
Abstract
Purpose
Conservative approaches such as Schroth exercises and core stabilization exercises showed effective results in the treatment of idiopathic scoliosis. This study aimed to critically evaluate the magnitude effect of Schroth and core stabilization exercises using a systematic review and meta-analysis.
Methods
This study has been developed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement. The following three databases were searched for articles collection: Web of Science, PubMed, and Google Scholar. The key search terms were: Schroth exercise, core exercise, idiopathic scoliosis, Cobb angle, angle of trunk rotation, and quality of life. The articles included in our study was limited to original articles written only in English that met the following inclusion criteria: (1) Participants with idiopathic scoliosis; (2) Schroth exercises and core stabilization exercises used as interventions; (3) Cobb angle or angle of trunk rotation or quality of life used as outcome measures.
Results
Thirteen studies were included. Depending on the outcome measured, the magnitude effect of Schroth and core stabilization exercises ranged from small to almost large as follows: Cobb angle (SMD = – 0.376, p ˂ 0.001); angle of trunk rotation (SMD = – 0.268, p = 0.104); quality of life (SMD = 0.774, p = 0.002). By subgroup analysis, Schroth method showed a larger effect size than core stabilization exercises.
Conclusion
The current systematic review and meta-analysis indicates that both Schroth method and core stabilization exercises have a positive effect in subjects with idiopathic scoliosis. Subgroup analysis showed that the Schroth method had a larger effect size than the core stabilization exercises.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Idiopathic scoliosis (IS) is a rare three-dimensional deformity of the spine that occurs in children without a known cause [1]. It can occur in different periods of childhood and adolescence characterized as periods of growth spurt. The first of these periods is between 6 and 24 months, then between 5 and 8 years, and finally between 11 and 14 years [2].
In about 20% of cases, scoliosis is secondary to another pathology, while for 80% it is idiopathic and is more frequent in female than male children [2].
IS can negatively affect physical and psychosocial health and can limit normal life functioning [1, 3]. Prevention of scoliosis is achieved through regular medical checkups, educational conversations about posture, sports practice, constant attendance of physical education classes, and the use of protective positions [4].
For scoliosis treatment can be distinguished conservative and non-conservative approaches. Non-conservative treatments usually include spine surgery and are not without risks [5]. Conservative treatments include physical therapy, physical exercise, and wearing a brace. The choice of treatment to be adopted depends on the severity of the scoliotic curve [1]. The International Society on Scoliosis Orthopaedic and Rehabilitation Treatment (SOSORT) was launched in Europe in 2004 to meet the need for the most effective treatment of subjects with scoliosis [6]. According to the most recent SOSORT guidelines, the general goals of conservative treatment of scoliosis include stopping or reducing the progression of the curve, reducing or treating respiratory dysfunctions, reducing or treating spinal pain syndromes, and improving the subject's aesthetics by correcting posture [2]. These goals ultimately prevent the need for surgery [2, 7, 8].
Among the conservative treatments, there are several approaches of physical therapy and physical exercise such as the Schroth method, and more recently, the core stabilization exercises [1, 4, 9].
The Schroth method is a three-dimensional program of exercises developed in Germany in the 1920s by Katharina Schroth [10]. Further progress of the method was made by her daughter, Christa Lehnert-Schroth [4]. This treatment is an individualized program, and it is based on kinesthetic and sensorimotor principles including postural corrective exercises, postural self-corrective exercises, and postural home-exercises and it is conducted through a mirror and adopting the exercises repetition [11]. The method uses rotational breathing techniques, i.e., exercises in which respiratory thoracic movements are performed toward the opposite side of the trunk torsion to reduce it, and a combination of stretching and strengthening exercises, based on the muscle groups imbalance [5, 10, 12].
Core stabilization is an exercise approach involving trunk muscles, i.e., the musculature of the spine, pelvis, and abdomen regions, recently used in order to improve body balance and reduce postural asymmetries [13, 14]. Indeed, core stabilization exercises recruit spinal stabilizer muscles, which improve the ability to straighten the spine [9]. The core muscles limit the forces of compression, distortion, and rotation of the spine [15]. Although core stabilization exercises would appear to be effective to increase muscle strength of the lumbar region and improve neuromuscular imbalance, which represent the causes of IS, few studies have investigated the beneficial effects of core stabilization exercises in subjects with IS [16].
Before and during of any treatment are performed different scoliosis measurements such as radiography of the spine and scoliometry. In order to monitor the status of IS during its treatment, the most commonly used parameter is the Cobb angle which is measured by radiographs in standing position [17, 18]. Among the other parameters, the angle of trunk rotation (ATR) is a measure of trunk deformity, and it is evaluated through a scoliometer [19].
The aim of this systematic review and meta-analysis is to examine the overall effect of Schroth and core stabilization exercises in subjects with IS, and also, if possible, to compare the mutual magnitudes of the effect to assess which of these treatments is better. The overall magnitude of the effect, using these two methods, was analyzed by meta-analysis, to find out whether there was a reduction in Cobb angle and in ATR and moreover, an improvement in quality of life (QoL) in subjects with IS.
Methods
Study design
This study has been developed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement [20].
Data sources and search strategy
The databases searched to identify all relevant studies were Web of Science, PubMed, and Google Scholar databases. The search strategy included the combinations of subject titles “Schroth exercise”, “core exercise”, “idiopathic scoliosis”, “Cobb angle”, “angle of trunk rotation”, and “quality of life”.
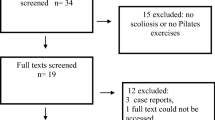
The search strategy is shown in Fig. 1. We also manually searched citations of identified critiques and selected original articles to download the full-text.

Flow diagram of the process of study selection
Study selection
PICOS (Population, Interventions, Comparators, Outcomes, Study Designs) eligibility criteria described in PRISMA were adopted for inclusion/exclusion of the studies [20]. To be included in our study, the articles had to meet the following inclusion criteria: (1) Participants with idiopathic scoliosis; (2) Schroth exercises and core stabilization exercises used as interventions; and (3) Cobb angle or angle of trunk rotation (ATR) or quality of life (QoL) used as the outcome measures. The inclusion of articles in our study was limited to original articles written only in English. The inclusion/exclusion of studies was carried out by two investigators by consultation and consensus.
Data extraction and quality assessment
After selecting studies based on the inclusion and exclusion criteria, two investigators independently conducted data extraction. The following information was extracted and inserted into a pre-formatted table: authors, year of publication, type of exercise program, characteristics of the sample (number of participants, age), outcomes, Cobb angle size, exercise time per day, duration of the exercise program, and whether the studies had a control group. All studies included had data available.
The categorization of the studies was assessed using the National Health and Medical Research Council (NHMRC) hierarchy of records [21].
Two investigators independently assessed the quality of the studies involved. Risk of bias was assessed for each study using the Cochrane Risk of Bias Tool (Fig. 2), which included seven sources of bias, including randomization process, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, missing outcome data, selective outcome reporting, and other potential bias [22]. Each study was examined based on the above seven aspects and subsequently assessed as at low risk of bias, high risk of bias, or unclear risk.

Risk of bias graph: review authors' judgments about each risk of bias item
Data synthesis and analysis
Meta-analysis and statistical analysis were performed using Meta-Analyst software (Brown University). For all outcomes measured by at least two studies, the magnitude of the effect was estimated. For each study, standardized mean difference (SMD) and 95% confidence interval (CI) were calculated for continuous outcomes with a random model. For Cobb angle, ATR, and QoL, the overall effect size for the Schroth method and for the core stabilization exercises was measured post- minus pre-intervention in the experimental and control groups. According to the Cohen’s guide, values of ≥ 0.2, ≥ 0.5, and ≥ 0.8 show small, medium, and large effect sizes, respectively [23]. After that, the analysis of subgroups for Cobb angle, ATR, and QoL outcomes was performed in order to separately assess the size of the effect and to solve the presence of increased heterogeneity. We also calculated the magnitude of the effect only in the experimental group (Schroth and core group), as post- minus pre-intervention. Statistical significance was set at p < 0.05. Heterogeneity between studies was assessed using the Higgins I2 test and p values. For the meta-analysis, the interpretation of heterogeneity across randomized trials was as follows: from 0 to 40%: might not be important; from 30 to 60%: may represent moderate heterogeneity; from 50 to 90%: may represent substantial heterogeneity; from 75 to 100%: considerable heterogeneity.
Results
Study selection and characteristics
Based on the search strategy, a total of 216 studies were selected from the initial database search. After the removal of 69 studies, 147 studies were selected for further analysis. After screening of titles and abstracts, 110 studies were excluded since they did not meet the inclusion criteria. The remaining 37 studies were completely reviewed. After the review of the full-text articles, 24 studies were excluded. The remaining 13 studies, shown in Table 1, were included in this review. The flowchart of the study selection process is shown in Fig. 1.
Table 1 shows the main characteristics of the included studies. A total of 412 subjects with scoliosis participated in the thirteen included studies. The sample size of the included studies ranged from 15 to 51, including 137 subjects in the Schroth method and 123 subjects in the core stabilization exercises. Schreiber [16, 24] used the same cohort reporting different outcomes in the two studies [3, 24]. The age of the respondents ranged between 10 and 23 years. The duration of the daily treatment ranged from 50 min up to 120 min. The total duration of the treatment ranged from 6 weeks to 6 months. As comparators, groups without treatment were used, standard of care of subjects who attended only initial and final measurements, Pilates exercises, respiratory muscle exercises performed using SpiroTiger, traditional rehabilitation which included breathing exercises, spine flexibility exercises, stretching exercises for muscles involved (especially for concave sides of the curve), and general strengthening exercises for the main muscle groups of the torso, pelvis, and shoulder girdle muscles (especially on the convex sides curve), manual massage, scientific exercises approach to scoliosis (SEAS), brace, and some studies have used Schroth exercises and core stabilization exercises in the control groups (Table 1).
Of the 13 included studies, according to the National Health and Medical Research Council (NHMRC) hierarchy of evidence [21], the study of Ko and Kang [16] was assessed as level III, while the other studies were assessed as level II.
Risk of bias
Figures 2 and 3 present the summary of the risk of bias for each included study. For the item of random sequence generation, twelve studies were randomized controlled trials, while one study did not report information regarding the randomization process [16] as shown in Risk of bias (Fig. 3). The item concerning the allocation concealment to the group was unclear in one study [18]. Because of the nature of the intervention, participants and investigators could not be blinded to the treatment, but one study reports that it used blinding [9]. For outcome blinding, four studies adopted a single-blind method to evaluate the intervention measures [3, 24,25,26]. All studies had low risk in incomplete outcome data. One study had unclear risk in selective reporting, while 12 studies had low risk. Because of objective outcome measures, outcome data were considered at low risk in 12 studies [27].

Risk of bias for each study. Legend. Yellow, unclear risk; green, low risk
Meta-analysis
Cobb angle
A total of 11 studies measured the outcome of Cobb angle [3, 9, 15, 16, 18, 25,26,27,28,29,30]: 6 studies using the Schroth method and 5 studies using the core stabilization exercises. After data pooling, SMD between post- and pre-intervention (Schroth or core stabilization) in the experimental group and the control group, statistical significance was reached: SMD = – 0.376; 95% CI = – 0.565, – 0.187, p ˂ 0.001; heterogeneity (I2 = 0%, p = 0.823) (Fig. 4). Subsequently, a subgroup analysis for Cobb angle outcome was performed for both the Schroth method and the core stabilization exercises. Subgroup Schroth method showed the following results: SMD = – 0.417; 95% CI = – 0.705, – 0.129, p = 0.005; heterogeneity I2 = 0%, p = 0.831. Subgroup core stabilization exercises showed the following results: SMD = – 0.345; 95% CI = – 0.596, – 0.94, p = 0.007; heterogeneity I2 = 0%, p = 0.521) (Fig. 5).

Standardized mean difference (SMD) of the Cobb angle outcome. Legend. Squares represent the SMD for each trial. Diamonds represent the pooled SMD across trials

Standardized mean difference (SMD) of the Cobb angle outcome, subgroup analysis. Legend. Squares represent the SMD for each trial. Diamonds represent the pooled SMD across trials
The overall results from post- minus pre-intervention in the experimental group were: SMD = – 0.821; 95% CI = – 1.189, – 0.454, p = 0.104; heterogeneity I2 = 70.06%, p = 0.000. Subgroup Schroth method showed the following results: SMD = – 0.996; 95% CI = – 1.662, – 0.331, p = 0.003; heterogeneity I2 = 77.22%, p = 0.000. Subgroup core stabilization exercises showed the following results: SMD = – 0.700; 95% CI = – 1.143, – 0.256, p = 0.002; heterogeneity I2 = 65.5%, p = 0.005 (supplementary materials).
ATR
A total of 4 studies measured the outcome of ATR [25, 27, 30, 31]: 3 studies using the Schroth method and 1 study using the core stabilization exercises. There was no statistical significance in the total effect size of Schroth method and core stabilization exercises on ATR outcome when the final results of the measurement in the experimental and control group were compared with the initial results in the experimental and control group (SMD = – 0.268; 95% CI = – 0.590, – 0.055, p = 0.104), heterogeneity (I2 = 12.81%, p = 0.332) (Fig. 6). Subsequently, a subgroup analysis for ATR outcome was performed for both the Schroth method and the core stabilization exercises. Subgroup Schroth method showed the following results: SMD = – 0.471, 95% CI = – 0.842, – 0.099, p = 0.013; heterogeneity I2 = 0%, p = 0.471. Subgroup core stabilization exercises showed the following results: SMD = 0.110, 95% CI = – 0.396, 0.617, p = 0.670; heterogeneity I2 = 0%, p = 0.820) (Fig. 7).

Standardized mean difference (SMD) of the angle of trunk rotation (ATR) outcome. Legend. Squares represent the SMD for each trial. Diamonds represent the pooled SMD across trials

Standardized mean difference (SMD) of the angle of trunk rotation (ATR) outcome, subgroup analysis. Legend. Squares represent the SMD for each trial. Diamonds represent the pooled SMD across trials
The overall results from post- minus pre-intervention in the experimental group were: SMD = – 0.992; 95% CI = – 1.472, – 0.513, p < 0.001; heterogeneity I2 = 52.53%, p = 0.049. Subgroup Schroth method showed the following results: SMD = – 1.064; 95% CI = – 1.678, – 0.451, p < 0.001; heterogeneity I2 = 53.58%, p = 0.071. Subgroup core stabilization exercises showed the following results: SMD = – 0.848; 95% CI = – 1.845, 0.149, p = 0.095; heterogeneity I2 = 71.03%, p = 0.063 (supplementary materials).
QoL
A total of 5 studies measured the outcome of QoL [9, 24, 25, 27, 30]: 3 studies using the Schroth method and 2 studies using the core stabilization exercises. The total effect size for all five studies when the final results of the measurement in the experimental and control group were compared with the initial results in the experimental and control groups was: SMD = 0.774; 95% CI = 0.291, 1.257, p = 0.002; heterogeneity I2 = 54.5%, p = 0.067) (Fig. 8). Subsequently, a subgroup analysis for QoL outcome was performed for both the Schroth method and the core stabilization exercises. Subgroup Schroth method showed the following results: SMD = 1.087, 95% CI = 0.597, 1.578, p˂0.001; heterogeneity I2 = 30.06%, p = 0.239. Subgroup core stabilization exercises showed the following results: SMD = 0.292, 95% CI = – 0.240, 0.825, p = 0.282; heterogeneity I2 = 0%, p = 0.592) (Fig. 9).

Standardized mean difference (SMD) of the quality of life outcome. Legend. Squares represent the SMD for each trial. Diamonds represent the pooled SMD across trials

Standardized mean difference (SMD) of the quality of life outcome, subgroup analysis. Legend. Squares represent the SMD for each trial. Diamonds represent the pooled SMD across trials
The overall results from post- minus pre-intervention in the experimental group for the outcome QoL are not presented due to high heterogeneity (I2 = 92.41%, p = 0.000).
Discussion
In this systematic review and meta-analysis, we combined the results of 13 studies in order to calculate the magnitude effect of Schroth method and core stabilization exercises in subjects with idiopathic scoliosis in a total of 412 participants.
In the thirteen studies considered, there were three outcomes measured by at least two studies, and we estimated the magnitude effect of them. In addition, a subgroup analysis of Cobb angle, ATR, and QoL outcomes was performed to compare the two approaches by effect size.
Cobb angle, the most reference value for determining the size of scoliotic deformities, was significantly reduced by applying Schroth method and core stabilization exercises. In our meta-analysis, we calculated the effect size for all three outcomes, and we presented the results comparing post- minus pre-intervention in the experimental and the control group.
By analyzing the outcome of Cobb angle for the total effect size of Schroth method and core stabilization exercises, statistical significance was achieved (SMD = – 0.376), according to the Cohen’s criterion for small effect size (Fig. 4). When subgroup analysis was subsequently performed, it showed that Schroth method had a larger effect size than core stabilization exercises (subgroup Schroth method: SMD = – 0.417; subgroup core stabilization exercises: SMD = – 0.345). From both analyzes, it was determined that there was no occurrence of heterogeneity among the included studies (Fig. 5).
By analyzing the outcome of ATR, negligible heterogeneity appeared, and there was no statistical significance of the effect size (SMD = – 0.268), according to the Cohen’s criterions for small effect size (Fig. 6). Analysis of subgroup for ATR outcome showed that Schroth method had a larger effect size than core stabilization exercises (subgroup Schroth method: SMD = -0.471; subgroup core stabilization exercises: SMD = 0.110) (Fig. 7).
By analyzing the outcomes of QoL, the results showed an almost large effect size (SMD = 0.774), according to the Cohen’s criterions for large effect size, and moderate heterogeneity appears (I2 = 54.5%) (Fig. 8). Analysis of subgroup for the outcome of QoL showed that Schroth method had a larger effect size than core stabilization exercises (subgroup Schroth method: SMD = 1.087; subgroup core stabilization exercises: SMD = 0.292) (Fig. 9). Analysis of subgroup for QoL also solved the problem of heterogeneity that did not occur in the subgroup core stabilization exercises and occurred in the subgroup Schroth method (I2 = 30.06%) (Fig. 9).
The results of the effect size analysis for the Cobb angle outcome only in the experimental group (Schroth and core) show a large effect size (SMD = – 0.821), but with the presence of substantial heterogeneity (I2 = 70.06%), which also occurs in the Schroth group (I2 = 77.22%) and in the core group (I2 = 65.5%) (supplementary materials). The results of the effect size analysis for the ATR outcome only in the experimental group (Schroth and core) show a large effect size (SMD = – 0.992), but with the presence of moderate heterogeneity (I2 = 52.53%), which also occurs in the Schroth group (I2 = 53.58%) and in the core group (I2 = 71.03%) (supplementary materials). The results of the effect size analysis for the QoL outcome only in the experimental group (Schroth and core) show considerable heterogeneity (I2 = 92.41%) and are not even shown.
Twelve included studies had low risk of bias, while the study of Kim [18] the only one had unclear risk of bias. The study of Ko et al. [16] is the only one not reporting whether it used the randomization process. The study of Kuru et al. presented the results of the final measurement for Cobb angle and QoL outcomes as Median (min–max) and not as Mean ± SD, which is a problem during the meta-analysis. This problem has been addressed according to recommendations [22].
Our meta-analysis is the only one so far that has assessed the magnitude effect of these two approaches and, through subgroup analysis, has compared which of these two treatments revealed better results for subjects with IS. A meta-analysis evaluated various conservative methods for treating IS, and some of them used the Schroth and core stabilization exercises [32]. In this meta-analysis, the magnitude effect, in terms of standardized mean difference, was 0.42 for the outcome of Cobb angle with no heterogeneity. Only one meta-analysis [12] examined the effect size for the Schroth method (SMD = 0.724) with high heterogeneity (I2 = 75.67%, p = 0.000), while no meta-analysis examined the effect size of the core stabilization exercises. In the study by Park et al., the magnitude of the effect for the Cobb angle outcome was (SMD = 0.65), with no report of heterogeneity. The magnitude of the effect for the ATR outcome was (SMD = 0.53), with no report of heterogeneity. The magnitude of the effect for the QoL outcome was (SMD = 0.76), also without reports of heterogeneity.
The Schroth method has long been used in the treatment of subjects with IS. Unlike the Schroth method, the core stabilization exercises has recently been used in the treatment of IS. In addition to these two approaches, we have other conservative methods used for these respondents. Many of the studies listed here record statistically significant results on both the impact of Schroth method and the impact of core stabilization exercises [9, 15, 18, 25, 26, 28]. Indeed, these two methods are not mutually exclusive, so they can be used together in the coming period to get better results in the treatment of IS. The various studies included in this meta-analysis provided evidence that conservative approaches as Schroth method and core stabilization exercises have a positive effect on individual outcomes through which the condition of subjects with IS is assessed [3, 9, 15, 16, 18, 24,25,26,27,28,29,30,31].
This study has several limitations. First, despite a comprehensive search, our study included only those written in English. Second, despite a detailed search, the number of studies found that would have common outcomes, except for Cobb angle, is relatively small.
Conclusion
This study addressed two conservative methods used in the treatment of subjects with IS. The current meta-analysis indicates that Schroth method and core stabilization exercises have a positive effect on subjects with IS. Depending on the outcome, the magnitude of the effect ranged from small to almost large. Subgroup analysis showed that the Schroth method had a larger effect size than the core stabilization exercises. Of the four outcomes we used in our meta-analysis, the most representative result is an estimate of the effect size for Cobb angle, as 11 studies participated in the analysis. We believe that our meta-analysis would be a good tool for specialist in physical activity, physiotherapists, and clinicians in solving IS-related problems, as well as an incentive for further work and future research.
References
Liu D, Yang Y, Yu X, Yang J, Xuan X, Yang J, Huang Z (2020) Effects of specific exercise therapy on adolescent patients with idiopathic scoliosis: a prospective controlled cohort study. Spine (Phile Pa 1976) 45:1039–1046. https://doi.org/10.1097/BRS.0000000000003451
Negrini S, Donzelli S, Aulisa AG, Czaprowski D, Schreiber S, de Mauroy JC, Diers H, Grivas TB, Knott P, Kotwicki T, Lebel A, Marti C, Maruyama T, O’Brien J, Price N, Parent E, Rigo M, Romano M, Stikeleather L, Wynne J, Zaina F (2018) 2016 SOSORT guidelines: orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis Spinal Disord 13:3. https://doi.org/10.1186/s13013-017-0145-8
Schreiber S, Parent EC, Khodayari Moez E, Hedden DM, Hill DL, Moreau M, Lou E, Watkins EM, Southon SC (2016) Schroth physiotherapeutic scoliosis-specific exercises added to the standard of care lead to better cobb angle outcomes in adolescents with idiopathic scoliosis - an assessor and statistician blinded randomized controlled trial. PLoS ONE 11:e0168746. https://doi.org/10.1371/journal.pone.0168746
Vrećić A, Glišić M, Živković V (2020) Significance of Schroth method in the rehabilitation of children with structural idiopathic scoliosis - značaj šrot metode u rehabilitaciji dece sa strukturalnom idiopatskom Skoliozom. Medicinski podmladak 71:33–38. https://doi.org/10.5937/mp71-22170
Day JM, Fletcher J, Coghlan M, Ravine T (2019) Review of scoliosis-specific exercise methods used to correct adolescent idiopathic scoliosis. Arch Physiother 9:8. https://doi.org/10.1186/s40945-019-0060-9
Negrini S, Hresko TM, O’Brien JP, Price N, Boards S, Committee SRSN-O (2015) Recommendations for research studies on treatment of idiopathic scoliosis: consensus 2014 between SOSORT and SRS non-operative management committee. Scoliosis 10:8. https://doi.org/10.1186/s13013-014-0025-4
Weinstein SL, Dolan LA, Wright JG, Dobbs MB (2013) Effects of bracing in adolescents with idiopathic scoliosis. N Engl J Med 369:1512–1521. https://doi.org/10.1056/NEJMoa1307337
Monticone M, Ambrosini E, Cazzaniga D, Rocca B, Ferrante S (2014) Active self-correction and task-oriented exercises reduce spinal deformity and improve quality of life in subjects with mild adolescent idiopathic scoliosis. results of a randomised controlled trial. Eur Spine J 23:1204–1214. https://doi.org/10.1007/s00586-014-3241-y
Gur G, Ayhan C, Yakut Y (2017) The effectiveness of core stabilization exercise in adolescent idiopathic scoliosis: a randomized controlled trial. Prosthet Orthot Int 41:303–310. https://doi.org/10.1177/0309364616664151
Lehnert-Schroth C (1992) Introduction to the three-dimensional scoliosis treatment according to Schroth. Physiotherapy 78:810–815. https://doi.org/10.1016/S0031-9406(10)60451-8
Bezalel T, Carmeli E, Levi D, Kalichman L (2019) The effect of Schroth therapy on thoracic kyphotic curve and quality of life in scheuermann’s patients: a randomized controlled trial. Asian Spine J 13:490–499. https://doi.org/10.31616/asj.2018.0097
Park JH, Jeon HS, Park HW (2018) Effects of the Schroth exercise on idiopathic scoliosis: a meta-analysis. Eur J Phys Rehabil Med 54:440–449. https://doi.org/10.23736/S1973-9087.17.04461-6
Ayhan C, Unal E, Yakut Y (2014) Core stabilisation reduces compensatory movement patterns in patients with injury to the arm: a randomized controlled trial. Clin Rehabil 28:36–47. https://doi.org/10.1177/0269215513492443
Muthukrishnan R, Shenoy SD, Jaspal SS, Nellikunja S, Fernandes S (2010) The differential effects of core stabilization exercise regime and conventional physiotherapy regime on postural control parameters during perturbation in patients with movement and control impairment chronic low back pain. Sports Med Arthrosc Rehabil Ther Technol 2:13. https://doi.org/10.1186/1758-2555-2-13
Park SW, Kwon J, Heo YC, Yu W (2021) Effect of core stabilization exercise on cobb’s angle and balance of scoliosis patients. Annal Romanian Soc Cell Biol 25:922–926
Ko KJ, Kang SJ (2017) Effects of 12-week core stabilization exercise on the Cobb angle and lumbar muscle strength of adolescents with idiopathic scoliosis. J Exerc Rehabil 13:244–249. https://doi.org/10.12965/jer.1734952.476
Schreiber S, Parent EC, Hill DL, Hedden DM, Moreau MJ, Southon SC (2018) Patients with adolescent idiopathic scoliosis perceive positive improvements regardless of change in the Cobb angle - results from a randomized controlled trial comparing a 6-month Schroth intervention added to standard care and standard care alone. SOSORT, award winner. BMC Musculoskelet Disord 20:319. https://doi.org/10.1186/s12891-019-2695-9
Kim G, HwangBo PN (2016) Effects of Schroth and Pilates exercises on the Cobb angle and weight distribution of patients with scoliosis. J Phys Ther Sci 28:1012–1015. https://doi.org/10.1589/jpts.28.1012
Adamczewska K, Wiernicka M, Malchrowicz-Mosko E, Malecka J, Lewandowski J (2019) The angle of trunk rotation in school children: a study from an idiopathic scoliosis screening. prevalence and optimal age screening value. Int J Environ Res Public Health 16:87. https://doi.org/10.3390/ijerph16183426
Moher D, Liberati A, Tetzlaff J, Altman DGP (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6:e1000097. https://doi.org/10.1371/journal.pmed.1000097
Health N, Council MR (2009) NHMRC additional levels of evidence and grades for recommendations for developers of guidelines. In. NHMRC Canberra, Australia.
Higgins JPT, Thomas J, Chandler J, Cumpston M, Tianjing L, Page MJ, Welch VA, Cochrane C (2019) Cochrane handbook for systematic reviews of interventions. Wiley
Cohen J (1988) Statistical power analysis for the behavioral sciences. Lawrence Erlbaum Associates
Schreiber S, Parent EC, Moez EK, Hedden DM, Hill D, Moreau MJ, Lou E, Watkins EM, Southon SC (2015) The effect of Schroth exercises added to the standard of care on the quality of life and muscle endurance in adolescents with idiopathic scoliosis-an assessor and statistician blinded randomized controlled trial: “SOSORT 2015 Award Winner.” Scoliosis 10:24. https://doi.org/10.1186/s13013-015-0048-5
Kocaman H, Bek N, Kaya MH, Buyukturan B, Yetis M, Buyukturan O (2021) The effectiveness of two different exercise approaches in adolescent idiopathic scoliosis: a single-blind, randomized-controlled trial. PLoS ONE 16:e0249492. https://doi.org/10.1371/journal.pone.0249492
Park YH, Park YS, Lee YT, Shin HS, Oh MK, Hong J, Lee KY (2016) The effect of a core exercise program on Cobb angle and back muscle activity in male students with functional scoliosis: a prospective, randomized, parallel-group, comparative study. J Int Med Res 44:728–734. https://doi.org/10.1177/0300060516639750
Kuru T, Yeldan I, Dereli EE, Ozdincler AR, Dikici F, Colak I (2016) The efficacy of three-dimensional Schroth exercises in adolescent idiopathic scoliosis: a randomised controlled clinical trial. Clin Rehabil 30:181–190. https://doi.org/10.1177/0269215515575745
HwangBo P-N (2016) Psychological and physical effects of Schroth and Pilates exercise on female high school students with idiopathic scoliosis. J Kor Phys Ther 28:364–368. https://doi.org/10.18857/jkpt.2016.28.6.364
Kim M-J, Park D-S (2017) The effect of Schroth’s three-dimensional exercises in combination with respiratory muscle exercise on Cobb’s angle and pulmonary function in patients with idiopathic scoliosis. Phys Therapy Rehabil Sci 6:113–119
Yagci G, Yakut Y (2019) Core stabilization exercises versus scoliosis-specific exercises in moderate idiopathic scoliosis treatment. Prosthet Orthot Int 43:301–308. https://doi.org/10.1177/0309364618820144
Duangkeaw R, Laddawong T, Rattanapongbundit N, Polmang B (2019) Effects of three-dimension schroth exercises and kinesio taping on general mobility of vertebrae, angle of trunk rotation, muscle strength and endurance of trunk, and inspiratory and expiratory muscle strength in children with idiopathic scoliosis. Walailak J Sci Technol (WJST) 16:965–973
Farooqui SI, Siddiqui PQR, Ansari B, Farhad A (2018) Effects of spinal mobilization techniques in the management of adolescent idiopathic scoliosis - a meta-analysis. Int J Health Sci (Qassim) 12:44–49
Funding
Open access funding provided by Università degli Studi di Palermo within the CRUI-CARE Agreement. No funding was received for conducting this study.
Author information
Authors and Affiliations
Contributions
Conceptualization: PD, AB; Literature search: TŠ, NM; Data analysis: DV; Writing-original draft preparation: VD; Writing-review and editing: VG. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no relevant financial or non-financial interests to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Dimitrijević, V., Viduka, D., Šćepanović, T. et al. Effects of Schroth method and core stabilization exercises on idiopathic scoliosis: a systematic review and meta-analysis. Eur Spine J 31, 3500–3511 (2022). https://doi.org/10.1007/s00586-022-07407-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-022-07407-4