acquisition on mortality. Antimicrob Agents Chemother 52(3):1028–1033. https://doi.org/10.1128/aac.01020-07
Tamma PD, Goodman KE, Harris AD, Tekle T, Roberts A, Taiwo A, Simner PJ (2017) Comparing the outcomes of patients with carbapenemase-producing and non-carbapenemase-producing carbapenem-resistant Enterobacteriaceae Bacteremia. Clin Infect Dis 64(3):257–264. https://doi.org/10.1093/cid/ciw741
Wang Q, Zhang Y, Yao X, Xian H, Liu Y, Li H, Chen H, Wang X, Wang R, Zhao C, Cao B, Wang H (2016) Risk factors and clinical outcomes for carbapenem-resistant Enterobacteriaceae nosocomial infections. Eur J Clin Microbiol Infect Dis 35(10):1679–1689. https://doi.org/10.1007/s10096-016-2710-0
Wilson H, Török ME (2018) Extended-spectrum β-lactamase-producing and carbapenemase-producing Enterobacteriaceae. Microb Genom 4(7). https://doi.org/10.1099/mgen.0.000197
Yoneyama H, Nakae T (1993) Mechanism of efficient elimination of protein D2 in outer membrane of imipenem-resistant Pseudomonas aeruginosa. Antimicrob Agents Chemother 37(11):2385–2390. https://doi.org/10.1128/aac.37.11.2385
Zeileis A (2008) Applied Econometrics with R. Springer-Verlag, New York
Zimmermann P, Curtis N (2018) The effect of aspirin on antibiotic susceptibility. Expert Opin Ther Targets 22(11):967–972. https://doi.org/10.1080/14728222.2018.1527314
Funding
Open access funding provided by University of Zurich
Author information
Authors and Affiliations
Contributions
⚬ Marius Müller: Design of the work. Data collection and interpretation. Drafting the article. Final approval of the version to be published.
⚬ Adrian Egli: Design of the work. Data interpretation. Drafting the “Antibiotic susceptibility testing” section. Critical revision of the article. Final approval of the version to be published.
⚬ Andrea Wiencierz: Data analysis. Critical revision of the article. Final approval of the version to be published.
⚬ Christian Gehringer: Matching process. Critical revision of the article. Final approval of the version to be published.
⚬ Sarah Tschudin: Design of the work. Critical revision of the article. Final approval of the version to be published.
⚬ Veronika Muigg: Critical revision of the article. Final approval of the version to be published.
⚬ Martin Siegemund: Critical revision of the article. Final approval of the version to be published.
⚬ Stefano Bassetti: Critical revision of the article. Final approval of the version to be published.
⚬ Vladimira Hinic: Critical revision of the article. Final approval of the version to be published.
Corresponding author
Ethics declarations
Ethics approval
The study was carried out in accordance with relevant national guidelines and regulations of swiss ethics and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study design was approved by the local Ethics Commission “Ethikkommission Nordwest- und Zentralschweiz” (EKNZ BASEC 2017-00222). As we were dealing with anonymized retrospective data, the EKNZ waived the need for patient consent for this study.
Consent to participate
No individual data was used in this study.
Consent for publication
No individual data was used in this study.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Müller, M., Wiencierz, A., Gehringer, C. et al. Factors associated with non-carbapenemase mediated carbapenem resistance of Gram-negative bacteria: a retrospective case-control study. Int Microbiol 27, 597–606 (2024). https://doi.org/10.1007/s10123-023-00405-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10123-023-00405-6