
Abstract
The iBerry Study, a Dutch population-based high-risk cohort (n = 1022) examines the transition from subclinical symptoms to psychiatric disorders in adolescents. Here, we present the first follow-up measurement, approximately 3 years after baseline assessment and 5 years after the screening based on self-reported emotional and behavioral problems (SDQ-Y). We give an update on the data collection, details on the (non)response, and the results on psychopathology outcomes. The first follow-up (2019–2022) had a response rate of 79% (n = 807). Our results at baseline (mean age 15.0 years) have shown the effectiveness of using the SDQ-Y to select a cohort oversampled for the risk of psychopathology. At first follow-up (mean age 18.1 years), the previously administered SDQ-Y remains predictive for selecting adolescents at risk. At follow-up, 47% of the high-risk adolescents showed significant mental health problems based on self- and parent reports and 46% of the high-risk adolescents met the criteria for multiple DSM-5 diagnoses. Compared to low-risk adolescents, high-risk adolescents had a sevenfold higher odds of significant emotional and behavioral problems at follow-up. Comprehensive assessment on psychopathology, substance abuse, psychotic symptoms, suicidality, nonsuicidal self-injury, addiction to social media and/or video gaming, and delinquency, as well as social development, and the utilization of healthcare and social services were conducted. This wave, as well as the ones to follow, track these adolescents into their young adulthood to identify risk factors, elucidate causal mechanisms, and discern pathways leading to both common and severe mental disorders. Results from the iBerry Study will provide leads for preventive interventions.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The onset of mental disorders mostly occurs in adolescence and young adulthood. An estimated 62.5% of disorders begin before the age of 25, with a peak age at 14.5 years [1]. These disorders are associated with negative outcomes on educational, occupational, and social domains [2,3,4,5,6,7,8]. Compared to those without psychiatric problems, individuals with a psychiatric disorder in their youth are nine times more likely to face negative outcomes on these domains in the transition to adulthood. For youth with subthreshold problems this is five times [9]. Early onset of psychiatric problems is associated with high persistence and negative prognosis [8, 10,11,12].
The etiology of psychiatric disorders is complex. Studies have shown that psychiatric disorders have a multifactorial etiology and that risk factors are pleiotropic [13,14,15]. Particularly in adolescence, the symptoms in the early stages of disorders tend to be non-specific [16, 17]. Subsequently, there are high comorbidity rates between psychiatric disorders as well as heterotypic continuity over time [11, 18,19,20]. This underlines the importance of a transdiagnostic approach in research [21].
To advance a more preventive and transdiagnostic approach in psychiatry, more epidemiological knowledge, especially on individual and environmental exposures, is necessary [7]. This knowledge could be used in individual prediction models for targeted prevention strategies [22, 23]. Considerable effort has been made to study the etiology of psychopathology, but this has been complicated by selective drop-out bias in general population studies, referral bias in patient-based samples, and a focus on a specific diagnosis or inheritance pattern in familial loading studies [24]. More accurate, large-sample deep-phenotype data in a high-risk population is likely to overcome these difficulties [16, 21].
The design of the iBerry (Investigating Behavioral and Emotional Risk in Rotterdam Youth) Study follows a cross-diagnostic approach that cuts across traditional diagnostic boundaries to examine the etiology and course of psychopathology instead of maintaining nosological boundaries with a focus on a single diagnostic category. The main aim of the iBerry Study is to examine the developmental course of psychiatric disorders and associated risk factors to contribute to the development of preventive interventions. The current paper discusses the design and protocol of the first follow-up measurement and gives a cohort profile update, details on the (non) response, and the prevalence of adolescent and parental psychopathology. Furthermore, the long-term effectiveness of using a screening questionnaire to select a cohort oversampled on their self-reported emotional and behavioral problems is discussed.
Study design
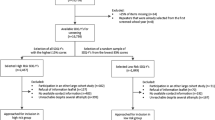
The iBerry Study is a cohort study of adolescents from the general population who were oversampled on their self-reported emotional and behavioral problems. The study is conducted in the greater Rotterdam area in the Netherlands, this region contains a combination of the highly urbanized city of Rotterdam, the surrounding suburban cities, and more rural villages [25]. The current study discusses the details from the first follow-up measurement (T1), the screening procedure at age 13 and baseline measurement at age 15 were described in detail elsewhere [24]. A concise graphical overview of the iBerry Study is presented in Fig. 1.

Overview of the design and summary of the different phases of the iBerry Study
Eligibility
As described previously by Grootendorst-van Mil and Bouter et al. [24], adolescents were selected for participation in the iBerry Study based on a questionnaire administered in the first year of secondary school as part of standard preventive healthcare performed by community Child and Family Centers in the Netherlands. All adolescents (mean age 13.1 years) filled out the Strengths and Difficulties Questionnaire–Youth (SDQ-Y), to assess their emotional and behavioral problems [26]. Unless the adolescent or their parent(s)/guardian(s) objected, all questionnaires from the school years 2014–2015 and 2015–2016 were screened. From these 16,736 screened questionnaires, adolescents with the highest 15% problem scores were selected, together with a random selection of adolescents with the lower 85% problem scores, resulting in the inclusion of 1,022 adolescents at baseline (September 2015–September 2019, response rate at enrollment 54%).
Enrollment at the first follow-up
Participants from the baseline measurement were contacted for the first follow-up measurement and 807 adolescents (79.0%) participated at T1. Data were collected between March 2019 and June 2022. Because the COVID-19 pandemic occurred during this measurement, we added two additional online measurements to collect data on emotional and behavioral problems during the lockdowns [27]. The median interval between the SDQ-Y screening and T1 was 4.7 years (IQR 4.5–5.4). The time between baseline and T1 had a median interval of 3.1 years (IQR 3.0–3.5).
Response rate
215 adolescents (21.0%) included at baseline did not participate at T1. A small number of participants objected to being contacted for follow-up measurements (n = 13, 1.3%). 71 adolescents (6.9%) declined participation in the first follow-up. The most common reasons for declining were a lack of interest (n = 48, 4.7%) or time (n = 10, 1.0%). The remaining 131 adolescents (12.8%) could not be reached.
Response rates were comparable for the high-risk adolescents (78.3%) and low-risk adolescents (80.6%), and the distributions of high-risk and low-risk adolescents were approximately equal in the responders and the non-responders (χ2 = 0.676, p = 0.411). A detailed overview of the baseline characteristics of responders and non-responders is provided in Supplementary table S1. Non-responders more often were male, had a higher age at baseline, had a non-Dutch ethnic background, had a lower educational level, and belonged to a lower income household. Non-responders were not more likely to score above the borderline cut-off for emotional and behavioral problems (measured with the Youth Self-Report) at baseline. Significant differences showed small effect sizes. Importantly, those non-responders at T1 were more frequently associated with incomplete baseline measurements, indicating that obtaining comprehensive data from this group was already challenging during the cohort's initial assessment.
Objectives
The iBerry Study aims to investigate the transition of subclinical symptoms to full-blown psychiatric disorders in adolescents who enter young adulthood. We use a cross-diagnostic approach to study all psychiatric disorders. The aim is to identify risk and protective factors and examine the mechanisms underlying the development of psychopathology.
Measurements
Assessment procedure
The adolescents were invited to the research center with one of their parents for a three-hour visit. All participants signed informed consent forms. All researchers were blinded from the SDQ-Y scores during the baseline assessment and follow-up measurements.
Details on data quality, control and management, and privacy protection have been described previously [24]. All protocols have been updated to ensure adherence to all applicable rules and regulations.
Main outcomes
The main aim is to study the long-term prognosis of adolescent subclinical psychiatric symptoms. We want to examine which determinants can predict the transition of subclinical symptoms to psychiatric disorders. To assess psychopathology we used various methods, including the Achenbach System of Empirically Based Assessment (ASEBA) questionnaires and the MINI Neuropsychiatric interview for DSM-5 diagnoses [28,29,30]. Specifically, we conducted detailed assessments of psychotic experiences [31], suicidality and nonsuicidal self-injury (NSSI) [32,33,34], and autism [35]. Subsequent studies will be conducted to examine the various determinants and the in depth measurements of psychopathology.
Main determinants
A broad range of biological, psychological, and social markers is assessed. At T1 these included socio-demographic characteristics, general functioning, sensory processing, aggressive and delinquent behavior, lifestyle and addiction, health care use and costs, personality, coping, family functioning, parenting, peers, relationships, sexuality, (adverse) life events and trauma, neuropsychological functioning, somatic complaints, anthropometry, and puberty development. We also collected detailed information on sleep and movement which was assessed using nine-day actigraphy measurements and a daily diary. Parents also provided information on parental psychopathology, personality, substance use, and anthropometry. A complete overview of all measurements is provided in Supplementary table S2.
Biological samples
Biological measurements at baseline were repeated at T1; we again obtained a blood and a hair sample from both the adolescent and from the accompanying parent.
Characteristics of the study cohort
Socio-demographic characteristics
Socio-demographic characteristics of the adolescents and their parents are presented in Table 1. At the first follow-up the adolescents in the cohort had a mean age of 18.1 years, 53.5% were female, 23.6% had a non-Dutch ethnic background, 61% lived in an urban area, and vocational education was the most reported education level. For 85.1% of the adolescents, one of their parents (83.4% mothers) also participated in the study. High-risk and low-risk adolescents differed on educational level, whether they participated with a parent, parental education level, and household income level, albeit with small effect sizes. The oversampled ratio of high-risk to low-risk adolescents remained consistent between baseline (2.5:1) and T1 (2.4:1), 570 high-risk adolescents (70.6%) and 237 low-risk adolescents (29.4%) participated at T1.
Emotional and behavioral problems
Emotional and behavioral problems, as measured with the Youth Self-Report (YSR) and Child Behavior Checklist (CBCL), are described in Table 2. In the high-risk group 37.1% of the adolescents reported problems in the borderline/clinical range (ASEBA norm scores, > 93rd percentile [28]), compared to 16.0% of the adolescents in the low-risk group. Combining the multi-informant questionnaires, 40.0% of the adolescents in the cohort (47.0% in the high-risk group, 23.1% in the low-risk group) scored above the borderline cut-off on the Total Problems scale according to one or both informants. For all scales, more high-risk adolescents scored above the cut-off compared to the low-risk adolescents.
Adolescent psychopathology
In 729 adolescents a complete semi-structured interview for the DSM-5 diagnoses was conducted (Table 3). The most common diagnoses in the high-risk group were substance-related disorders (40.0%), followed by mood disorders (35.1%), and ADHD (29.5%). In the low-risk group, substance-related disorders were common (42.1%), followed by mood disorders (16.8%). Notably, the high-risk adolescents more often met the criteria for multiple diagnoses (46.0%) compared to the low-risk adolescents (24.8%).
Parental psychopathology
In line with the prevalences presented in our design paper [24], parents in the cohort showed higher rates of psychopathology in the past 2 years compared to the general population (Table 3). In the parents of high-risk adolescents 27.7% met the criteria for one DSM-IV diagnosis, 13.9% met the criteria for multiple DSM-IV diagnoses. In the parents of low-risk adolescents, these prevalences were 24.1% and 8.2%, respectively. Because a validated Dutch translation of the DSM-5 interview was not available at the start of T1, the same DSM-IV interview from the baseline measurement was used for consistency.
Predictiveness of SDQ-Y score
To investigate the longitudinal predictive value of the SDQ-Y score at age 13 on the development of emotional and behavioral problems, we used multilevel random intercept regression models. We used sex, age, time, and an interaction term between time and risk status to model self-reported internalizing, externalizing, and YSR Total Problems scores. The estimated mean scores from linear mixed models for the three problem scales, stratified by SDQ-Y risk status, are visualized in Fig. 2. The coefficient estimates are summarized in Supplementary table S3. Next, we examined adolescents who reported internalizing, externalizing, and total problems above the borderline cut-off score. The odds ratios from the mixed effect logistic regression are presented in Table 4. Both in the linear and logistic models, we did not find an interaction effect between time and risk status. Between baseline and T1, the trajectory of emotional and behavioral problems did not differ between low and high-risk adolescents. Overall, both groups either remained equal or increased on emotional and behavioral problems. Notably, the difference between low and high-risk adolescents remained stable between baseline and T1, indicating that the SDQ-Y score is a good predictor of later psychopathology both in the short-term (baseline, after ~ 1–3 years) and in the medium-long term (T1, after ~ 4–6 years). Adolescents identified as high-risk had a four to sevenfold higher odds of scoring in the borderline range on internalizing, externalizing, and total problems compared to low-risk adolescents.

Estimated emotional and behavioral problem mean scores for the internalizing and externalizing subscales and the total problem scale at baseline and first follow-up measurement (T1) stratified by risk status
Statistical power
In future studies that make use of the collected data, not all analyses will be performed in the complete cohort because of loss to follow-up and missing values. Depending on the association under study, we will consider the information that is available for the main predictor and main outcome variable. Based on sample sizes ranging from 1000 to 500 (with an alpha value of 0.05 and 80% power), the study can detect a difference in standard deviation ranging from 0.18–0.25 (50% prevalence) to 0.41–0.58 (5% prevalence). These are detectable effect sizes using a dichotomous measure of exposure, which are considered conservative. Within the iBerry Study, we will often study the effect of continuous determinants and prognostic factors, assessed at multiple time points, which will further increase power.
Follow-up and retention strategies
All adolescents received gift certificates for their participation. All travel expenses were reimbursed. To keep in contact we send newsletters, birthday cards, and holiday cards. It is also possible to follow the study on social media channels. To minimize loss to follow-up we ensured the correctness of contact information at each contact. If an adolescent was unable to participate it was possible to make an appointment during the evening, online, as a home visit, or to postpone the visit for a couple of months. Lastly, if these possibilities were not an option a short questionnaire was sent to the adolescent to collect data on sociodemographic characteristics, emotional and behavioral problems, psychotic experiences, (adverse) life events, substance use, and self-harm. In a separate questionnaire parents provided additional information on emotional and behavioral problems, adverse life events, healthcare use, personality, executive functioning, and family functioning.
Data linkage and collaboration
The available information of the participants makes it possible to integrate the cohort data with other data sources. Environmental characteristics can be studied based on the home address to be linked with data from Statistics Netherlands or in collaboration with the Geoscience and health consortium [27, 36]. Furthermore, adolescents provided informed consent to obtain additional information on their health and development from their healthcare providers. We warmly welcome other researchers to collaborate by combining the iBerry cohort data with other studies.
Strengths and limitations
Our results show that the screening procedure was successful in selecting a cohort of adolescents at risk of psychopathology. Adolescents with a high score on emotional and behavioral problems at age 13 were four to seven times more likely to report significant emotional and behavioral problems at age 18. New normative SDQ-Y norms for Dutch adolescents showed that the 15% SDQ-Y cut-off used to select the high-risk population aligns with adolescents scoring above the borderline/clinical cut-off score [37]. This relative cut-off score where adolescents were compared to their peers, is an efficient way to select adolescents at risk for psychopathology as evidenced by the high levels of psychopathology in our cohort at follow-up.
The specific design of our cohort enables us to address a limitation of general population studies that suffer from drop-out dependent on less prevalent risk factors and outcomes. With the oversampled selection and the retention of adolescents at higher risk of psychopathology, we will continue to have the advantage of increased power to examine associations of interest. Despite oversampling individuals with a high risk for psychopathology, the risk factors that our study identifies are relevant to the general population as well. This enriched population might enable us to pick up risk factors that are more rare, but it is not likely that the oversampling will lead to spurious associations [38].
Although our retention rate is high, we still have adolescents who were lost to follow-up. As indicated by our non-response analyses, these adolescents do differ on socio-demographic characteristics from the adolescents who did participate. This could introduce bias in our results, which we will reduce as much as possible. Attrition will be addressed in a targeted manner for each association under study, for example by controlling analyses for potential confounders and by using multiple imputation methods [39,40,41,42,43,44]. Furthermore, the scientific inference of our findings will not necessarily be compromised. While a completely representative sample of the source population is valuable, broader scientific generalizations can sometimes hold more significance than strict sample representativeness, especially when examining associations between variables of interest [45]. Selective drop-out will likely result in biased estimations of prevalences, and by design the prevalences within the iBerry cohort will be higher than in the general population, but this will not likely affect the direction of the associations under study [46,47,48].
Future perspectives
Now that the cohort has been established and we have found successful retention strategies, we aim to follow up this cohort until young adulthood. Adolescents are invited for follow-up visits every 2–3 years. Currently, the third visit to the research center is being conducted. This visit includes both repeated as well as new age-appropriate measurements, such as an extensive assessment for personality disorders.
To ensure valid conclusions we will also request microdata, anonymized data at the level of private individuals from Statistics Netherlands (CBS), which enables us to study the outcome in both individuals participating in subsequent follow-up phases and in those who might be lost to follow-up.
Conclusion
The iBerry Study closely examines adolescents and their parents to determine a broad range of biological, psychological, and social markers for the transition of subclinical symptoms to psychiatric disorders. Adolescents were successfully selected based on their self-reported emotional and behavioral problems at age 13. The current data underscore an evident vulnerability in high-risk adolescents, manifesting in significant psychopathological problems by age 18. The research's in-depth measurements in combination with its design, anchored by its careful screening and retention strategies, create a foundation for numerous detailed future investigations into the complexities of adolescent psychopathology.
Availability of data and materials
Other researchers are welcome to collaborate with researchers in the iBerry Study group and to request access to the data. Proposals to collaborate will be assessed by the iBerry Study group with respect to quality, feasibility, and potential overlap with planned or published publications.
References
Lo Buglio G et al (2022) A network analysis of anxiety, depressive, and psychotic symptoms and functioning in children and adolescents at clinical high risk for psychosis. Front Psych 13:1016154
Mojtabai R et al (2015) Long-term effects of mental disorders on educational attainment in the National Comorbidity Survey ten-year follow-up. Soc Psychiatry Psychiatr Epidemiol 50(10):1577–1591
Holttinen T et al (2022) Educational attainment of adolescents treated in psychiatric inpatient care: a register study over 3 decades. Eur Child Adolesc Psychiatry 32:2163–2173
Meißner C et al (2022) Associations between mental health problems in adolescence and educational attainment in early adulthood: results of the German longitudinal BELLA study. Front Pediatr 10:828085
Gibb SJ, Fergusson DM, Horwood LJ (2010) Burden of psychiatric disorder in young adulthood and life outcomes at age 30. Br J Psychiatry 197(2):122–127
Iorfino F et al (2018) Delineating the trajectories of social and occupational functioning of young people attending early intervention mental health services in Australia: a longitudinal study. BMJ Open 8(3):e020678
Fusar-Poli P et al (2021) Preventive psychiatry: a blueprint for improving the mental health of young people. World Psychiatry 20(2):200–221
Erskine HE et al (2015) A heavy burden on young minds: the global burden of mental and substance use disorders in children and youth. Psychol Med 45(7):1551–1563
Copeland WE et al (2015) adult functional outcomes of common childhood psychiatric problems: a prospective, longitudinal study. JAMA Psychiat 72(9):892–899
Copeland WE et al (2013) Diagnostic transitions from childhood to adolescence to early adulthood. J Child Psychol Psychiatry 54(7):791–799
Caspi A et al (2020) Longitudinal assessment of mental health disorders and comorbidities across 4 decades among participants in the Dunedin birth cohort study. JAMA Netw Open 3(4):e203221–e203221
Piao J et al (2022) Alarming changes in the global burden of mental disorders in children and adolescents from 1990 to 2019: a systematic analysis for the Global Burden of Disease study. Eur Child Adolesc Psychiatry 31(11):1827–1845
Uher R, Zwicker A (2017) Etiology in psychiatry: embracing the reality of poly-gene-environmental causation of mental illness. World Psychiatry 16(2):121–129
Taylor JH et al (2020) Characteristics of youth with reported family history of psychosis spectrum symptoms in the Philadelphia Neurodevelopmental Cohort. Schizophr Res 216:104–110
Guloksuz S, van Os J, Rutten BPF (2018) The exposome paradigm and the complexities of environmental research in psychiatry. JAMA Psychiat 75(10):985–986
Shah JL et al (2020) Transdiagnostic clinical staging in youth mental health: a first international consensus statement. World Psychiatry 19(2):233–242
Hartmann JA et al (2019) At-risk studies and clinical antecedents of psychosis, bipolar disorder and depression: a scoping review in the context of clinical staging. Psychol Med 49(2):177–189
Plana-Ripoll O et al (2019) Exploring comorbidity within mental disorders among a Danish National Population. JAMA Psychiat 76(3):259–270
McGrath JJ et al (2020) Comorbidity within mental disorders: a comprehensive analysis based on 145 990 survey respondents from 27 countries. Epidemiol Psychiatr Sci 29:e153
Oldehinkel AJ, Ormel J (2023) Annual research review: stability of psychopathology: lessons learned from longitudinal population surveys. J Child Psychol Psychiatry 64(4):489–502
McGorry PD et al (2018) Beyond the “at risk mental state” concept: transitioning to transdiagnostic psychiatry. World Psychiatry 17(2):133–142
Salazar de Pablo G et al (2020) Implementing precision psychiatry: a systematic review of individualized prediction models for clinical practice. Schizophr Bull 47(2):284–297
Meehan AJ et al (2022) Clinical prediction models in psychiatry: a systematic review of two decades of progress and challenges. Mol Psychiatry 27(6):2700–2708
Grootendorst-van Mil NH et al (2021) The iBerry study: a longitudinal cohort study of adolescents at high risk of psychopathology. Eur J Epidemiol 36:453–464
Bouter DC et al (2023) Associations between the urban environment and psychotic experiences in adolescents. Schizophr Res 260:123–131
Goodman R et al (2004) Using the strengths and difficulties questionnaire (SDQ) multi-informant algorithm to screen looked-after children for psychiatric disorders. Eur Child Adolesc Psychiatry 13(2):ii25–ii31
Bouter DC et al (2023) A longitudinal study of mental health in at-risk adolescents before and during the COVID-19 pandemic. Eur Child Adolesc Psychiatry 32(6):1109–1117
Achenbach TM, Rescorla LA (2001) Manual for the ASBEA school-age forms & profiles. University of Vermont, Research Center for Children, Youth, & Families, Burlington
Bauhuis O et al (2013) MINI KID. De introductie van een Nederlandstalig instrument om DSM-IV-TR diagnoses bij kinderen te stellen. Kind en adolescent praktijk 1:20–26
Sheehan DV et al (2010) Reliability and validity of the Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-KID). J Clin Psychiatry 71(3):313–326
Ising HK et al (2012) The validity of the 16-item version of the prodromal questionnaire (PQ-16) to screen for ultra high risk of developing psychosis in the general help-seeking population. Schizophr Bull 38(6):1288–1296
Klonsky ED, Glenn CR (2009) Assessing the functions of non-suicidal self-injury: psychometric properties of the inventory of statements about self-injury (ISAS). J Psychopathol Behav Assess 31(3):215–219
Kerkhof AJFM et al (2015) VOZZ & VOZZ-SCREEN. Vragenlijst over zelfdoding en zelfbeschadiging. Handleiding. Vrije Universiteit Amsterdam, Amsterdam
Posner K et al (2011) The Columbia-suicide severity rating scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am J Psychiatry 168(12):1266–1277
Roeyers H et al (2015) SRS-2 Screeningslijst voor autismespectrumstoornissen. Hogrefe Uitgevers, Amsterdam
Lakerveld J et al (2020) Deep phenotyping meets big data: the Geoscience and hEalth Cohort COnsortium (GECCO) data to enable exposome studies in The Netherlands. Int J Health Geogr 19(1):49
Vugteveen J, de Bildt A, Timmerman ME (2022) Normative data for the self-reported and parent-reported strengths and difficulties questionnaire (SDQ) for ages 12–17. Child Adolesc Psychiatry Ment Health 16(1):5
Hauner KK, Zinbarg RE, Revelle W (2014) A latent variable model approach to estimating systematic bias in the oversampling method. Behav Res Methods 46(3):786–797
Williams TC et al (2018) Directed acyclic graphs: a tool for causal studies in paediatrics. Pediatr Res 84(4):487–493
Ohlsson H, Kendler KS (2020) Applying causal inference methods in psychiatric epidemiology: a review. JAMA Psychiat 77(6):637–644
Li P, Stuart EA, Allison DB (2015) Multiple imputation: a flexible tool for handling missing data. JAMA 314(18):1966–1967
Sterne JAC et al (2009) Multiple imputation for missing data in epidemiological and clinical research: potential and pitfalls. BMJ (Clin Res Ed) 338:b2393–b2393
John WG (2009) Missing data analysis: making it work in the real world. Annu Rev Psychol 60(1):549–576
Enders CK (2022) Applied missing data analysis, 2nd edn. The Guilford Press, New York, pp ix, 546–ix, 546
Rothman KJ, Gallacher JEJ, Hatch EE (2013) Why representativeness should be avoided. Int J Epidemiol 42(4):1012–1014
Wolke D et al (2009) Selective drop-out in longitudinal studies and non-biased prediction of behaviour disorders. Br J Psychiatry 195(3):249–256
Saiepour N et al (2019) Does attrition affect estimates of association: a longitudinal study. J Psychiatr Res 110:127–142
Steinhausen H-C et al (2020) Selective attrition does not affect cross-sectional estimates of associations with emotional and behavioral problems in a longitudinal study with onset in adolescence. Psychiatry Res 284:112685
Acknowledgements
We are grateful for all the adolescents and parents who participated in the iBerry Study, the Child and Family Center Rijnmond for their help in the screening procedure, and the whole iBerry team of master students, research assistants, PhD-students, managers, and collaborating clinicians.
ESPRi Consortium
Wim van Beek3, Carla Hagestein-de Bruijn3, Mirjam E.J. Kouijzer4, Alex J.M. de Ridder4, Chi M. van 't Hooft-Nguyen5, Natalie D. Veen5, Philip J. S. Michielsen6, Mark H. de Jong7. 3Parnassia Psychiatric Institute, Rotterdam, The Netherlands; 4GGZ Breburg, Breda, Netherlands; 5GGZ Delfland, Delft, The Netherlands; 6GGZ Westelijk Noord-Brabant, Halsteren, The Netherlands; 7 Yulius Mental Health, Dordrecht, The Netherlands
Funding
The iBerry Study is funded by the ESPRi (Epidemiological and Social Psychiatric Research Institute) consortium that consists of the Erasmus University Medical Center and the mental health care institutes Parnassia Psychiatric Institute Antes, GGz Breburg, GGz Delfand, GGz Westelijk Noord-Brabant, and Yulius.
Author information
Authors and Affiliations
Consortia
Contributions
Conceptualization – all authors; methodology – DB, SRa, NG-vM; formal analysis – DB, MZ, SRa; investigation – DB, SRa, NdN-E Resources - WH; data curation – DB, SRa; writing, original draft – DB; writing, review & editing – all authors; visualization – DB; supervision – NG-vM; project administration – DB, SRa, NdN-E, NG-vM; funding acquisition – ESPRi consortium
Corresponding author
Ethics declarations
Conflict of interest
The authors have no competing interests to declare.
Ethical approval
The study has been approved by the Medical Ethics Research Committee of the Erasmus Medical Center, Rotterdam and was conducted in accordance with the guidelines established by the Declaration of Helsinki.
Consent to participate
Written informed consent was obtained from each participating adolescent and the participating parent.
Additional information
Members of ESPRi Consortium are listed in acknowledgements section.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bouter, D.C., Ravensbergen, S.J., de Neve-Enthoven, N.G.M. et al. Five-year follow-up of the iBerry Study: screening in early adolescence to identify those at risk of psychopathology in emerging adulthood. Eur Child Adolesc Psychiatry (2024). https://doi.org/10.1007/s00787-024-02462-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00787-024-02462-2