
Abstract
Purpose
Predicting lymph node metastasis (LNM) in esophageal squamous cell carcinoma (ESCC) is critical for selecting appropriate treatments despite the low accuracy of computed tomography (CT) for detecting LNM. Variation in potential nodal sizes among locations or patients’ clinicopathological background factors may impact the diagnostic quality. This study explored the optimal criteria and diagnostic ability of CT by location.
Methods
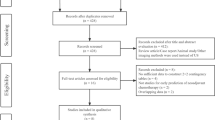
We retrospectively reviewed preoperative CT scans of 229 patients undergoing curative esophagectomy. We classified nodal stations into six groups: Cervical (C), Right-upper mediastinal (UR), Left-upper mediastinal (UL), Middle mediastinal (M), Lower mediastinal (L), and Abdominal (A). We then measured the short-axial diameter (SAD) of the largest lymph node in each area. We used receiver operating characteristics analyses to evaluate the CT diagnostic ability and determined the cut-off values for the SAD in all groups.
Results
Optimal cut-offs were 6.5 mm (M), 6 mm (C, L, and A), and 5 mm (UR and UL). Diagnostic abilities differed among locations, and UR had the highest sensitivity. A multivariate analysis showed poor differentiation to be an independent risk factor for a false-negative diagnosis (p = 0.044).
Conclusions
Optimal criteria and diagnostic abilities for predicting LNM in ESCC varied among locations, and poor differentiation might contribute to failure to detect LNM.


Similar content being viewed by others


Abbreviations
- ESCC:
-
Esophageal squamous cell cancer
- LNM:
-
Lymph node metastasis
- CT:
-
Computed tomography
- NAC:
-
Neoadjuvant chemotherapy
- LNA:
-
Lymph node area
- SAD:
-
Short-axis diameter
- TME:
-
Transmediastinal esophagectomy
- TTE:
-
Transthoracic esophagectomy
- ROC:
-
Receiver operating characteristics
- AUC:
-
Area under the curve
- PPV:
-
Positive predictive value
- Y statistic:
-
Youden’s J statistic
- pdESCC:
-
Poorly differentiated esophageal squamous cell cancer
- EUS:
-
Endoscopic ultrasound
- FDG-PET:
-
8F-fluorodeoxyglucose positron emission tomography
References
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424.
van Rijswijk AS, Hagens ERC, van der Peet DL, van Berge Henegouwen MI, Gisbertz SS. Differences in esophageal cancer surgery in terms of surgical approach and extent of lymphadenectomy: findings of an international survey. Ann Surg Oncol. 2019;26(7):2063–72.
Akutsu Y, Matsubara H. The significance of lymph node status as a prognostic factor for esophageal cancer. Surg Today. 2019;41(9):1190–5.
Sgourakis G, Gockel I, Lyros O, Hansen T, Mildenberger P, Lang H. Detection of lymph node metastases in esophageal cancer. Expert Rev Anticancer Ther. 2011;11(4):601–12.
Liu J, Wang Z, Shao H, Qu D, Liu J, Yao L. Improving CT detection sensitivity for nodal metastases in oesophageal cancer with combination of smaller size and lymph node axial ratio. Eur Radiol. 2008;28(1):188–95.
Sugawara K, Yamashita H, Uemura Y, Yagi K, Nishida M, Aikou S, et al. Preoperative lymph node status on computed tomography influences the survival of pT1b, T2 and T3 esophageal squamous cell carcinoma. Surg Today. 2019;49(5):378–86.
Choi J, Kim SG, Kim JS, Jung HC, Song IS. Comparison of endoscopic ultrasonography (EUS), positron emission tomography (PET), and computed tomography (CT) in the preoperative locoregional staging of resectable esophageal cancer. Surg Endosc. 2010;24(6):1380–6.
Schmidt AF Jr, Rodrigues OR, Matheus RS, Kim Jdu U, Jatene FB. Mediastinal lymph node distribution, size and number: definitions based on an anatomical study. J Bras Pneumol. 2007;33(2):134–40.
Li H, Zhang Y, Cai H, Xiang J. Pattern of lymph node metastases in patients with squamous cell carcinoma of the thoracic esophagus who underwent three-field lymphadenectomy. Eur Surg Res. 2007;39(1):1–6.
Duan XF, Tang P, Shang XB, Jiang HJ, Yu ZT. The prevalence of lymph node metastasis for pathological T1 esophageal cancer: a retrospective study of 143 cases. Surg Oncol. 2018;27(1):1–6.
Zhang J, Liu Y, Che F, Luo Y, Huang W, Heng X, et al. Pattern of lymph node metastasis in thoracic esophageal squamous cell carcinoma with poor differentiation. Mol Clin Oncol. 2018;8(6):760–6.
Rice TW, Ishwaran H, Hofstetter WL, Schipper PH, Kesler KA, Law S, et al. Esophageal cancer: associations with (pN+) lymph node metastases. Ann Surg. 2017;265(1):122–9.
Rice TW, Patil DT, Blackstone EH. 8th edition AJCC/UICC staging of cancers of the esophagus and esophagogastric junction: application to clinical practice. Ann Cardiothorac Surg. 2017;6(2):119–30.
Kitagawa Y, Uno T, Oyama T, Kato K, Kato H, Kawakubo H, et al. Esophageal cancer practice guidelines 2017 edited by the Japan Esophageal Society. Esophagus. 2019;16(1):1–43.
Wang Z, Mao Y, Gao S, Li Y, Tan L, Daiko H, et al. Lymph node dissection and recurrent laryngeal nerve protection in minimally invasive esophagectomy. Ann N Y Acad Sci. 2020;1481(1):20–9.
Mori K, Yamagata Y, Aikou S, Nishida M, Kiyokawa T, Yagi K, et al. Short-term outcomes of robotic radical esophagectomy for esophageal cancer by a nontransthoracic approach compared with conventional transthoracic surgery. Dis Esophagus. 2016;29(5):429–34.
Seto Y, Mori K, Aikou S. Robotic surgery for esophageal cancer: merits and demerits. Ann Gastroenterol Surg. 2017;1(3):193–8.
Japan Esophageal Society. Japanese classification of esophageal cancer, tenth edition: part I. Esophagus. 2009;6:1–25.
Japan Esophageal Society. Japanese classification of esophageal cancer, 11th edition: part I. Esophagus. 2017;14(1):1–36.
Schisterman EF, Perkins NJ, Liu A, Bondell H. Optimal cut-point and its corresponding Youden Index to discriminate individuals using pooled blood samples. Epidemiology. 2005;16(1):73–81.
Prionas ND, Ray S, Boone JM. Volume assessment accuracy in computed tomography: a phantom study. J Appl Clin Med Phys. 2010;11(2):3037.
Onuma Y, Tsuruta C, Okita K, Hamabe A, Ogura K, Takemasa I, et al. CT reconstruction with thick slices not only underestimates lymph node size but also reduces data reproducibility in colorectal cancer. Acta Radiol. 2021;62(10):1275–82.
Genereux GP, Howie JL. Normal mediastinal lymph node size and number: CT and anatomic study. AJR Am J Roentgenol. 1984;142(6):1095–100.
Glazer GM, Gross BH, Quint LE, Francis IR, Bookstein FL, Orringer MB. Normal mediastinal lymph nodes: number and size according to American Thoracic Society mapping. AJR Am J Roentgenol. 1985;144(2):261–5.
Suwatanapongched T, Gierada DS. CT of thoracic lymph nodes. Part I: anatomy and drainage. Br J Radiol. 2006;79(947):922–8.
Wang H, Li QK, Auster M, Gong G. PET and CT features differentiating infectious/inflammatory from malignant mediastinal lymphadenopathy: a correlated study with endobronchial ultrasound-guided transbronchial needle aspiration. Radiol Infect Dis. 2018;5(1):7–13.
Palmer J, Yang J, Pan T, Court LE. Motion of the esophagus due to cardiac motion. PLoS ONE. 2014. https://doi.org/10.1371/journal.pone.0089126.
Wang SZ, Li JB, Zhang YJ, Li FX, Wang W, Liu TH. Measurement of intrafraction displacement of the mediastinal metastatic lymph nodes of non-small cell lung cancer based on four-dimensional computed tomography (4D-CT) (in Chinese). Zhonghua Zhong Liu Za Zhi. 2012;34(9):679–83.
Vazquez-Sequeiros E, Wiersema MJ, Clain JE, Norton ID, Levy MJ, Romero Y, et al. Impact of lymph node staging on therapy of esophageal carcinoma. Gastroenterology. 2003;125(6):1626–35.
Li L, Liu SY, Zhu KS, Chen JQ, Ying MG. Analysis of lymph node metastases in early esophageal carcinoma and treatment regimens (in Chinese). Zhonghua Zhong Liu Za Zhi. 2009;31(3):226–9.
Kumakura Y, Yokobori T, Yoshida T, Hara K, Sakai M, Sohda M, et al. Elucidation of the anatomical mechanism of nodal skip metastasis in superficial thoracic esophageal squamous cell carcinoma. Ann Surg Oncol. 2018;25(5):1221–8.
Mortensen MB, Fristrup C, Holm FS, Pless T, Durup J, Ainsworth AP, et al. Prospective evaluation of patient tolerability, satisfaction with patient information, and complications in endoscopic ultrasonography. Endoscopy. 2005;37(2):146–53.
Li B, Li B, Jiang H, Yang Y, Zhang X, Su Y, et al. The value of enhanced CT scanning for predicting lymph node metastasis along the right recurrent laryngeal nerve in esophageal squamous cell carcinoma. Ann Transl Med. 2020;8(24):1632.
Karashima R, Watanabe M, Imamura Y, Ida S, Baba Y, Iwagami S, et al. Advantages of FDG-PET/CT over CT alone in the preoperative assessment of lymph node metastasis in patients with esophageal cancer. Surg Today. 2015;45(4):471–7.
Kajiyama Y, Iwanuma Y, Tomita N, et al. Size analysis of lymph node metastasis in esophageal cancer: diameter distribution and assessment of accuracy of preoperative diagnosis. Esophagus. 2006;3:189–95.
Acknowledgements
We thank the past and present members of our department for collecting the data used for this analysis from the early period of the study.
Funding
This research received no specific grants from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Sachiyo Nomura is the recipient of a research grant from JCR Pharmaceuticals Co., Ltd. The other authors have no potential conflicts of interest to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Shiomi, S., Yajima, S., Yoshimura, S. et al. Optimal criteria for predicting lymph node metastasis in esophageal squamous cell carcinoma by anatomical location using preoperative computed tomography: a retrospective cohort study. Surg Today 52, 1185–1193 (2022). https://doi.org/10.1007/s00595-022-02460-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00595-022-02460-4