
Abstract
Next-generation sequencing-based microbiological analysis is a complex way to profile vaginal microbiome samples since each step affects the results gained. Methodologies for sample collection lack golden standards. We compared Puritan DNA/RNA swab (PS) and Copan FLOQ swab (CS) and provided consistent and reliable microbiome profiles analyzed by 16S rRNA gene sequencing. We collected two consecutive vaginal samples utilizing PS with room temperature storing and CS with instant freezing from 26 women. Variable region 4 of bacterial 16S rRNA gene was amplified with single PCR by custom-designed dual-indexed primers and sequenced with Illumina MiSeq system. Read quality control, operational taxonomic unit tables, and alpha and beta diversities analysis were performed, and community richness, diversity, and evenness were evaluated and compared between the two samplings and tests. Nineteen sample pairs produced detectable, intact DNA during the extraction protocol and/or further microbial profiles. Alpha bacterial diversity indices were independent on the collection protocol. No significant statistical differences were found in the measured beta diversity metrics between the collection methods. Of the women, 43% had Lactobacillus-dominated vaginal microbiome profile despite of collection method. Previously reported important vaginal microbiome phyla Actinobacteria, Bacteroidetes, Firmicutes, Fusobacteria, and Proteobacteria were present in the sample set although their relative abundances varied among individuals. PS and CS enable constant vaginal microbiota sampling. The PS method with no need for instant freezing is suitable for on-site collections at clinics. Furthermore, it seems to be possible to take two samples instead of one with constant microbiological results.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Background
Vaginal microbiota plays a crucial role in women’s reproductive and sexual health. In the vagina, there is an ingeniously orchestrated communication between the microbes and the host providing vital defense for the host [1,2,3,4,5]. Enormous inter-individual variability of vaginal microbiota arises from various intrinsic and external factors such as genetics, age, diet, medications, hygiene level, and habits [1, 5]. Vaginal microbial profiles of low overall microbial diversity, dominated by certain lactobacilli species such as Lactobacillus crispatus, are currently considered as an example of a healthy vaginal microbiota [1, 2, 5].
Lactobacilli protect women from pathogenic microbes. The development of imbalanced microbiota composition leads to a pathological condition called dysbiosis, a state which has been linked to various disorders and diseases typical for the urogenital tract [6,7,8,9,10]. For example, anaerobic bacteria such as Gardnerella, Atopobium, and Prevotella spp. are shown to dominate microbiota in bacterial vaginosis and increase the risk of vaginal and urogenital infections as well as various sexually transmitted infections (STI) [9,10,11,12,13]. Recent accumulating evidence has linked unhealthy, unbalanced vaginal microbiota even to poor perinatal outcomes such as miscarriage and preterm birth, and also to severe STIs and even increased risk of cervical cancer [8, 14,15,16].
Conventionally, vaginal microbiota has been analyzed by light microscope with direct staining of pap smear or by traditional cultivation methods. Today, next-generation sequencing (NGS) is the method of choice for analyzing clinical human microbiota samples [1, 10, 17, 18]. Thus, the current era of microbiological research is characterized by its reliance on large data sets of nucleotide sequences and bioinformatics [17, 18]. NGS-based molecular analysis methods have increased our knowledge of the detailed vaginal microbial community composition and have provided a broader view of the microbial factors that influence the health of this rather complex vaginal ecosystem [1, 10]. Utilization of NGS as a tool in clinical diagnostics and treatment is currently under heady investigation [10, 18,19,20].
However, the NGS-based analysis is still quite a challenging and complex way to profile human microbiota samples since each step from sample collection to bioinformatics and final statistics affect the final results [17,18,19,20,21]. Further, this research field still lacks the so-called golden standards and the variety of utilized methods for example in sample collection and DNA extraction combined with diverse reporting practices make replication of studies and assessing their quality challenging [17, 22,23,24]. Thus, it is of outmost importance to enhance and optimize the sampling and NGS analysis procedures. These optimized procedures will improve the diagnostics, treatment, and prevention of dysbiosis and infections affecting women’s health [18, 24].
The goal of this study was to compare two vaginal microbiota sampling techniques, namely Puritan DNA/RNA swab (PS) and Copan FLOQ swab (CS), and their possible effect on the subsequent NGS analysis. First, our goal was to study a possibility of taking two consecutive samples instead of one without risking the microbiological results. The second goal was to compare two preserving methods (shield fluid reagent and dry ice) of the samples during transportation to the laboratory. The gain of several samples instead of one and the ability to work without ice and cold chain in the clinical setting would greatly benefit microbiota studies.
Material and methods
This study is a pilot project of the EMMI study (vaginal and oral microbiota study). EMMI study is conducted at the Departments of Gynecology and Obstetrics and Dermatology of the Turku University Hospital and Institute of Dentistry, University of Turku, Turku, Finland. EMMI study has been reviewed by the Ethics Committee of the Hospital District of Southwest Finland (nro 97/1801/2016).
This pilot project of the EMMI study includes a population of non-pregnant women (n = 26, mean 39.1 years, age range 21–68). These women were referred to the Department of Gynecology and Obstetrics, Turku University Hospital because of an abnormal finding in a pap smear test for further examination by colposcopy. Written, informed consent was obtained from each of the volunteers prior to the sample collection. Further, they filled a questionnaire of their demographic characteristics.
Vaginal sampling and DNA extraction
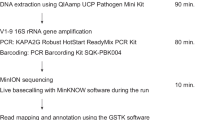
Vaginal study samples were collected on-site, at the beginning of the clinical visit prior to any other investigations and procedures by a specialist in gynecology. Two consecutive swabs were collected and preserved in different sampling tubes namely the Puritan shield fluid tube (PS) and Copan FLOQ tube (CS) from each individual. The sampling flow chart representing the two collection tubes is presented in Fig. 1. Samples were transferred after the collection to the laboratory of Microbiome Biobank, Turku, Finland. PS samples were stored at room temperature and CS at − 80 °C until the DNA extraction, which was made within two weeks according to the manufacturer’s protocol.

Vaginal sample collection and wet lab workflow. Consecutive two samples were taken from the identical vaginal site. Firstly, sterile Puritan DNA/RNA swab (Puritan Medical products, Guilford, ME, USA) was rotated in vagina to collect discharge and placed in a 2-mL shield fluid collection tube (Zymo Research, Irvine, Canada). The tube was kept at room temperature. Secondly, a Copan FLOQ swab (CopanDiagnostics, Murrieta, CA, USA) was rotated in the vagina and transferred immediately on dry ice. Samples were transferred after the collection point to the laboratory of Microbiome Biobank, Turku, Finland. Puritan Shield fluid samples were stored at room temperature and Copan FLOQ swabs at − 80 °C until the DNA extraction
Bacterial DNA was extracted with Hain Viral N/A Extraction Kit and GenoXtract machine (Hain Lifescience GmbH, Nehren, Germany) from the 200 μl aliquot of PS. The biological content collected by CS was dissolved in 200 μl of Puritan Shield fluid prior to the extraction. DNA concentrations were measured with Qubit dsDNA HS Assay Kit and Qubit 2.0 fluorometer (Life Technologies, Carlsbad, USA). Extracted DNAs were stored at − 80 °C prior to the NGS approach.
Next-generation sequencing analysis
Nineteen of the original 26 sample pairs produced detectable DNA and/or microbial profiles with sequencing. Variable region 4 (V4) of bacterial 16S rRNA gene was amplified with single PCR by custom-designed dual-indexed primers and sequenced with Illumina MiSeq (Illumina, San Diego, California, USA) system as previously described [25]. Briefly, the KAPA HiFi PCR kit (KAPA Biosystems, Massachusetts, USA) with in-house generated primers was utilized in amplification. Forward and reverse primer sequences were 5′-AATGATACGGCGACCACCGAGATCTACAC-i5-TATGGTAATT-GT-GTGCCAGCMGCCGCGGTAA-3′ and 5′-CAAGCAGAAGACGGCATACGAGAT -i7- AGTCAGTCAG-GC-GGACTACHVGGGTWTCTAAT-3′, respectively, where i5 and i7 represent the sample-specific index sequences.
The PCR products were purified with Agencourt AMPure XPMagnetic beads (BeckmanCoulter, Inc., USA) on DynaMag™-96 magnetic plate (Life Technologies, USA). The PCR product length and DNA integrity were checked with TapeStation (Agilent Technologies Inc., USA), and the final DNA concentrations of the purified products were measured with Qubit 2.0 dsDNA HS assay kit (Life Technologies, USA). The products were then mixed in equal concentrations to generate a 4 nM library pool, which was denatured, diluted into a final concentration of 4 pM, and spiked with 25% denatured PhiX control (Illumina, USA) for sequencing. Sequencing was done with 2 × 250 bp paired-end reads on the MiSeq system (Illumina, USA), using MiSeq v3 reagent kit (Illumina, USA). Raw reads across the samples sequenced with the Illumina MiSeq 250 bp paired-end sequencing were used as input for the data analysis.
Data processing and statistical methods
Read quality control, operational taxonomic unit (OTU) tables, alpha, and beta diversities analysis were performed with CLC Genomics Workbench v. 20 Microbial Genomics module (QIAGEN Digital Insights, Aarhus, Denmark). Raw sequences were assigned to operational taxonomic units (OTU) according to the CLC Microbial genomics module workflow. Quality and ambiguous trims were performed with default settings, and the minimum number of nucleotides was set to 150. The minimum rarefraction level was 5264. SILVA 16S v132 preclustered at 97% identity was used as the reference database [26, 27]. Alpha diversity measures, namely Chao1 index, Shannon index, and number of observed species were calculated to evaluate community richness, diversity, and evenness. The beta diversity measure, Bray–Curtis dissimilarity, was calculated and the PERMANOVA test with 99,999 permutations was used to calculate the p-values.
Kruskal–Wallis H test was used to assess whether the values depend on the group they belong to in Chao1 and Shannon indices.
Results
The effect of the sample collection method on the DNA yields
There was a significant difference in the DNA gain (nanogram/microliter of vaginal sample) between the two evaluated sampling methods, CS and PS: 3.2 ± 4.0 vs. 15.6 ± 14.6 ng/µl (p < 0.001). Four CS samples contained too low DNA gain or quality and were excluded from the MiSeq analysis. Thus, the DNA quantity when using dry CS and immediate freezing was lower in all the collected sample pairs than in PS.
Overall sequencing output and microbial profiles
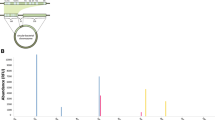
Three samples did not provide quality results and were excluded. A total of 18, 327, 359 reads from the Illumina MiSeq platform of the 19 samples were trimmed for further analyses. All sequenced samples produced detectable microbial profiles. However, there was some variation between the sequence counts between the different individuals (Fig. 2). Despite the collection method, all gained 16S rRNA taxonomical profiles represented bacterial taxa that are characteristic of vaginal microbiota (Fig. 2).

Stacked barplots representing relative abundance of bacteria on consecutive vaginal microbiome samples in phylum (upper chart) and genus level (lower chart). All the gained 16S rRNA taxonomical profiles represented bacterial taxa that are characteristic of vaginal microbiota despite the collection method
Vaginal microbiota
Members of all the previously reported important phyla Actinobacteria, Bacteroidetes, Firmicutes, Fusobacteria, and Proteobacteria, were present in the sample sets although their relative abundances varied markedly from person to person (Fig. 2 upper chart). Altogether, 8/19 (42%) of the women had Lactobacillus-dominated vaginal microbiome despite of collection method (Fig. 2 lower chart).
Diversity indices
The overall microbial profiles of vaginal samples were further described by utilizing various diversity measures. Observed alpha bacterial diversity indices, represented as Shannon index, Chao1 index, and the observed number of species, were not dependent on the collection protocol (P > 0.05 for all, Fig. 3A-C). In addition, no significant statistical differences were found in any of the measured β-diversity metrics between the collection methods (p > 0.05 for all, Fig. 4A, B) indicating that both CS and PS are acceptable means of sampling.

Observed alpha bacterial diversity indices, represented as A Shannon index (p = 0.7), B Chao1 index (p = 0.8), and C the observed number of species (p = 0.6), was not dependent on the collection protocol

Neither A weighted UniFrac nor B Bray Curtis β-diversity metrices were significantly different between the collection methods (p > 0.05, for both) indicating that both CS and PS are acceptable means of sampling. Blue = CS, red = PS
Discussion
Microbial diseases and disorders affecting female genital health have become an increased epidemiological and clinical challenge and also have a social and psychological influence. Vaginal microbial composition is a potential future target for clinical diagnostics [10, 20, 24, 28,29,30]. However, the development of any diagnostic test in clinical microbiology requires straightforward and trustworthy sample-collection methods.
In the present study, DNA gain was different between the two evaluated sampling methods as reported also in earlier methodological studies [23]. This may reflect issues with the sampling method such as the structure of the swab. However, since the gain reduced with the latter utilized method, the possibility is that the first sampling had a better yield simply because it was performed first. However, this reduced gain was able to provide similar results on the microbiota. Furthermore, both sample collection methods produced 16S rRNA taxonomical profiles that were similarly distinguishable between Lactobacillus-dominant versus mixed microbiota. Bacterial diversity was not dependent on the collection protocol. Therefore, it seems safe to collect two samples at the same visit from the vaginal site with no influence on microbiota results. The gain of two vaginal samples instead of one will increase the possibilities for microbiota research.
Based on molecular studies, there are an estimated 1012 − 1013 fungi compared to 1013 − 1014 bacteria in the human microbiota, across the gastrointestinal tract, oral cavity, vaginal mucosa, and skin [31]. According to previous studies as mentioned above, in cohort representative of a normal healthy female population, the vaginal microbiome has shown five subgroups where four of the groups have contained lactobacillus dominated and one group non-lactobacillus dominated microbiome [1, 10, 23, 32, 33]. In our study, 42% of the women had Lactobacillus-dominated vaginal microbiome. Our primer set included also V4 level primers [25] and thus, we were able to show the presence of Gardnerella spp. (Fig. 3). The presence of Gardnerella vaginalis and an assortment of other, typically anaerobic species is indicative of dysbiosis and prevails, e.g., in bacterial vaginosis [9, 34, 35]. However, this was expected since our cohort consisted of women referred to colposcopy due to an abnormal pap smear finding, thus not representing a normal population. An abnormal pap smear is linked with human papillomavirus (HPV) positivity and further dysbiosis [8].
As a strength of the current study, with V4-targeted 16S amplicon sequencing analysis, it is possible to get an overview of the bacterial community composition of a clinical sample and further, in clinical studies identify profile-level differences between the groups and variation within groups [18, 24]. Research work is time and money consuming. In the current study, we have simplified the sampling method and succeeded in taking two consecutive samples and working on room-temperature material in the clinical setting. This increases the gain of research material with fewer appointments for sampling and the lack of ice and cold chain opens new and more distant possibilities for research. However, our study also has several limitations. This study was designed only to methodologically compare the microbial results of two consecutive vaginal samplings focusing on two different sampling methods. In addition, the design of this pilot study with a small number of participants did not allow randomization due to clinical practice and only one researcher.
As a conclusion, we demonstrate that it was safe to collect two consecutive samples from the same vaginal site with minimal influence on microbiota results. PS and CS enabled constant vaginal microbiota sampling without differences between the two sampling methods. In addition, shield fluid reagent allows the transportation of microbiota samples at room temperature as it preserves the integrity of genetic material present in samples at ambient temperatures enabling it to be used in NGS analysis. A redundant cold chain simplifies collection and research in more distant locations from research utilities.
Data availability
The datasets generated during and analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request.
References
France M, Alizadeh M, Brown S, Ma B, Ravel J (2022) Towards a deeper understanding of the vaginal microbiota. Nat Microbiol 7(3):367–378. https://doi.org/10.1038/s41564-022-01083-2
Dabee S, Passmore JS, Heffron R, Jaspan HB (2021) The complex link between the female genital microbiota, genital infections, and inflammation. Infect Immun 89:e00487-e520. https://doi.org/10.1128/IAI.00487-20
Kalia N, Singh J, Kaur M (2020) Microbiota in vaginal health and pathogenesis of recurrent vulvovaginal infections: a critical review. Ann Clin Microbiol Antimicrob 19:5. https://doi.org/10.1186/s12941-020-0347-4
Chopra C, Bhushan I, Mehta M, Koushal T, Gupta A, Sharma S et al (2022) Vaginal microbiome: considerations for reproductive health. Fut Microbiol 17(18):1501–1513. https://doi.org/10.2217/fmb-2022-0112
Lehtoranta L, Ala-Jaakkola R, Laitila A, Maukonen J (2022) Healthy vaginal microbiota and influence of probiotics across the female life span. Front Microbiol 787. https://doi.org/10.3389/fmicb.2022.819958
Hong X, Ma J, Yin J, Fang S, Geng J, Zhao H et al (2020) The association between vaginal microbiota and female infertility: a systematic review and meta-analysis. Arch Gynecol Obstet 302:569–578. https://doi.org/10.1007/s00404-020-05675-3
Tamarelle J, Thiébaut ACM, de Barbeyrac B, Bébéar C, Ravel J, Delarocque-Astagneau E (2019) The vaginal microbiota and its association with human papillomavirus, Chlamydia trachomatis, Neisseria gonorrhoeae and Mycoplasma genitalium infections: a systematic review and meta-analysis. Clin Microbiol Infect 25:35–47. https://doi.org/10.1016/j.cmi.2018.04.019
Kyrgiou M, Mitra A, Moscicki AB (2017) Does the vaginal microbiota play a role in the development of cervical cancer? Transl Res 179:168–182. https://doi.org/10.1016/j.trsl.2016.07.004
Lev-Sagie A, De Seta F, Verstraelen H, Ventolini G, Lonnee-Hoffmann R, Vieira-Baptista P (2022) The vaginal microbiome: II. Vaginal dysbiotic conditions. J Low Genit Tract Dis 26(1):79–84. https://doi.org/10.1097/LGT.0000000000000644
Günther V, Allahqoli L, Watrowski R, Maass N, Ackermann J, von Otte S, Alkatout I (2022) Vaginal microbiome in reproductive medicine. Diagnostics 12(8):1948. https://doi.org/10.3390/diagnostics12081948
Anahtar MN, Gootenberg DB, Mitchell CM, Kwon DS (2018) Cervicovaginal microbiota and reproductive health: the virtue of simplicity. Cell Host Microbe 23:159–168. https://doi.org/10.1016/j.chom.2018.01.013
Ravel J, Brotman RM (2016) Translating the vaginal microbiome: gaps and challenges. Genome Med 8:35. https://doi.org/10.1186/s13073-016-0291-2
Dols JA, Molenaar D, van der Helm JJ, Caspers MP, de Kat A-B, Schuren FH et al (2016) Molecular assessment of bacterial vaginosis by Lactobacillus abundance and species diversity. BMC Infect Dis 16:180. https://doi.org/10.1186/s12879-016-1513-3
Tuddenham S, Ravel J, Marrazzo JM (2021) Protection and risk: male and female genital microbiota and sexually transmitted infections. J Infect Dis 223:S222–S235. https://doi.org/10.1093/infdis/jiaa762
Al-Memar M, Bobdiwala S, Fourie H, Mannino R, Lee YS, Smith A et al (2020) The association between vaginal bacterial composition and miscarriage: a nested case-control study. BJOG 127:264–274. https://doi.org/10.1111/1471-0528.15972
Mitra A, MacIntyre DA, Lee YS, Smith A, Marchesi JR, Lehne B et al (2015) Cervical intraepithelial neoplasia disease progression is associated with increased vaginal microbiome diversity. Sci Rep 5:16865. https://doi.org/10.1038/srep16865
Knight R, Vrbanac A, Taylor BC, Aksenov A, Callewaert C, Debelius J et al (2018) Best practices for analysing microbiomes. Nat Rev Microbiol 16:410–422. https://doi.org/10.1038/s41579-018-0029-9
Verstraelen H, Vieira-Baptista P, De Seta F, Ventolini G, Lonnee-Hoffmann R, Lev-Sagie A (2022) The vaginal microbiome: I. Research development, lexicon, defining “Normal” and the dynamics throughout women’s lives. J Low Genit Tract Dis 26(1):73–78. https://doi.org/10.1097/LGT.0000000000000643
Singer M, Koedooder R, Bos MP, Poort L, Schoenmakers S, Savelkoul PHM et al (2021) The profiling of microbiota in vaginal swab samples using 16S rRNA gene sequencing and IS-pro analysis. BMC Microbiol 21:100. https://doi.org/10.1186/s12866-021-02149-7
Campisciano G, Zanotta N, Petix V, Giangreco M, Ricci G, Maso G et al (2021) Vaginal dysbiosis and partial bacterial vaginosis: the interpretation of the “Grey Zones” of clinical practice. Diagnostics (Basel) 11:191. https://doi.org/10.3390/diagnostics11020191
Marotz C, Cavagnero KJ, Song SJ, McDonald D, Wandro S, Humphrey G et al (2021) Evaluation of the effect of storage methods on fecal, saliva, and skin microbiome composition. mSystems 6:e01329-20. https://doi.org/10.1128/mSystems.01329-20
Nearing JT, Comeau AM, Langille MG (2021) Identifying biases and their potential solutions in human microbiome studies. Microbiome 9:113. https://doi.org/10.1186/s40168-021-01059-0
Virtanen S, Kalliala I, Nieminen P, Salonen A (2017) Comparative analysis of vaginal microbiota sampling using 16S rRNA gene analysis. PLoS ONE 12:e0181477. https://doi.org/10.1371/journal.pone.0181477
Sharma M, Chopra C, Mehta M, Sharma V, Mallubhotla S, Sistla S et al (2021) An insight into vaginal microbiome techniques. Life (Basel) 11(11):1229. https://doi.org/10.3390/life11111229
Rintala A, Riikonen I, Toivonen A, Pietilä S, Munukka E, Pursiheimo JP et al (2018) Early fecal microbiota composition in children who later develop celiac disease and associated autoimmunity. Scand J Gastroenterol 53:403–409. https://doi.org/10.1080/00365521.2018.1444788
Quast C, Pruesse E, Yilmaz P, Gerken J, Schweer T, Yarza P et al (2013) The SILVA ribosomal RNA gene database project: improved data processing and web-based tools. Nucleic Acids Res 41(Database issue):D590-596. https://doi.org/10.1093/nar/gks1219
Yilmaz P, Parfrey LW, Yarza P, Gerken J, Pruesse E, Quast C et al (2014) The SILVA and “All-species Living Tree Project (LTP)” taxonomic frameworks. Nucleic Acids Res 42:D643–D648. https://doi.org/10.1093/nar/gkt1209
Mohamed I, Zakeer S, Azab M, Hanora A (2020) Changes in vaginal microbiome in pregnant and nonpregnant women with bacterial vaginosis: toward microbiome diagnostics? OMICS 24:602–614. https://doi.org/10.1089/omi.2020.0096
Reid G (2019) The need to focus on therapy instead of associations. Front Cell Infect Microbiol 9:327. https://doi.org/10.3389/fcimb.2019.00327
Rajpoot M, Sharma AK, Sharma A, Gupta GK (2018) Understanding the microbiome: emerging biomarkers for exploiting the microbiota for personalized medicine against cancer. Semin Cancer Biol 52:1–8. https://doi.org/10.1016/j.semcancer.2018.02.003
Sender R, Fuchs S, Milo R (2016) Revised estimates for the number of human and bacteria cells in the body. PLoS Biol 14:e1002533. https://doi.org/10.1371/journal.pbio.1002533
Tortelli BA, Lewis WG, Allsworth JE, Member-Meneh N, Foster LR, Reno E et al (2020) Associations between the vaginal microbiome and Candida colonization in women of reproductive age. Am J Obstet Gynecol 222:471.e1-471.e9. https://doi.org/10.1016/j.ajog.2019.10.008
Ravel J, Gajer P, Abdo Z, Schneider GM, Koenig SS, McCulle SL et al (2011) Vaginal microbiome of reproductive-age women. Proc Natl Acad Sci U S A 108(Suppl 1):4680–4687. https://doi.org/10.1073/pnas.1002611107
Pybus V, Onderdonk AB (1997) Evidence for a commensal, symbiotic relationship between Gardnerella vaginalis and Prevotella bivia involving ammonia: potential significance for bacterial vaginosis. J Infect Dis 175:406–413. https://doi.org/10.1093/infdis/175.2.406
Cox C, Watt AP, McKenna JP, Coyle PV (2016) Mycoplasma hominis and Gardnerella vaginalis display a significant synergistic relationship in bacterial vaginosis. Eur J Clin Microbiol Infect Dis 35:481–487. https://doi.org/10.1007/s10096-015-2564-x
Funding
Open Access funding provided by University of Helsinki including Helsinki University Central Hospital. The EMMI pilot study was supported by research grants from the Southwest Finland Cultural Foundation, government research grant awarded to Turku University Hospital (EVO foundation) and Southwest Finland Cancer Association.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by KK, NH, JR, TK, and EM. The first draft of the manuscript was written by KK, NH, AA, and JR, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
The study was approved by the Ethics Committee of the Hospital District of Southwest Finland (nro 97/1801/2016).
Competing interests
EM is currently working as full-time Medical Advisor for Biocodex Nordics.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kero, K., Hieta, N., Kallonen, T. et al. Optimal sampling and analysis methods for clinical diagnostics of vaginal microbiome. Eur J Clin Microbiol Infect Dis 42, 201–208 (2023). https://doi.org/10.1007/s10096-022-04545-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10096-022-04545-x