
Abstract
The aim of the present review is to systematically analyse the current literature about gender differences in hip or knee cartilage composition and degeneration, to help explaining how and why osteoarthritis affects women more often and more severely than men. A systematic review of the literature in English was performed. Eleven studies on 1962 patients (905 females and 787 males) that reported differences on cartilage composition between males and females were included. Nine evaluated the knee, one the hip, and one both. They were heterogeneous in their methods: one conducted histological analyses, and all the others evaluated cartilage characteristics (volume, width, and composition) through magnetic resonance imaging. All authors reported gender differences in both volume and morphology of the cartilage, from infancy to menopause. In fact, a study on 92 healthy children statistically showed significant gender differences in cartilage thickness at all sites, even after adjustment for age, body, and bone size. Gender differences become more evident after menopause, when women have a lower cartilage volume and a higher cartilage loss. Men show significantly higher knee and hip cartilage volumes than women, and women carry a significantly greater risk to develop osteoarthritis. This is in part due to body and bone size, but also depends on qualitative and quantitative differences in the composition of cartilage and its degeneration rate after menopause. Structural changes in cartilage that occur between genders during ageing have significance in the development of osteoarthritis.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The most common musculoskeletal illness, osteoarthritis (OA), affects more than 300 million individuals globally and is a primary cause of disability [1]: 10–15% of all adults over the age of 60 have some type of OA [2]. Despite the scientific community's efforts, the processes underlying the genesis, evolution, and therapy of OA remain unknown. While risk variables such age, genetic profiles, obesity, and traumatic injury [3] have been discovered and established, the role of gender has been undervalued [4, 5]. As a matter of facts, there are sex/gender variations in the frequency, incidence, and severity of OA: women are more affected, particularly following menopause, and often exhibit more severe clinical symptoms [6]. A meta-analysis of nine studies that provide impact sizes for gender on risk variables for the start of knee OA found that females have an odds ratio of 1.84 (95% CI 1.32–2.55) compared to males [7]. An explanation for this difference may lie in the distinct cartilage compositions between men and women, which may predispose female to a sooner joint degradation [8, 9]. Imaging methods like magnetic resonance imaging (MRI) allow for non-invasive evaluation of cartilage composition, loss of collagen matrix and proteoglycans and water content variation [10, 11].
The purpose of this study is to conduct a systematic review of the available studies on gender differences in hip or knee cartilage composition and degeneration. In fact, a study that lays the foundation for the different clinical manifestations of OA in men and women is lacking to date. This study could help to understand the structural phenomena (quantitative and qualitative change of the cartilage) underlying the different clinical manifestations of OA between men and women. Knowing the changes in cartilage structure could also be helpful in laying the foundation in the prevention of joint arthrosis and developing successful tailored diagnostic and treatment solutions.
Materials and methods
Search strategy
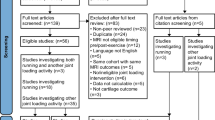
In April 2023, a comprehensive evaluation of the existing English literature was conducted using three big databases (Scopus, Embase, and PubMed). The strings MeSH terms utilized were a combination of the following keywords: “hip”, “knee”, “cartilage characteristics”, “gender”, “sex”, “cartilage composition”, “differences”, “osteoarthritis”. Two authors independently screened all potentially relevant titles and abstracts, and any disagreement was solved by the senior authors. During the development of this review, the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines were followed [12] (Fig. 1).

PRISMA algorithm: search strategy according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement
Two authors independently assessed the quality of included trials using the NIH tool [13]. Two of the authors retrieved reference data, populations, and outcomes from the papers into pre-specified tables with Excel (Microsoft®). The authors extracted data on the basic features of the studies (including the design and primary outcomes), participants (population and sample size), treatments (diagnostic modality of cartilage composition), comparator (if applicable), and summary of major results. An attempt was made to compare qualitative and quantitative differences in articular cartilage of the knee and of the hip between male and female with the methods used in individual studies.
Eligibility criteria
For the current study, the PICOS model (Population, Intervention, Comparison, Outcomes, Study design) was used: studies that considered healthy subjects and/or patients with hip or knee osteoarthritis (Population), submitted or did not submit to a specific surgical intervention (Intervention), with or without a comparison group of healthy controls (Comparison), reported differences in cartilage composition between males and females (Outcomes), in clinical studies (Study design).
There were no publishing year restrictions. Only articles in English were considered. The search was limited to human data. Reviews, case reports, case series, and in vitro or in vivo studies were eliminated; randomized controlled trials (RCTs), retrospective or prospective observational studies that satisfied the indicated PICOS were included.
Results
Baseline characteristics
The search for relevant publications retrieved 587 studies. These references were entered into a reference manager (Mendeley 1.14) and duplicates (n = 152) were eliminated. The remaining 435 records were examined for title, abstract, and full text. In the end, 11 papers were selected for synthesis (Fig. 1). The key aspects of these investigation are extracted and summarized in Table 1. There were eight cross-sectional studies (CSS) [14,15,16,17,18,19,20,21], two prospective studies (PS) [22, 23], and one longitudinal cohort study (LCS) [24] among the 11 publications chosen. They studied 1692 patients, 905 females and 787 males. According to the NIH tool, all the studies were of high quality (Table 2).
Different procedures were used in the studies examined. In terms of cartilage evaluation, only one author performed histological studies [14]. The other studies [15,16,17,18,19,20,21,22,23,24] assessed its composition (volume, length, width, T1/T2 values) through MRI. Nine studies looked at the knee [15,16,17,18,19,20,21, 23, 24], one at the hip [22], and one at both joints [14]. Table 3 presents a summary of the main results obtained from the various studies.
Knee cartilage morphometry
Most of the included research discussed how gender differed in terms of knee morphometry [15,16,17,18,19,20,21, 23, 24]. They all used MRIs to assess quality and quantity of cartilage. The findings of each author demonstrated the existing disparities in gender anatomy. All studies agree on the better quality and greater quantity of cartilage in men than in women, except the work of Tameem et al.
Jones et al. [17] (2000) proposed the possibility that differences in cartilage formation might explain sex-related and joint compartment-related differences in the risk of osteoarthritis (OA) in the knee. They examined 92 kids randomly to measure the thickness and volume of articular cartilage. Compared to females, males had noticeably more knee cartilage. The variance in cartilage thickness and volume was statistically significant at all locations and was explained by gender in 6–36% of cases [17]. These disparities persisted even after controlling for bone density, age, BMI, physical activity, and bone area [17].
Also, Faber et al. [18] noticed gender variabilities in cartilage thickness and volumes when eighteen healthy participants, nine males and nine females, without local or systemic joint illness underwent MRIs to quantify the articular surface area, cartilage thickness, and cartilage volume. Women presented 19.9% smaller cartilage of the patella and 46.6% smaller cartilage of the medial tibia compared to men. Even though these differences were less pronounced when body weight and BMI were considered [18].
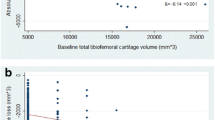
Attempting to characterize the relationship between gender, BMI, age, bone size, and cartilage degeneration rate, Ding et al. [19, 24] conducted two studies, in 2003 and 2007, that showed a significantly higher (33–42%) knee cartilage volume in men than women [19], and that the rate of cartilage deterioration in women was much greater than in males after 40 years old (medial tibia − 3.5%, lateral tibia − 2.6% and patella − 0.8% of cartilage loss per year) [24].
An average atlas of the morphology of the femoral knee cartilage was produced by Tameem et al. [15]. After adjusting for joint surface area, they found that women's cartilage was thicker (average Jacobian, a voxel-based measure of the volume that provides information on the localized volume changes) at 1.2 ± 0.078 versus 1.08 ± 0.097 [15]. The cartilage of each subject was initially normalized to the atlas for the overall size: therefore, if the cartilage scaled nonlinearly with body size, a linear global correction resulted in a bigger cartilage volume [15].
In 2014, Pachowsky et al. [23] observed that there were gender disparities in both post-matrix-associated autologous chondrocyte transplantation (MACT) zones and healthy cartilage. They also found worse quality cartilage in female with less healing capacity than male. In fact, T2 values with the MRI were significantly shorter in men than women.
Using 3 T MRI, Kumar et al. [16] quantitatively analysed the knee cartilage of three patient cohorts: young active, middle-aged without OA, and middle-aged with OA. Their findings indicated that women had higher levels of lateral articular and patellofemoral cartilage on T1ρ (or T1rho, used for quantitative cartilage mapping due to its sensitivity to the proteoglycans of the cartilage extracellular matrix), which indicate a lower proteoglycan content and lower tissue quality.
Moreover, Berman et al. [20] discovered gender-based morphological variations in the architecture of femoral condyles, even in patients with the same height. A stratified study of patient height and medial/lateral condylar width revealed a significant difference in condylar widths for each stratum. They also observed a statistically significant difference in articular cartilage width between males and females (31.62 ± 3.54 for males and 26.53 ± 3.70) [20].
Anthony et al. [21] examined the quantity of tibial cartilage in a group of young Australians. Men's tibial cartilage volume was found to be 13% bigger than women's [21]. Nevertheless, after adjusting for fibrinogen, fat mass, and lean body mass, the strength of this correlation declined [21].
Hip cartilage morphometry
The work for the hip cartilage evaluation demonstrated a better quality of the cartilage of men compared to women. Nemeth et al. [22] evaluated hip cartilage by analysing thirty asymptomatic participants' right hip MRIs. The average T1ρ value was greater in women than in males (5.98 ms higher in women compared to men). Age, BMI, and the level of sports activity did not significantly affect the mean T1ρ value [22]. Additionally, women's T1ρ value standard deviations were larger than men's.
Histological analysis
Histological quality of cartilage appears worse in women than in men. The osteoarthritic cartilage was histologically analysed only by Kaspiris et al. [14]. The study examined the frequency of cracks over the course of OA and tried to relate them to underlying cellular alterations. Three patient groups were analysed, one with knee OA, one with hip OA, and a control group of unaffected population. They categorized each group for the disease severity. Patients with moderate to severe OA exhibited a higher frequency of cartilage cracks, but those with severe OA showed them in the subchondral bone [14]. Moreover, those with a more severe histology grade had a larger frequency of cracks in the hip OA patient group. Lastly, they noticed that females often had more cartilage cracks [14].
Discussion
Aim of the present article was to review and summarize the current literature about gender differences in hip or knee cartilage composition, and the potential implications of these differences on joint degeneration in diagnosis and therapy of osteoarthritis. Our results show that men have a significantly higher cartilage volume than women, who are more likely to develop osteoarthritis.
These results should be read in the context of their limitations. These mainly stem from the difficulty of finding manuscripts specifically focused on exploring gender-related differences, where the primary purpose and key outcome measures are explicitly stated. Most clinical research relies on standard methodologies that incorporate sex-adjusted analyses and consider gender as a confounding variable. The diverse range of studies included and their limited degree of evidence pose an additional challenge, significantly limiting the interpretability of our results.
One known risk factor for osteoarthritis (OA) is female gender: women older than 50 years of age are more likely to develop OA in the hands, hips, or knees, and it is often found to be at a more advanced stage already at clinical onset [25, 26]. The reasons behind this evidence are still unclear. Understanding the fundamental processes underlying gender-related variations and the role that gender differences play in the development of osteoarthritis (OA) would be crucial from an epidemiological, diagnostical, and treatment perspective. Indeed, identifying gender-based disparities would result in ad hoc diagnostic procedures, and customized treatment for men and women [6].
Our results showed considerable variability in the outcomes assessed by examining changes in cartilage width and structure. While no histological analysis was performed in any of the included investigations to search for variations in cartilage composition, imaging studies were used to indirectly illustrate these variations. MRI was primarily used to assess the volume, thickness, and composition of cartilage [15,16,17,18,19,20,21, 23, 24]; both qualitative and quantitative variations were documented. Males were often shown to have higher hip and knee cartilage volumes than females, even after adjustment for height and body weight [16, 18, 19]. According to Faber et al. [18], rather than the cartilage's thickness, the variation in cartilage volume among individuals with healthy knees is mostly caused by a difference in joint size. However, the study was unable to relate this discrepancy to the inter-individual anthropometric variabilities [18]. Another study conducted by Ding and colleagues assessed that the disparity in volume between genders can only be partially attributed to differences in body mass and bone size, and in any case, it is not impacted by the level of physical activity [19, 24].
Different studies [15, 16, 19] assessed that female’s cartilage has an higher T1ρ on MRI, which is indicative of inferior quality due to a lower proteoglycan concentration.
According to Kumar and colleagues [16], the variation in volume may be ascribed to the articular cartilage's composition as well as a distinct walking alignment mechanism. The analysis of the morphological atlas of the distal femur's articular cartilage conducted by Tameen et al. [15] revealed different load points between men and women, especially in the medial weight-bearing region and the trochlear femoral side of the patellofemoral compartment. These differences could be interpreted as a risk factor for the development of OA.
The single study on hip cartilage was carried out in 2017 by Nemeth et al. [22]. Based on MRI cartilage quantitative evaluation, they confirmed the results of other studies on knee joints [16,17,18, 23], founding a gender difference of 10% higher in females T1ρ values.
After the age of 50, the observed gender variations in cartilage composition become more noticeable, thus indicating a possible connection between the development of cartilage width and quality during growth and the subsequent loss of cartilage throughout adulthood [24].
In terms of cartilage development, Jones et al. [17] conducted an interesting study on healthy children. The analysis of the knees’ cartilage thickness and volume showed gender-related differences from an early age. Males had significantly more knee cartilage than females in terms of both thickness and volume [17].
Regarding cartilage loss, females have higher annual rates of change in knee cartilage volume compared to men [24]. It is hypothesized that the drastic reduction in oestrogen levels in postmenopausal women triggers and initiates OA [27, 28]. Ding et al. [24] showed that women start the cartilage loss around the age of 40, with a notable escalation after menopause, as anticipated [19]. So, many studies found that sex differences vary with age and become greater in females > 55: the reasons for this age specificity are largely unknown but may reflect the effect of oestrogen deficiency in earlier life and of menopause in later life. Our speculation is that, although oestrogen may have a modulating effect on cartilage, the effects of sex hormones and growth factors in mediating such and age-sex interaction in OA risk are still poorly understood and need further investigation.
Furthermore, women undergoing hormone replacement therapy demonstrated a diminished rate of cartilage degeneration [29]. This raises the possibility of preventative measures for women in the onset of OA. However, hormonal fluctuations are not the sole cause of cartilage loss, and the reason behind this cartilage disparity between females and males remains unknown and needs to be studied.
In the authors’ opinion, this article shows how deeply gender differences may affect both medicine and surgery; some authors, considering the morphological and biomechanical differences between men and women, utilize gender-specific customized prosthetic implants with very good outcome [30, 31]. This suggests how medicine is moving towards an increasingly deeper understanding of the biological mechanisms underlying pathologies, aiming to prevent them where possible, or, when prevention is not possible, to treat them in the most personalized manner.
Conclusions
Men exhibit significantly higher knee and hip cartilage volumes than women. Thus, women are significantly more likely than men to develop osteoarthritis, especially with ageing. These differences seem to be only partially influenced by body and bone size, suggesting the need for further research in this area. Moreover, these gender disparities become more pronounced after the age of fifty, indicating that gender-related variations in cartilage volume throughout adulthood are shaped by both cartilage loss and development during childhood and adolescence. Currently, in the age of precision medicine, there are no gender-specific procedures available to address and compare the progression of end-stage osteoarthritis.
References
World Health Organization (2022) Muscoloskeletal health. https://www.who.int/news-room/fact-sheets/detail/musculoskeletal-conditions. Accessed May 2023
Kolasinski SL, Neogi T, Hochberg MC, Oatis C, Guyatt G, Block J, Callahan L, Copenhaver C, Dodge C et al (2019) American college of rheumatology/arthritis foundation guideline for the management of osteoarthritis of the hand, hip, and knee. Arthritis Rheumatol 72(2):220–233. https://doi.org/10.1002/art.41142
Martel-Pelletier J (2004) Pathophysiology of osteoarthritis. Osteoarthr Cartil 12(Suppl A):S31–S33. https://doi.org/10.1016/j.joca.2003.10.002
Maleki-Fischbach M, Jordan JM (2010) New developments in osteoarthritis Sex differences in magnetic resonance imaging-based biomarkers and in those of joint metabolism. Arthritis Res Ther 12(4):212. https://doi.org/10.1186/ar3091
Sowers M (2001) Epidemiology of risk factors for osteoarthritis: systemic factors. Curr Opin Rheumatol 13(5):447–451. https://doi.org/10.1097/00002281-200109000-00018
O’Connor MI (2007) Sex differences in osteoarthritis of the hip and knee. J Am Acad Orthop Surg 15(Suppl 1):S22–S25
Blagojevic M, Jinks C, Jeffery A, Jordan KP (2010) Risk factors for onset of osteoarthritis of the knee in older adults: a systematic review and meta-analysis. Osteoarthr Cartil 18(1):24–33. https://doi.org/10.1016/j.joca.2009.08.010
Pearle AD, Warren RF, Rodeo SA (2005) Basic science of articular cartilage and osteoarthritis. Clin Sports Med 24(1):1–12. https://doi.org/10.1016/j.csm.2004.08.007
Sims EL, Carland JM, Keefe FJ, Kraus VB, Guilak F, Schmitt D (2009) Sex differences in biomechanics associated with knee osteoarthritis. J Women Aging 21(3):159–170. https://doi.org/10.1080/08952840903054856
Rauscher I, Stahl R, Cheng J, Li X, Huber MB, Luke A et al (2008) Meniscal measurements of T1rho and T2 at MR imaging in healthy subjects and patients with osteoarthritis. Radiology 249(2):591–600. https://doi.org/10.1148/radiol.2492071870
Regatte RR, Akella SV, Lonner JH, Kneeland JB, Reddy R (2006) T1rho relaxation mapping in human osteoarthritis (OA) cartilage: comparison of T1rho with T2. J Magn Reson Imaging 23(4):547–553. https://doi.org/10.1002/jmri.20536
Moher D, Altman DG, Liberati A, Tetzlaff J (2011) PRISMA statement. Epidemiology 22(1):128. https://doi.org/10.1097/EDE.0b013e3181fe7825
National Heart, Lung, and Blood Institute (2021) Studi Quality Assessment Tools. https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools. Accessed May 30, 2023
Kaspiris A, Chronopoulos E, Vasiliadis E, Khaldi L, Melissaridou D, Iliopoulos ID et al (2022) Sex, but not age and bone mass index positively impact on the development of osteochondral micro-defects and the accompanying cellular alterations during osteoarthritis progression. Chronic Dis Transl Med 8(1):41–50. https://doi.org/10.1002/cdt3.16
Tameem HZ, Ardekani S, Seeger L, Thompson P, Sinha US (2011) Initial results on development and application of statistical atlas of femoral cartilage in osteoarthritis to determine sex differences in structure: data from the Osteoarthritis Initiative. J Magn Reson Imaging 34(2):372–383. https://doi.org/10.1002/jmri.22643
Kumar D, Souza RB, Subburaj K, MacLeod TD, Singh J, Calixto NE et al (2015) Are there sex differences in knee cartilage composition and walking mechanics in healthy and osteoarthritis populations? Clin Orthop Relat Res 473(8):2548–2558. https://doi.org/10.1007/s11999-015-4212-2.PMID:25716211;PMCID:PMC4488198
Jones G, Glisson M, Hynes K, Cicuttini F (2000) Sex and site differences in cartilage development: a possible explanation for variations in knee osteoarthritis in later life. Arthritis Rheum 43(11):2543–2549
Faber SC, Eckstein F, Lukasz S, Mühlbauer R, Hohe J, Englmeier KH et al (2001) Gender differences in knee joint cartilage thickness, volume and articular surface areas: assessment with quantitative three-dimensional MR imaging. Skeletal Radiol 30(3):144–150. https://doi.org/10.1007/s002560000320
Ding C, Cicuttini F, Scott F, Glisson M, Jones G (2003) Sex differences in knee cartilage volume in adults: role of body and bone size, age and physical activity. Rheumatology (Oxford) 42(11):1317–1323. https://doi.org/10.1093/rheumatology/keg374
Berman D, Rogers K, Griffin J, Bonner K (2019) Gender disparity between absolute versus relative size of condylar chondral defects: an MRI analysis. J Knee Surg 32(5):448–453. https://doi.org/10.1055/s-0038-1646932
Antony B, Venn A, Cicuttini F, March L, Blizzard L, Dwyer T et al (2016) Association of body composition and hormonal and inflammatory factors with tibial cartilage volume and sex difference in cartilage volume in young adults. Arthritis Care Res (Hoboken) 68(4):517–525. https://doi.org/10.1002/acr.22715
Nemeth A, Di Marco L, Boutitie F, Sdika M, Grenier D, Rabilloud M et al (2018) Reproducibility of in vivo magnetic resonance imaging T1 rho and T2 relaxation time measurements of hip cartilage at 3.0T in healthy volunteers. J Magn Reson Imaging 47(4):1022–1033
Pachowsky ML, Werner S, Marlovits S, Stelzeneder D, Renner N, Trattnig S et al (2014) 3D-isotropic high-resolution morphological imaging and quantitative T2 mapping as biomarkers for gender related differences after matrix-associated autologous chondrocyte transplantation (MACT). J Orthop Res 32(10):1341–1348. https://doi.org/10.1002/jor.22682
Ding C, Cicuttini F, Blizzard L, Scott F, Jones G (2007) A longitudinal study of the effect of sex and age on rate of change in knee cartilage volume in adults. Rheumatology (Oxford) 46(2):273–279. https://doi.org/10.1093/rheumatology/kel243
Phinyomark A, Osis ST, Hettinga BA, Kobsar D, Ferber R (2016) Gender differences in gait kinematics for patients with knee osteoarthritis. BMC Musculoskelet Disord 12(17):157. https://doi.org/10.1186/s12891-016-1013-z
Jordan JM, Helmick CG, Renner JB, Luta G, Dragomir AD, Woodard J et al (2007) Prevalence of knee symptoms and radiographic and symptomatic knee osteoarthritis in African Americans and Caucasians: the Johnston county osteoarthritis project. J Rheumatol 34(1):172–180
Hardcastle SA, Dieppe P, Gregson CL, Davey Smith G, Tobias JH (2015) Osteoarthritis and bone mineral density: are strong bones bad for joints? Bonekey Rep 21(4):624. https://doi.org/10.1038/bonekey.2014.119
Burr DB, Gallant MA (2012) Bone remodelling in osteoarthritis. Nat Rev Rheumatol 8(11):665–673. https://doi.org/10.1038/nrrheum.2012.130
Wluka AE, Davis SR, Bailey M, Stuckey SL, Cicuttini FM (2001) Users of oestrogen replacement therapy have more knee cartilage than non-users. Ann Rheum Dis 60(4):332–336. https://doi.org/10.1136/ard.60.4.332
Xie X, Lin L, Zhu B, Lu Y, Lin Z, Li Q (2014) Will gender-specific total knee arthroplasty be a better choice for women? A systematic review and meta-analysis. Eur J Orthop Surg Traumatol 24(8):1341–1349. https://doi.org/10.1007/s00590-013-1396-6
Jain R, Kalia RB, Das L (2019) Anthropometric measurements of patella and its clinical implications. Eur J Orthop Surg Traumatol 29(8):1765–1769. https://doi.org/10.1007/s00590-019-02490-8
Funding
Open access funding provided by Alma Mater Studiorum - Università di Bologna within the CRUI-CARE Agreement. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
ADM contributed to conception and design; drafting—writing and editing; and critical revision; FB contributed to conception and design; data analysis and interpretation; and drafting—reviewing. CDA contributed to data analysis and interpretation and drafting—writing and editing. VC contributed to collection and assembly of data; quality assessment; and drafting—writing. TC contributed to collection and assembly of data. PM and FT contributed to data analysis and interpretation and critical revision. AR contributed to data analysis and interpretation; drafting—reviewing and editing. CF contributed to critical revision of the article for important intellectual content and final approval.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest.
Protocol registration
PROSPERO does not accept scoping reviews, literature reviews or mapping reviews. For these reasons our review and its protocol are not registered.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Di Martino, A., Barile, F., D’Agostino, C. et al. Are there gender-specific differences in hip and knee cartilage composition and degeneration? A systematic literature review. Eur J Orthop Surg Traumatol 34, 1901–1910 (2024). https://doi.org/10.1007/s00590-024-03871-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00590-024-03871-4