
Abstract
Background
Event-related potentials (ERPs) reflect cognitive processing: negative early components (N100, N200) are involved in the sensory and perceptual processing of a stimulus, whereas late positive component P300 requires conscious attention. Both neuropsychological and affective disorders are present in patients with spinocerebellar ataxia type 1 (SCA1), but the underlying mechanisms need further clarification.
Materials and methods
In this pilot study, we assessed cognitive processing by recording auditory ERPs in 16 consecutive SCA1 patients and 16 healthy controls (HC) matched for age and sex. Motor and nonmotor symptoms were evaluated using the Scale for the Assessment and Rating of Ataxia (SARA) and an extensive neuropsychological battery. ERPs were recorded using an oddball paradigm, and peak latency and amplitude of N100, N200, and P300 were measured in the averaged responses to target tones.
Results
We found in SCA1 significantly increased latencies of N200 and P300 (p=0.033, p=0.007) and decreased amplitudes of N100 and P300 (p=0.024, p=0.038) compared with HC. Furthermore, P300 latency had the highest AUC in the discrimination of SCA1 in ROC analysis. The expansion of trinucleotide repeats correlated with P300 latency (r=−0.607, p=0.048), whereas both P300 and N100 amplitudes correlated with the severity of motor symptoms (r=−0.692, p=0.003; r=−0.621; p=0.010). Significant correlations between P300 latency and the scores of Emotion Attribution Task (r=−0.633, p=0.027), as well as between N200 latency and the scores of Frontal Assessment Battery and Stroop test (r=−0.520, p=0.047; r=0.538, p=0.039), were observed.
Conclusions
This research provides for the first time an extensive characterization of ERPs as useful electrophysiological markers to identify early cognitive dysfunction in SCA1.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
The spinocerebellar ataxias (SCAs) are a heterogeneous group of neurodegenerative disorders characterized by the main involvement of cerebellar functions and an autosomal dominant inheritance. Both repeat expansions and non-repeat mutations have been described, mostly causing damage to cerebellar Purkinje neurons, even though other parts of the central and peripheral nervous system can be involved [1]. Spinocerebellar ataxia type 1 (SCA1) represents 3–16 % of all SCAs and has a global prevalence of 1–2 in 100,000 with significant geographical variations [2]. Along with cerebellar motor deterioration, cognitive and affective functions may also be affected, contributing to the development of the cerebellar cognitive affective syndrome (CCAS) described by Schmahmann in 1998 [3]. The involvement of executive functions, orientation, and logical reasoning was observed by Ma et al. [4]. Moriarty and colleagues further reported in different subtypes of SCAs decreased function in the executive, visual memory, and social-affective domains, finding the most rapid cognitive decline in SCA1 patients [5]. Since SCA1 is a multi-domain neurodegenerative disorder, several studies explored the integrity of different pathways using neurophysiology, reporting abnormalities in visual, motor, somatosensory, and brainstem auditory evoked potentials [6]. Nonetheless, less is known about endogenous event-related potentials (ERPs) in SCAs. ERPs are known to primarily provide valuable information about attention and memory function: in the “oddball” paradigm subjects respond only to a specific target stimulus randomly presented with non-target stimuli, which implies the updating of working memory and the relocation of attentive resources. ERPs mirror cognitive processing from the evaluation of earlier sensory stimuli to later cognitive components requiring attentional resources: early components reflect sensory and perceptual processing of a stimulus and occur without or before conscious attention from the participant, whereas later components require conscious attention. The N100 reflects a change in auditory stimulation, like the offset and onset of sounds [7]. Typically evoked 190 and 360 ms after the presentation of a specific visual or auditory stimulus, the N200 is a fronto-central negative wave reflecting cognitive processes of stimulus evaluation and resulting from a deviation from a prevailing stimulus [8]. In the context of an oddball paradigm, the mismatch negativity (MMN), or auditory N2a, is elicited in a task-independent manner and reflects the discrimination between the deviating stimulus and the sensory-memory representation of the standard stimulus [9]. This component is independent of attention and top-down processes and can be found in both comatose patients and unresponsive wakefulness syndrome [10]. The P300 is a later (typically >250 ms) component, believed to be an index of active cognitive processing, especially attention and memory processes [11]. Different generators have been identified including the frontal and parietal cortex, amygdala, hippocampus, parahippocampal gyrus, temporal lobe, and basal ganglia. It requires the participant to pay attention to all the stimuli and categorize the difference between the standard and the rare target stimuli [11]. All ERP waveforms can be quantitatively characterized in amplitude and latency: the amplitude depends on the amount of neural activation, whereas the latency reveals the timing of this activation.
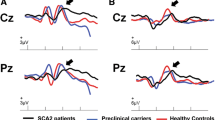
ERPs have been widely employed to investigate brain function in several disorders, i.e., Alzheimer’s disease (AD) and mild cognitive impairment (MCI) [12, 13]. Recently, Rodrìguez-Labrada and colleagues explored in a cross-sectional study visual and auditory ERPs in 30 SCA2 patients, 20 preclinical carriers, and 33 healthy controls (HC) [14]: compared with HC, patients had increased P300 latencies and decreased P300 amplitudes, whereas preclinical carriers exhibited only a prolongation of P300 latencies. Intriguingly, visual P300 latencies were significantly associated with time-to-ataxia onset in preclinical carriers, thus identifying this measure as a feasible biomarker of the prodromal stage of the disease [14].
Even though previous research highlighted progressive cognitive dysfunction in SCA1 patients, the role of auditory ERPs is not yet fully elucidated. With the present study, we aim to provide a thorough characterization of auditory ERP components (N100, N200, and P300) in SCA1 compared with HC and explore the relationship between ERPs and motor/cognitive measures.
Methods
Subjects
Genetically determined SCA1 patients referring to our outpatient clinic for movement disorders were consecutively examined for eligibility criteria. Demographic and clinical data were collected, and SCA1 patients were evaluated for motor symptoms and global cognition by neurologists with experience in movement disorders through the Scale for the Assessment and Rating of Ataxia (SARA) [15] and Mini-Mental State Examination (MMSE) [16]. As exclusion criteria, we considered: severe cerebellar impairment with SARA score > 24 or cognitive impairment with MMSE < 24 (to maximize adherence to the study protocol), and a history of hearing loss. The initial cohort consisted of 17 patients (9 males and 8 females), but one subject was excluded from the study because ERP components were poorly discernible. Therefore, the final analysis was performed on N = 16 (9 males and 7 females) SCA1 patients. Apart from two sisters belonging to the same family, the other participants were not consanguineous. We also recruited 16 HC, without any history of neurological or psychiatric disorders or concurrent treatment with drugs acting on the central nervous system, who were strictly matched to patients 1:1 for age (± 1 year) and sex. The institutional Ethics Committee approved the study protocol (CE 453/2021), and all subjects gave their informed written consent. The study was conducted according to the Declaration of Helsinki and followed international research ethical principles involving human subjects.
Neuropsychological testing
At enrollment, SCA1 patients were examined through an extensive neuropsychological battery including the following tests: Frontal Assessment Battery (FAB) [17], FAS for verbal fluency [18], Trail Making Test (TMT) [19], Raven Colored Progressive Matrices (RCPM) [20], Stroop Color and Word Interference Test (SCWT) [21], Rey-Osterrieth Complex Figure (ROCF) [22], and Babcock’s short tale (BST) [23]. The Emotion Attribution Task (EAT) [24] and Visual Analogue Test for Anosognosia for motor impairment (VATA-m) [25] were also administered to explore affective and self-awareness functions. We used Italian validated versions, and raw scores were adjusted for gender, age, and educational level according to established correction grids. Individual test performance was considered abnormal according to available cutoff scores.
Electrophysiological assessment
Within 1 month of clinical and neuropsychological evaluation, all patients underwent electrophysiological assessment for ERP analysis. Briefly, we used KeypointTM software (Natus Neurology Incorporated, Middleton, WI, USA) and administered auditory stimuli (average 74.97 ± 3.15 dB sound level to avoid uncomfortableness) using an oddball paradigm. The oddball paradigm consisted of at least 100 “standard” and “target” stimuli presented binaurally via earphones. Standard stimuli had 80% presenting probability and 2000-Hz frequency, whereas target stimuli had 20% presenting probability and 1500-Hz frequency. All tones were presented in a pseudo-randomized manner, had a 200-ms duration and an interstimulus interval of 1200 ms. In our experiment, subjects were instructed to concentrate on target stimuli: a brief practice trial was carried out to allow the correct discrimination between standard and target stimuli, and then subjects were asked to perform a simple motor task (e.g., clicking the pen tip) upon the onset of target tones. In the meantime, EEG signals were recorded from the scalp using Ag/AgCl electrodes at Fz, Cz, and Pz sites of the international 10/20 system, referred to linked earlobe electrodes. The ground electrode was located on the right hand, and impedance was kept below 5 kOhm. EEGs were filtered with a bandpass of 0.5–50 Hz and epochs were segmented at intervals of 100 ms pre-stimulus and 900 ms after-stimulus. Electrooculographic (EOG) recording was obtained, and artifact rejection was applied to remove trials with blinks (EOG voltage exceeding 75 μV) and other movements [26]. The responses to target and standard stimuli were averaged separately and at least two trials for each subject were conducted to prove the consistency of the waveforms. Peak latency and amplitude of components N100, N200, and P300 were measured in the averaged responses to target tones. We analyzed data recorded from the Cz electrode, where ERP components showed their maximum amplitude. N100, N200, and P300 components were identified. In the case of multi-peak morphology, the highest peak was chosen. When P300 subcomponents were recognizable, we considered for analysis the P3b, which better reflects the allocation of attentional resources for stimulus evaluation and memory updating [27]. Amplitude was determined using the baseline-to-peak method. The main steps of the employed paradigm are summarized in Fig. 1.

Schematic representation of the oddball paradigm employed for ERP acquisition
Statistical analysis
Variables were expressed as counts and percentages when categorical and as mean ± standard deviation (SD) when continuous. The normality of data was assessed using the Shapiro-Wilk test. Differences between groups were analyzed through parametric Student’s t-test for independent samples or non-parametric Mann-Whitney U test as appropriate. Comparisons between categorical variables were assessed using Fisher’s exact test. A receiver operating characteristic (ROC) curve analysis was carried out to establish ERP components’ discriminatory power. The area under the curve (AUC) and significance values were obtained. AUC values interpretation was determined according to Mandrekar et al. [28]. The relationship between neuropsychological, clinical, and electrophysiological measures in the SCA1 group was assessed through Spearman correlation analysis. Partial correlation analysis was also employed to control for the potential confounding effect of cerebellar motor symptoms in the assessment of neuropsychological tests. The significance level was set to p < 0.05. Since this research was a pilot study, we did not apply any correction for multiple comparisons. All analyses were performed using SPSS Version 25 (IBM Corporation, Armonk, USA) and GraphPad Prism version 8 (GraphPad Software Inc., San Diego, USA).
Results
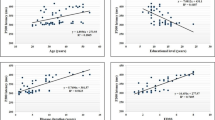
Complete clinical, demographic, and electrophysiological characteristics of SCA1 patients and matched HC are shown in Table 1. SCA1 patients were 47.69 ± 8.16 years old, with an average age at onset of 41.27 ± 8.50 years, average disease duration of 6.47 ± 3.62 years, and mean score of the SARA scale = 11.53 ± 5.14. There were no statistically significant differences regarding age, sex, and educational level between groups. Analysis of ERPs revealed in SCA1 patients significantly increased latencies of N200 and P300 (p = 0.033, p = 0.007) and decreased amplitudes of N100 and P300 (p = 0.024, p = 0.038) than HC; see Table 1 and Fig. 2. We then used ROC curve analysis to establish which ERP component could represent the most reliable electrophysiological signature of SCA1 patients and found that P300 latency showed the highest AUC (0.777, p = 0.007); see Table 2. Furthermore, we found moderate inverse correlations between the severity of SARA score and the amplitudes of P300 (r = −0.692, p = 0.003) and N100 (r = −0.621, p = 0.010), and between P300 latency and the number of CAG repeats in the expanded allele (r = −0.607, p = 0.048); see Supplementary Table S1.

Means of latency and amplitude values of ERP components are plotted. Error bars represent standard deviations. Significant between-groups differences (p-value < 0.05) are highlighted with the asterisk
Regarding neuropsychological assessment, the average test scores of the whole cohort were within normal limits. Nonetheless, out of 16 subjects, some showed impaired performances in the following: FAB (12.5%), FAS (25%), TMT-A and TMT-B (18.7%), SCWT (6.2%), ROCF (12.5%), BST (6.2%), VATA-m (37.5%), and EAT (25%). Concerning the latter, we found that the recognition of fear and anger was mostly affected with error rates respectively of 62.5% and 75%. Significant correlations between neuropsychological test scores and the severity of cerebellar motor involvement were also observed (see Table 3). The relationship between neuropsychological and electrophysiological measures was then investigated using Spearman correlation analysis (see Supplementary Table S1). A moderate inverse correlation between P300 latency and EAT score (r = −0.633, p = 0.027) was found. Since we could not exclude the interference of dysarthria, dysmetria, and tremor in the assessment of some neuropsychological tests (namely FAB, FAS, SCWT, TMT-A, and TMT-B), SARA scores were used as a control variable in partial correlation analysis. Moderate correlations were confirmed between N200 latency and both FAB (r = −0.520, p = 0.047) and SCWT (r = 0.538, p = 0.039).
Discussion
This study provided an extensive neuropsychological and electrophysiological evaluation of a homogeneous cohort of SCA1 patients. Even though the overall cognitive performances were within normal limits, early differences in auditory ERPs could be detected in SCA1. Indeed, compared with HC, average latency values of N200 and P300 were increased and average amplitudes of N100 and P300 were decreased. We also found that, among ERP measures, P300 latency was the most useful electrophysiological marker in the discrimination of SCA1 from HC, whereas the severity of cerebellar motor symptoms significantly correlated with both P300 and N100 amplitudes. Lastly, P300 and N200 latency showed significant correlations with the scores obtained on EAT, FAB, and SCWT tests. Taken together, these findings suggest the early involvement in SCA1 patients of specific networks engaged in the generation of ERPs and their relationship with both motor and non-motor features.
The role of the cerebellum as a key component interacting with cortical areas in the control of attentional processes has been highlighted in previous literature: Mannarelli et al. studied the effects of transcranial direct current stimulation (tDCS) delivered over the left cerebellar hemisphere in 15 healthy participants and found that cathodal cerebellar tDCS significantly decreased neural excitability through hyperpolarization and reduced the amplitude of N100, N200, and P300 [29]. Hyperpolarization may suppress cerebellar-brain inhibition (CBI), a functional pathway promoting the coordination and synchronization of both motor and non-motor circuits through the interaction at different levels of the cerebellothalamocortical tract. Since the cerebellum is involved in the temporal and spatial tuning of cortical activity, inhibitory cathodal tDCS could promote the desynchronization of cortical neurons and the altered allocation of selective attentional resources from the early phase of stimulus perception to its discrimination [29]. Our findings are in line with previous research reporting significantly increased latency and decreased amplitude of auditory and visual P300 in chronic neurodegenerative disorders involving the cerebellum [14, 30]. On the other hand, in contrast with previous research [30], we found that N200 latency may also provide an acceptable AUC in detecting SCA1 and shows moderate correlations with frontal function scores. Even though N200 could be partly influenced by exogenous factors and is mainly involved in stimulus categorization, the role of this component in cognitive processing is being increasingly recognized. Bennys and colleagues reported that N200 is a feasible biomarker of cognitive deterioration in MCI and preclinical AD patients [31]. N200 latency prolongation has been also described in subcortical patterns of cognitive deterioration, i.e., Parkinson’s disease (PD) [32]. Tachibana and colleagues described ERPs during semantic discrimination tasks in six patients with pure cerebellar atrophy and two patients with olivopontocerebellar atrophy, reporting longer N200 latencies [33]. Concerning the earliest stages of information processing, decreased N100 amplitude was reported in PD [34], whereas N100 latency was increased in both cerebellar [30] and non-cerebellar disorders [35] and showed significant correlations with visual working memory tasks [36].
Intriguingly, in our study, P300 latency was the only neurophysiological measure correlating with EAT score. It was previously reported that anodal high-definition tDCS over the temporoparietal junction (one of the P300 generators) determined improvement in facial emotion processing performance in healthy subjects [37]. Furthermore, both the cerebellum and basal ganglia are involved in the cortical-subcortical networks underlying the recognition and discrimination of emotions. Notably, negative emotions are thought to activate phylogenetically older circuits (including the cerebellum) than positive ones, probably reflecting a defense system against potential threats [38], which is in line with the results of the present study. Even though research on non-invasive stimulation to improve emotional impairment in SCA1 patients is lacking, Ruggiero and colleagues observed in PD that anodal cerebellar tDCS enhances emotional recognition in response to sad facial expressions by about 16%, whereas no improvement was observed in the recognition of happiness and neutral facial expressions [39].
The abnormalities of auditory ERP components may provide valuable insights into the brain mechanisms underlying the neuropsychological dysfunction characteristic of SCAs. More in detail, an early decline of attention, fluency, executive, visuospatial, and emotional functions in some patients of our cohort was observed, in line with previous literature [40]. Prominent executive and attentional dysfunction were reported in several studies evaluating cognitive profile in SCA1 [41,42,43,44,45, 4, 5, 46], worse than other SCAs [42, 43], whereas deficits in visuospatial perception and memory have yielded conflicting results [5, 41, 46]. Different involvement of phonemic and semantic fluency has been observed as well [47, 44,45,46]. These discrepancies may arise from the analysis of heterogenous testing of cognitive functions and relatively small sample sizes, as summarized in Table 4. In the context of cerebellar involvement in cognitive control, a meta-analysis [38] reported that language and executive tasks activate regions of the Crus I and lobule VII (involved in prefrontal-cerebellar loops), whereas emotional processing involved the vermal lobule VII, which is implicated in cerebellar-limbic circuitry. Additionally, our results highlight the role of anosognosia, as this domain was impaired in 37.5% of SCA1 patients. Even though cognitive mechanisms of anosognosia remain uncertain, previous evidence suggested in AD a significant correlation between anosognosia scores and the atrophy of the cerebellar vermis [48] and an interplay between the cerebellum and the anterior default mode network in non-memory anosognosia [49], thus supporting the need for a thorough assessment of self-awareness in cerebellar patients. Nonetheless, no significant correlations were found between VATA-m scores and ERPs, thus suggesting the limited feasibility of these electrophysiological measures as biomarkers of anosognosia.
To the best of our knowledge, this is the first research providing an extensive characterization of ERPs as early neurophysiological markers of cognitive dysfunction in a homogenous cohort of SCA1 patients. Our results also support the multiple system involvement in SCA1: on one side, we can hypothesize that cerebellar degeneration can likely alter P300 as a result of the dysfunction of cortico-cerebellar circuits; on the other, the key role of early components (N100, N200) suggests the participation of sensory pathways involved in the discrimination and categorization of auditory stimuli. Some limitations of the present study should be mentioned as well, such as (i) the unavailability of neuroimaging features that could have clarified any anatomical correlates of cognitive function; (ii) the lack of assessment of cognitive-affective functions in HC; (iii) the use of a neuropsychological battery with several ataxia-dependent tests; (iv) the cross-sectional design and small sample size, which require a cautious interpretation of these results; (v) the use of a simple auditory oddball paradigm, which may not be sufficient to explain complex cognitive processes. Nonetheless, several issues have been addressed: firstly, we carefully assessed the relationship between ataxia severity and neuropsychological test scores in partial correlation analysis, thus limiting the influence of motor impairment on cognitive outcomes. Secondly, even though the small number of patients and controls limited the power of statistical tests, the electrophysiological assessment was conducted through a strict matching procedure, thus controlling for the effect of age and gender in ERP components. Lastly, even though the cross-sectional design has several weaknesses, SCA1 patients involved in the present study are currently enrolled in a longitudinal protocol to further elucidate the usefulness of ERPs as biomarkers of cognitive dysfunction progression.
Conclusions
This pilot study highlights the feasible role of ERPs as neurophysiological markers of cognitive and emotional processing in SCA1 patients. Future studies, with prospective designs and involving larger cohorts, are therefore warranted to confirm these preliminary findings and further elucidate the underlying mechanisms of CCAS.
Data availability
Anonymized data can be obtained upon reasonable request from qualified researchers.
References
Klockgether T, Mariotti C, Paulson HL (2019) Spinocerebellar ataxia. Nat Rev Dis Primers 5:24. https://doi.org/10.1038/s41572-019-0074-3
Manto M, Marmolino D (2009) Cerebellar ataxias. Curr Opin Neurol 22:419–429. https://doi.org/10.1097/WCO.0b013e32832b9897
Schmahmann JD, Sherman JC (1998) The cerebellar cognitive affective syndrome. Brain 121(Pt 4):561–579. https://doi.org/10.1093/brain/121.4.561
Ma J, Wu C, Lei J, Zhang X (2014) Cognitive impairments in patients with spinocerebellar ataxia types 1, 2 and 3 are positively correlated to the clinical severity of ataxia symptoms. Int J Clin Exp Med 7:5765–5771
Moriarty A, Cook A, Hunt H et al (2016) A longitudinal investigation into cognition and disease progression in spinocerebellar ataxia types 1, 2, 3, 6, and 7. Orphanet J Rare Dis 11:82. https://doi.org/10.1186/s13023-016-0447-6
Abele M (1997) Autosomal dominant cerebellar ataxia type I. Nerve conduction and evoked potential studies in families with SCA1, SCA2 and SCA3. Brain 120:2141–2148. https://doi.org/10.1093/brain/120.12.2141
Ofek E, Pratt H (2012) The effects of subjectively significant stimuli on subsequent cognitive brain activity. Physiol Behav 105:428–442. https://doi.org/10.1016/j.physbeh.2011.06.003
Tomé D, Barbosa F, Nowak K, Marques-Teixeira J (2015) The development of the N1 and N2 components in auditory oddball paradigms: a systematic review with narrative analysis and suggested normative values. J Neural Transm 122:375–391. https://doi.org/10.1007/s00702-014-1258-3
Näätänen R, Paavilainen P, Rinne T, Alho K (2007) The mismatch negativity (MMN) in basic research of central auditory processing: a review. Clin Neurophysiol 118:2544–2590. https://doi.org/10.1016/j.clinph.2007.04.026
Pruvost-Robieux E, Marchi A, Martinelli I et al (2022) Evoked and event-related potentials as biomarkers of consciousness state and recovery. J Clin Neurophysiol 39:22–31. https://doi.org/10.1097/WNP.0000000000000762
Polich J (2007) Updating P300: an integrative theory of P3a and P3b. Clin Neurophysiol 118:2128–2148. https://doi.org/10.1016/j.clinph.2007.04.019
Hedges D, Janis R, Mickelson S et al (2016) P300 amplitude in Alzheimer’s disease: a meta-analysis and meta-regression. Clin EEG Neurosci 47:48–55. https://doi.org/10.1177/1550059414550567
Jiang S, Qu C, Wang F et al (2015) Using event-related potential P300 as an electrophysiological marker for differential diagnosis and to predict the progression of mild cognitive impairment: a meta-analysis. Neurol Sci 36:1105–1112. https://doi.org/10.1007/s10072-015-2099-z
Rodríguez-Labrada R, Velázquez-Pérez L, Ortega-Sánchez R et al (2019) Insights into cognitive decline in spinocerebellar ataxia type 2: a P300 event-related brain potential study. Cerebellum Ataxias 6:3. https://doi.org/10.1186/s40673-019-0097-2
Weyer A, Abele M, Schmitz-Hübsch T et al (2007) Reliability and validity of the scale for the assessment and rating of ataxia: a study in 64 ataxia patients. Mov Disord 22:1633–1637. https://doi.org/10.1002/mds.21544
Folstein MF, Folstein SE, McHugh PR (1975) “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 12:189–198. https://doi.org/10.1016/0022-3956(75)90026-6
Appollonio I, Leone M, Isella V et al (2005) The Frontal Assessment Battery (FAB): normative values in an Italian population sample. Neurol Sci 26:108–116. https://doi.org/10.1007/s10072-005-0443-4
Costa A, Bagoj E, Monaco M et al (2014) Standardization and normative data obtained in the Italian population for a new verbal fluency instrument, the phonemic/semantic alternate fluency test. Neurol Sci 35:365–372. https://doi.org/10.1007/s10072-013-1520-8
Giovagnoli AR, Del Pesce M, Mascheroni S et al (1996) Trail making test: normative values from 287 normal adult controls. Ital J Neurol Sci 17:305–309. https://doi.org/10.1007/BF01997792
Basso A, Capitani E, Laiacona M (1987) Raven’s coloured progressive matrices: normative values on 305 adult normal controls. Funct Neurol 2:189–194
Caffarra P, Vezzadini G, Dieci F et al (2002) Una versione abbreviata del test di Stroop: dati normativi nella popolazione italiana. Nuova Riv Neurol 12:111–115
Carlesimo GA, Buccione I, Fadda L et al (2002) Standardizzazione di due test di memoria per uso clinico: Breve Racconto e Figura di Rey. Nuova Riv Neurol 12:1–13
Spinnler H (1987) Standardizzazione e taratura italiana di test neuropsicologici. Ital J Neurol Sci 6:21–120
Dodich A, Cerami C, Canessa N et al (2015) A novel task assessing intention and emotion attribution: Italian standardization and normative data of the Story-based Empathy Task. Neurol Sci 36:1907–1912. https://doi.org/10.1007/s10072-015-2281-3
Della Sala S, Cocchini G, Beschin N, Cameron A (2009) VATA-m: Visual-Analogue Test assessing Anosognosia for motor impairment. Clin Neuropsychol 23:406–427. https://doi.org/10.1080/13854040802251393
Remijn GB, Hasuo E, Fujihira H, Morimoto S (2014) An introduction to the measurement of auditory event-related potentials (ERPs). Acoust Sc Tech 35:229–242
Polich J (2004) Clinical application of the P300 event-related brain potential. Phys Med Rehabil Clin N Am 15:133–161. https://doi.org/10.1016/S1047-9651(03)00109-8
Mandrekar JN (2010) Receiver operating characteristic curve in diagnostic test assessment. J Thorac Oncol 5:1315–1316. https://doi.org/10.1097/JTO.0b013e3181ec173d
Mannarelli D, Pauletti C, De Lucia MC et al (2016) Effects of cerebellar transcranial direct current stimulation on attentional processing of the stimulus: evidence from an event-related potentials study. Neuropsychologia 84:127–135. https://doi.org/10.1016/j.neuropsychologia.2016.02.002
Yang J-C, Chan S-H, Khan S et al (2013) Neural substrates of executive dysfunction in fragile X-associated tremor/ataxia syndrome (FXTAS): a brain potential study. Cereb Cortex 23:2657–2666. https://doi.org/10.1093/cercor/bhs251
Bennys K, Portet F, Touchon J, Rondouin G (2007) Diagnostic value of event-related evoked potentials N200 and P300 subcomponents in early diagnosis of Alzheimer’s disease and mild cognitive impairment. J Clin Neurophysiol 24:405–412. https://doi.org/10.1097/WNP.0b013e31815068d5
Raudino F, Garavaglia P, Beretta S, Pellegrini G (1997) Auditory event-related potentials in Parkinson’s disease. Electromyogr Clin Neurophysiol 37:409–413
Tachibana H, Aragane K, Sugita M (1995) Event-related potentials in patients with cerebellar degeneration: electrophysiological evidence for cognitive impairment. Brain Res Cogn Brain Res 2:173–180. https://doi.org/10.1016/0926-6410(95)90006-3
Lagopoulos J, Gordon E, Lim CL et al (1997) Automatic processing dysfunction in Parkinson’s disease. Neurol Res 19:609–612. https://doi.org/10.1080/01616412.1997.11740868
Golob EJ, Ringman JM, Irimajiri R et al (2009) Cortical event-related potentials in preclinical familial Alzheimer disease. Neurology 73:1649–1655. https://doi.org/10.1212/WNL.0b013e3181c1de77
Annanmaki T, Palmu K, Murros K, Partanen J (2017) Altered N100-potential associates with working memory impairment in Parkinson’s disease. J Neural Transm (Vienna) 124:1197–1203. https://doi.org/10.1007/s00702-017-1758-z
Donaldson PH, Kirkovski M, Rinehart NJ, Enticott PG (2019) A double-blind HD-tDCS/EEG study examining right temporoparietal junction involvement in facial emotion processing. Soc Neurosci 14:681–696. https://doi.org/10.1080/17470919.2019.1572648
Stoodley CJ, Schmahmann JD (2009) Functional topography in the human cerebellum: a meta-analysis of neuroimaging studies. Neuroimage 44:489–501. https://doi.org/10.1016/j.neuroimage.2008.08.039
Ruggiero F, Dini M, Cortese F et al (2022) Anodal transcranial direct current stimulation over the cerebellum enhances sadness recognition in Parkinson’s disease patients: a pilot study. Cerebellum 21:234–243. https://doi.org/10.1007/s12311-021-01295-y
Giocondo F, Curcio G (2018) Spinocerebellar ataxia: a critical review of cognitive and socio-cognitive deficits. Int J Neurosci 128:182–191. https://doi.org/10.1080/00207454.2017.1377198
Bürk K, Bösch S, Globas C et al (2001) Executive dysfunction in spinocerebellar ataxia type 1. Eur Neurol 46:43–48. https://doi.org/10.1159/000050755
Bürk K, Globas C, Bösch S et al (2003) Cognitive deficits in spinocerebellar ataxia type 1, 2, and 3. J Neurol 250:207–211. https://doi.org/10.1007/s00415-003-0976-5
Klinke I, Minnerop M, Schmitz-Hübsch T et al (2010) Neuropsychological features of patients with spinocerebellar ataxia (SCA) types 1, 2, 3, and 6. Cerebellum 9:433–442. https://doi.org/10.1007/s12311-010-0183-8
Orsi L, D’Agata F, Caroppo P et al (2011) Neuropsychological picture of 33 spinocerebellar ataxia cases. J Clin Exp Neuropsychol 33:315–325. https://doi.org/10.1080/13803395.2010.518139
Fancellu R, Paridi D, Tomasello C et al (2013) Longitudinal study of cognitive and psychiatric functions in spinocerebellar ataxia types 1 and 2. J Neurol 260:3134–3143. https://doi.org/10.1007/s00415-013-7138-1
Nigri A, Sarro L, Mongelli A et al (2022) Spinocerebellar ataxia type 1: one-year longitudinal study to identify clinical and MRI measures of disease progression in patients and presymptomatic carriers. Cerebellum 21:133–144. https://doi.org/10.1007/s12311-021-01285-0
Sokolovsky N, Cook A, Hunt H et al (2010) A preliminary characterisation of cognition and social cognition in spinocerebellar ataxia types 2, 1, and 7. Behav Neurol 23:17–29. https://doi.org/10.1155/2010/395045
Guerrier L, Le Men J, Gane A et al (2018) Involvement of the cingulate cortex in anosognosia: a multimodal neuroimaging study in Alzheimer’s disease patients. J Alzheimers Dis 65:443–453. https://doi.org/10.3233/JAD-180324
Valera-Bermejo JM, De Marco M, Venneri A (2021) Altered interplay among large-scale brain functional networks modulates multi-domain anosognosia in early Alzheimer’s disease. Front Aging Neurosci 13:781465. https://doi.org/10.3389/fnagi.2021.781465
Acknowledgements
The authors wish to acknowledge Fondazione A.c.a.Re.f (Ferrara) and Associazione Nazionale AISA (Associazione Italiana per la lotta alle Sindromi Atassiche) for their support.
Funding
Open access funding provided by Università degli Studi di Ferrara within the CRUI-CARE Agreement.
Author information
Authors and Affiliations
Contributions
EC and MS: study concept, data interpretation, and writing of the first draft of the manuscript; EC, FC, MRN, ED, and AB: ERP data collection and analysis; EC and ACP: neuropsychological data collection and analysis; MS, JGC, and VT: study design, data interpretation, and manuscript editing.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no relevant financial or non-financial interests to disclose.
Ethical approval
The study was approved by the local Ethics Committee of the University of Ferrara (CE 453/2021). The study has been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Informed consent
Written informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
ESM 1
(DOCX 18 kb)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Contaldi, E., Sensi, M., Colucci, F. et al. Electrophysiological and neuropsychological assessment of cognition in spinocerebellar ataxia type 1 patients: a pilot study. Neurol Sci 44, 1597–1606 (2023). https://doi.org/10.1007/s10072-022-06597-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-022-06597-5