
Abstract
Purpose
There is a paucity of studies on new vertebral body tethering (VBT) surgical constructs especially regarding their potentially motion-preserving ability. This study analyses their effects on the ROM of the spine.
Methods
Human spines (T10-L3) were tested under pure moment in four different conditions: (1) native, (2) instrumented with one tether continuously connected in all vertebrae from T10 to L3, (3) additional instrumented with a second tether continuously connected in all vertebrae from T11 to L3, and (4) instrumented with one tether and one titanium rod (hybrid) attached to T12, L1 and L2. The instrumentation was inserted in the left lateral side. The intersegmental ROM was evaluated using a magnetic tracking system, and the medians were analysed. Please check and confirm the author names and initials are correct. Also, kindly confirm the details in the metadata are correct. The mentioned information is correct
Results
Compared to the native spine, the instrumented spine presented a reduction of less than 13% in global ROM considering flexion–extension and axial rotation. For left lateral bending, the median global ROM of the native spine (100%) significantly reduced to 74.6%, 66.4%, and 68.1% after testing one tether, two tethers and the hybrid construction, respectively. In these cases, the L1-L2 ROM was reduced to 68.3%, 58.5%, and 38.3%, respectively. In right lateral bending, the normalized global ROM of the spine with one tether, two tethers and the hybrid construction was 58.9%, 54.0%, and 56.6%, respectively. Considering the same order, the normalized L1-L2 ROM was 64.3%, 49.9%, and 35.3%, respectively.
Conclusion
The investigated VBT techniques preserved global ROM of the spine in flexion–extension and axial rotation while reduced the ROM in lateral bending.
Similar content being viewed by others


Introduction
Vertebral body tethering (VBT) is increasingly being discussed as an alternative to spinal fusion for selected patients with severe idiopathic scoliosis. In 2019, the Food and Drug Administration (FDA) has approved the first device for US patients, whereas another device has already received CE approval (European approval) in 2017. Several basic sciences as well as clinical studies have confirmed safety and efficacy, including a prospective Humanitarian Device Exemption (HDE) study that was controlled by the FDA [1,2,3,4,5,6,7,8,9,10,11,12,13].
VBT consists of anchors and screws that are inserted into the vertebral bodies from the lateral side then connected and tensioned by a flexible polyethylene cord to correct the spine deformity and stop its progression. The spinal growth is affected by the mechanical stresses described by the Hueter‐Volkmann Law, which states that compression acting on a growth plate retards bone growth and, conversely, tension accelerates it [14, 15]. Accordingly, the mechanical stresses induced after VBT tend to reduce the growth on the convex side while accelerate the growth on the concave side remodelling the spine curvature over time.
Compared to the traditional spinal fusion, VBT has the advantage of allowing for continued spinal growth and mobility. However, some authors have also already observed a non-acceptable high implant failure rate. One paper found a cord rupture rate of 47% two to four years after surgery [8]. Therefore, surgeons have started to modify their surgical techniques. One such modification is the use of a two-cord technique, specifically for surgical treatment of thoracolumbar and lumbar curves [16]. However, there are concerns about additional stiffening of the spine when adding a second tether to a construct, especially in the very flexible lumbar spine. To our best knowledge, no data are available to confirm or disprove this hypothesis.
Therefore, this study aimed to analyse ROM of thoracolumbar and lumbar segments for different VBT constructs in human cadaveric spines. From the clinical point of view, this study tries to answer the question whether a VBT modification can still be motion preserving. We hypothesised that global and segmental motion in lateral bending can be reduced but preserved in flexion–extension and axial rotation after VBT, and the motion markedly dependent on the kind of screw-cord-combination. Please check whether the intended meaning of the sentence ‘From the clinical point of view, this study tries to answer the question whether a VBT modification can still be motion preserving’ is clearly conveyed. It is correct
Materials and methods
Specimen selection and preparation
Six fresh frozen specimens (T10-L3, 1 male and 5 females) who had no history of spinal disease were obtained for testing. The mean age at death was 82 years (range: 73–88 years). The spines were carefully harvested by removing muscles, costovertebral joints, costotransverse joints, and ribs. The vertebrae, intervertebral discs, and ligaments were preserved. For embedding purposes, polymer screws were inserted at the cranial and the caudal ends of each segment. The T12-L1 intervertebral disc was horizontally aligned using a dual crossline laser inside a custom-made guide rail set-up. Each end of the specimen was inserted in an end cap which was subsequently filled with resin (Technovit®, Kulzer GmbH, Wehrheim, Germany) up to approximately 1/2 of their midbodies. After the resin solidified, a strong fixation was created with the vertebrae and easy access to the segment structures for insertion of the instrumentations. Subsequently, the segments were stored at − 18 °C in sealable bags and thawed at 8 °C for 16 h (including embedding time) before testing [17, 18].
Precondition and flexibility testing
The specimens were exposed to a static compressive load of 400 N for 15 min to reduce their water content after unfreezing process [19]. This was realized by using a ZwickRoell® universal testing machine (Zwick GmbH & Co. KG, Baden-Württemberg, Germany). A physiological saline solution (0.9%) was used throughout testing to ensure the specimens from drying-out.
After preconditioning, flexibility tests within the three anatomical planes were performed using a spine testing rig (Fig. 1) custom-built by Dyna-mess Prüfsysteme GmbH® (Stolberg, Germany). A mechanism composed of a rack and gear was used to convert the linear displacement of the machine’s pneumatic actuator to a rotational motion allowing flexion–extension or lateral bending of the spine [20]. The axial rotation was performed by rotating the bottom platform of the machine while holding the most cephalic vertebra. Cardan shafts with an almost frictionless spline ball bearing were used to enable unconstrained movements of the spine in the five degrees of freedom (DoF) that differ to the applied moment [21]. The pure moment applied at the specimen was controlled and recorded by torque transducers positioned along the cardan shaft (T4A with a nominal load of 50 Nm, HBM GmbH, Darmstadt, Germany) and at the machine bottom platform (DMS with a nominal load of 100 Nm, Dyna-mess Prüfsysteme GmbH®) at a frequency of 100 Hz. Both load cells provide a maximum error of 1% relative to the target or recorder value. An Aurora® electromagnetic tracking system (NDI Europe GmbH, Radolfzell, Germany) was used to track the 6 DoF of microsensors that were inserted in the middle of the vertebral bodies [22, 23]. The Euler angles were recorded to detect the orientation of the sensors. This AURORA® system provides deviations lower than 0.1 mm and 0.1° [20]. The presented testing apparatus showed deviations of less than 1% of translation and rotation compared to non-metal environment. A balance system composed of ropes and pulleys was used to compensate for the weight of 1.5 kg applied at the top of the specimen due to the resin and cardan shaft.

Testing apparatus for testing of the spine. The pure moment is applied to the specimen by a cardan shaft. An electromagnetic system is used to track the kinematics of microsensors inserted in the vertebral bodies. For axial rotation, the specimen is moved to a rotator platform and a cardan shaft is attached to the most cephalic vertebra
The position of the microsensors was recorded with the spine under no load to detect the vertebrae positions before and after instrumentation in order to determine the scoliotic angles. The specimens underwent three loading cycles at a rate of 1°/s to a maximum moment of ± 6 Nm [24]. The first two cycles served as precycles to minimize the effect of the viscoelastic response whereas the last cycle was used for evaluation [19].
Surgical reconstruction groups
The spines were tested in flexion–extension, lateral bending, and axial rotation in four different conditions: (1) native, (2) instrumented with one tether continuously attached in all vertebrae from T10 to L3, (3) additional instrumented with a second tether continuously connected in all vertebrae from T11 to L3, and (4) instrumented with one tether and one titanium rod (hybrid) attached to T12, L1 and L2 vertebrae (Fig. 2). The instrumentation was obtained from Globus Medical (Audubon, PA, USA) and implanted in the left lateral side of the spine by an experienced surgeon. The first line of screws was inserted close to the foramen with bicortical purchase. The tether made of polyethylene terephthalate cord was locked after applying a sequential tension force of 100 N [24]. For the attachment of the second tether or the titanium rod, the second line of screws was placed anteriorly to the first line of screws. The second tether was inserted without pretension. The sequence of the trials within each test condition and the groups were randomized to avoid bias such as screw loosening and softening effects of specimen degeneration [18, 24].

Left lateral view of the spine (T10-L3) instrumented with 1 tether a, 2 tethers b, and 1 tether combined with a titanium rod c
Data analysis
The ROM of the whole spine (T10-L3) and L1-L2 segment were calculated as described previously by Beckmann et al. [18, 23]. The Euler angles recorded by the magnetic tracking system were converted to rotation matrices for each sensor. The ROM was defined as the angular displacement between two vertebrae and was calculated using basis transformations [20]. A sensor was aligned with the universal joint connector at the top of the most cephalic vertebra to detect the main loading direction for the spine in the undeformed state for the cases of flexion–extension and lateral bending [23]. For axial rotation, the main loading direction was set as the plane parallel to the rotatory platform of the machine which has the load cell. The axes of the magnetic tracking receivers’ coordinate systems were projected on the primary direction of the load to calculate the 2D ROM [20, 23]. The average moment for the same ROM values of the loading and unloading curves of the hysteresis was calculated [25]. This process provided the middle curve of the hysteresis which is presented and discussed. Changes in the coronal plane angles due to the insertion of each surgical construct were determined with respect to the native spine. Data from broken sensors or when the orientation of the sensors were not uniquely defined by the Euler Angles (gimbal lock) were excluded. The 2D ROM at the maximum load applied on the whole spine (± 6 Nm) was considered for statistical analysis and was calculated concerning the neutral position of the spine for each trial. All ROM values were standardized by dividing the 2D ROM of each trial to the respective 2D ROM of the native spine (intact = 100%). The analysis was performed using MATLAB (version R2019b, The MathWorks, Natick, MA, USA). The Mauchly's sphericity test and the Shapiro–Wilk test provided evidence that part of the 2D ROM data does not hold the sphericity assumption and is non-normally distributed (p ≤ 0.05). The nonparametric Wilcoxon signed-rank test for repeated measures was used to determine statistical significance between the 2D ROM of each surgical reconstruction group. One-tailed tests were performed assuming a stepwise reduction in the 2D ROM of the spine for the native state, instrumented with one tether, instrumented with 2 tethers, and instrumented with the hybrid construction, respectively. After standardization of the 2D ROM with respect to the native spine for each trial, the medians were calculated and analysed for statistical comparisons. Therefore, relative values representing comparisons between the ROM of different groups were calculated only after standardization of each trial.
Results
Compared to the native state, the spine instrumented with one tether, two tethers, and the hybrid construction bended to the left side and presented median global (interquartile range) Cobb angles (n = 4) of 2.51° (2.64), 2.52° (3.03) and 2.95° (2.71), respectively. In these cases, the median L1-L2 Cobb angles (n = 4) was 0.49° (0.90), 0.63° (0.89), and 0.93° (1.19), respectively.
Herein, the analysis is performed considering the 2D ROM of the spine at the maximum load (± 6 Nm). The absolute median of the global and segmental ROM (°) of the native spine and the spine with different surgical constructs in flexion–extension (n = 5 for L1-L2 and n = 6 for T10-L3), lateral bending (n = 6), and axial rotation (n = 4) is shown in Table 1 and Fig. 3. The median global ROM of the native spine for flexion, extension, left and right lateral bending, left and right axial rotation was 15.25°, 13.39°, 19.05°, 14.26°, 11.74°, and 12.67°, respectively (Table 1). The L1-L2 ROM for these cases was 2.50°, 2.58°, 3.59°, 2.54°, 2.37°, and 1.67°, respectively. For most of the cases, the median global ROM (T10-L3) and median segmental ROM (L1-L2) of the spine stepwise reduced after implanting one tether, two tethers, and the hybrid construction, respectively (Fig. 3).

Median of the global ROM (T10-L3) and segmental (L1-L2) ROM of the native spine and the spine with different surgical constructs in flexion–extension (n = 5 for L1-L2 and n = 6 for T10-L3), lateral bending (n = 6), and axial rotation (n = 4). Positive values represent flexion, right lateral bending, and left axial rotation. The vertical axis represents the results of the moment applied to the whole specimen
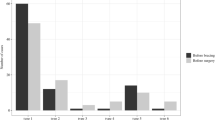
Compared to the native spine, the instrumented spine with one or two tethers presented a statistically significant reduction (p ≤ 0.05) of less than 9.7% in global ROM of the spine in flexion or extension (Fig. 4). Figure 4 also presents the number of specimens used for analysis of relative comparisons. For the L1-L2 segment, the maximum statistically significant reduction in ROM was less than 9.5% for the spine with two tethers compared to the native spine in flexion. For axial rotation motion, a maximum decrease of 13.5% occurred for the L1-L2 ROM of the spine with two tethers in right axial rotation and was statistically significant (p ≤ 0.05).

Effects of different surgical constructs on the motion of the spine in flexion–extension, lateral bending, and axial rotation. The data were standardized concerning the ROM of the native spine. The bars and error bars represent the medians of 2D ROM and interquartile ranges, respectively. The symbol * represents p ≤ 0.05. The numbers at the bottom of the bars indicate the numbers of specimens used for calculation of the medians when they differ of 6 specimens
Compared to the spine instrumented with one tether, the global ROM and local ROM of the spine with two tethers slightly reduced in all loading directions except for the L1-L2 segment in extension (Fig. 3). Considering the motions of flexion, extension, left and right axial rotation, the maximum significant reduction in ROM was 5.9% for the global ROM of the spine in flexion and 5.7% for the local ROM of the spine in right axial rotation (Fig. 4).
For left lateral bending, the median global ROM of the native spine (100%) significantly reduced to 74.6, 66.4, and 68.1% after testing one tether, two tethers, and the hybrid construction, respectively (Fig. 4). In these cases, the L1-L2 ROM was reduced to 68.3%, 58.5%, and 38.3%, respectively. In right lateral bending, the normalized global ROM of the spine with one tether, two tethers, and the hybrid construction was 58.9%, 54.0%, and 56.6%, respectively. Considering the same order, the normalized L1-L2 ROM was 64.3%, 49.9%, and 35.3%, respectively. For left and right lateral bending, all comparisons were statistically significant (p ≤ 0.05) except for the global ROM of the spine with two tethers against the spine with the hybrid construction.
The hybrid technique significantly reduced the global ROM of the native spine less than 10.5% for flexion or extension (Fig. 4). Following a similar trend, the L1-L2 segment presented a significant reduction of 26.8% in flexion and a non-significant reduction of 8.6% in extension. The global ROM and local ROM reduced 10.0% and 28.9% in right axial rotation and 13.0% and 32.9% in left axial rotation, respectively. These comparisons were statistically different.
Discussion
This is the first study to analyse the effects of different VBT constructs on the ROM of the thoracolumbar spine. VBT is a promising new treatment option for severe scoliosis. Surgeons have started to use a 2-cord technique for VBT, specifically for the treatment of thoracolumbar and lumbar curves because it has been hypothesized that the incidence for tether ruptures would be even higher in the flexible lumbar spine [16]. Several animal studies as well as clinical short- to mid-term observations have been able to proof the growth modulation effect of VBT [2, 6,7,8,9, 11, 26] but limited data were available on the motion-preserving ability of this technique. Our study showed that the surgical constructs with one tether or two tethers slightly restricted the global and L1-L2 motion of the native spine in flexion or extension (< 10%) and left or right axial rotation (< 14%). This result was expected for flexion or extension because the tethers were inserted close to the centre of rotation of each spinal segment providing a relatively small level arm. Moreover, the tethers do not provide resistance to bending. Additionally, the most effective resistance of the tether occurs along its directions and therefore, along the spine curvature. Only a small component of the force applied by the tether or the tethers is situated on the horizontal plane, and therefore, the resistive moment is relatively small in left or right axial rotation.
The insertion of one tether with a sequential tension force of 100 N produced a change in the global Cobb angle of the T10-L3 spine (2.51°) lower than the value obtained by Lavelle et al. [24] for the T4-T12 spine in the cases of T4–T12 continuous tensioned (4.6 ± 3.2°) and T4–T12 continuous sequentially tensioned (9.9 ± 5.5°). The differences might be due to the differences in the number of segments and properties of the specimens. Moreover, these data have limitations because the instrumented spine has multiple neutral positions. Compared to the spine with one tether, the insertion of the second tether resulted in a neglected change in the global Cobb angle (0.01°) since it was inserted without pretension.
We found that a 2-cord technique does not have an additional limiting effect on the kinematics of the spine with 1 cord. The little effects suggest that the first tether restricts most of the motion of the spine while the second cord remained relatively relaxed. In right lateral bending, for example, the first tether significantly reduced the global ROM of the native spine from 100 to 58.9% whereas the additional tether significantly reduced to 54.0%. These results are associated with the pretension of 100 N applied to the first tether whereas the second tether received no pretension. Moreover, the additional cord connected in parallel to a relative stiff cord theoretically does not add much stiffness to the whole system. The no pretension mirrors the clinical scenario in which the second tether is considered a supportive (back-up) tether that could also limit endpoint of rotation. In the clinical setting, the anterior tether also needs to have less tension to not have a kypohogenic effect on the lumbar spine. Possible effects of pretensioning the second tether would be increase of the Cobb angle and higher compression on the lateral side of the spine near the tether whereas higher traction on the other side. This could potentially reduce the ROM in lateral bending as occurred to the insertion of one tether compared to the native spine. Please check whether the usage of the term ‘kypohogenic’ in the sentence ‘. In the clinical setting, the anterior tether also needs to have less tension to not have a kypohogenic effect on the lumbar spine’ is OK. It is correct
In right lateral bending, the screws act as lever arms, and the tethers provide resistance to tension resulting in a reduction of the motion of the spine. In left lateral bending, the tethers tend to offer no resistance or buckle while the spine is bending. However, our results showed that the ROM of the spine is reduced not only for right lateral bending but also for left lateral bending. It possibly occurs because the first tether was inserted with a pretension which changed the neutral position of the spine and tensioned the soft tissue at its right side.
From the mechanical point of view, the spine with the VBT implants forms a complex system that connects several vertebrae and can be implemented with a second tether or a rod. Even for simple loading conditions such as pure moment, the biomechanical characteristics (e.g. stiffness) of one segment can affect the response of the other segments because the cord is continuously connected in all vertebrae and responsible for transferring load. The same applies to the process of inserting an extra cord or rod with pretension which can add or release the tension of the first cord. Therefore, the moment applied to the specimen by the machine can differ from the moment experienced by a certain segment (e.g. L1-L2).
Primary stability is an important requirement for VBT implants, and it would be preferred if the implants last at least until skeletal maturity, which in some cases, could last a few years from the time of surgery. Short-term success rates (no fusion required) after VBT have been observed [27], but tether breakages seem to be one of the most frequently observed implant-related complications, which may make results after VBT less predictable. However, the definition of success remains controversial. While some authors define prevention of spinal fusion as success, others define a Cobb angle below 35° (others below 30°) as success. Most authors agree that radiographic signs of mechanical failure, e.g. tether breakage, would not necessarily define clinical failure. Newton et al. suspected a broken tether in 47% of his patients and Hoernschemeyer in 48% within a 2- to 5-year follow-up period – both after thoracic VBT [8, 11]. Although both study groups agree that most patients with a tether rupture will still have a successful outcome, it is understandable that surgeons would like to decrease the incidence of this implant-related complication.
We also tested the use of a hybrid technique because this can become an option for patients with very rigid apices. While a hybrid technique will reduce ROM at the fused level, it may only have a limited stiffening effect on the global ROM. Previous studies suggested that a larger number of fused levels increase the risk of adjacent segment degeneration [28,29,30]. Therefore, the hybrid technique has the potential to reduce adjacent segment degeneration since the number of fused segments are less than traditional T10-L3 fusion. Nohara et al. [28] observed disc degeneration in the unfused segments below the instrumentation in 48% of patients 10 years after fusion surgery for adolescent idiopathic scoliosis and a correlation between the lowest instrumented vertebra with the incidence of disc degeneration.
The major limitation of this study is the use of non-scoliotic osteoporotic adult cadaveric spines to investigate surgical techniques that are typically used in children and adolescents. It occurs due to the difficulty of obtaining specimens with specific characteristics and it is a limitation present in most of the studies in the literature [24, 31]. Moreover, the limited number of specimens led to non-statistically significant values for some comparisons of the ROM between the surgical groups. This was also contributed by the fact that data were missing for some trials due to broking sensors or non-uniquely defined Euler Angles. In axial rotation, for instance, five specimens were used in most of the comparisons. In left axial rotation, only four datasets were analysed for two tethers. Also, a follower load could be implemented using two ropes attached at the vertebral bodies to simulate the body weight. Future work is the application of a finite element model to overcome these limitations and provide supplementary information to the experimental data. Despite these limitations, it is the first biomechanical study that compares different VBT techniques in a human thoracolumbar spine and still adds significant information to the existing literature.
This biomechanical study confirms that VBT is a motion-preserving surgical technique for flexion–extension and axial rotation. However, the technique can reduce motion in lateral bending. Moreover, the surgical variations like a double-tether technique or a hybrid surgery may be still able to preserve the global motion of the spine in flexion–extension and axial rotation.
References
Baroncini A, Rodriguez L, Verma K, Trobisch PD (2019) Feasibility of single-staged bilateral anterior scoliosis correction in growing patients. Glob Spine J. https://doi.org/10.1177/2192568219892904
Trobisch PD, Kobbe P, Baroncini A (2019) Dynamic scoliosis correction as alternative treatment for patients with adolescent idiopathic scoliosis: a non-fusion surgical technique. Z Orthop Unfall. https://doi.org/10.1055/a-0983-1265
Samdani AF, Ames RJ, Kimball JS et al (2014) Anterior Vertebral Body Tethering for Idiopathic Scoliosis. Spine 39:1688–1693. https://doi.org/10.1097/BRS.0000000000000472
Baker CE, Kiebzak GM, Neal KM (2021) Anterior vertebral body tethering shows mixed results at 2-year follow-up. Spine Deform 9:481–489. https://doi.org/10.1007/s43390-020-00226-x
Liu J, Li Z, Shen J, Xue X (2015) Spinal growth modulation with posterior unilateral elastic tether in immature swine model. Spine J 15:138–145. https://doi.org/10.1016/j.spinee.2014.07.008
Newton PO, Farnsworth CL, Faro FD et al (2008) Spinal growth modulation with an anterolateral flexible tether in an immature bovine model. Spine (Phila Pa 1976) 33:724–733. https://doi.org/10.1097/BRS.0b013e31816950a0
Newton PO, Fricka KB, Lee SS et al (2002) Asymmetrical Flexible Tethering of Spine Growth in an Immature Bovine Model. Spine (Phila Pa 1976) 27:689–693. https://doi.org/10.1097/00007632-200204010-00004
Newton PO, Kluck DG, Saito W et al (2018) Anterior spinal growth tethering for skeletally immature patients with scoliosis. J Bone Jt Surg 100:1691–1697. https://doi.org/10.2106/JBJS.18.00287
Samdani AF, Ames RJ, Kimball JS et al (2015) Anterior vertebral body tethering for immature adolescent idiopathic scoliosis: one-year results on the first 32 patients. Eur Spine J 24:1533–1539. https://doi.org/10.1007/s00586-014-3706-z
Boudissa M, Eid A, Bourgeois E et al (2017) Early outcomes of spinal growth tethering for idiopathic scoliosis with a novel device: a prospective study with 2 years of follow-up. Child’s Nerv Syst 33:813–818. https://doi.org/10.1007/s00381-017-3367-4
Hoernschemeyer DG, Boeyer ME, Robertson ME et al (2020) Anterior vertebral body tethering for adolescent scoliosis with growth remaining. J Bone Jt Surg Publish Ah. https://doi.org/10.2106/JBJS.19.00980
Pehlivanoglu T, Oltulu I, Erdag Y et al (2021) Double-sided vertebral body tethering of double adolescent idiopathic scoliosis curves: radiographic outcomes of the first 13 patients with 2 years of follow-up. Eur Spine J. https://doi.org/10.1007/s00586-021-06745-z
Pehlivanoglu T, Oltulu I, Erdag Y et al (2021) Comparison of clinical and functional outcomes of vertebral body tethering to posterior spinal fusion in patients with adolescent idiopathic scoliosis and evaluation of quality of life: preliminary results. Spine Deform. https://doi.org/10.1007/s43390-021-00323-5
Mehlman CT, Araghi A, Roy DR (1997) Hyphenated history: the Hueter-Volkmann law. Am J Orthop 26:798–800
Smit TH (2020) Adolescent idiopathic scoliosis: The mechanobiology of differential growth. JOR SPINE. https://doi.org/10.1002/jsp2.1115
Baroncini A, Trobisch PD, Migliorini F (2020) Learning curve for vertebral body tethering: analysis on 90 consecutive patients. Spine Deform. https://doi.org/10.1007/s43390-020-00191-5
Herren C, Beckmann A, Meyer S et al (2017) Biomechanical testing of a PEEK-based dynamic instrumentation device in a lumbar spine model. Clin Biomech 44:67–74. https://doi.org/10.1016/j.clinbiomech.2017.03.009
Beckmann A, Nicolini LF, Grevenstein D et al (2020) Biomechanical in vitro test of a novel dynamic spinal stabilization system incorporating polycarbonate urethane material under physiological conditions. J Biomech Eng DOI 10(1115/1):4044242
Heuer F, Schmidt H, Klezl Z et al (2007) Stepwise reduction of functional spinal structures increase range of motion and change lordosis angle. J Biomech 40:271–280. https://doi.org/10.1016/j.jbiomech.2006.01.007
Beckmann A, Herren C, Mundt M et al (2018) A new in vitro spine test rig to track multiple vertebral motions under physiological conditions. Biomed Eng / Biomed Tech 63:341–347. https://doi.org/10.1515/bmt-2016-0173
Wilke H-J, Claes L, Schmitt H, Wolf S (1994) A universal spine tester for in vitro experiments with muscle force simulation. Eur Spine J 3:91–97. https://doi.org/10.1007/BF02221446
Eschweiler J, Stromps J-P, Fischer M et al (2016) Development of a biomechanical model of the wrist joint for patient-specific model guided surgical therapy planning: Part 1. Proc Inst Mech Eng Part H J Eng Med 230:310–325. https://doi.org/10.1177/0954411916632791
Beckmann A, Herren C, Nicolini LF et al (2019) Biomechanical testing of a polycarbonate-urethane-based dynamic instrumentation system under physiological conditions. Clin Biomech 61:112–119. https://doi.org/10.1016/j.clinbiomech.2018.12.003
Lavelle WF, Moldavsky M, Cai Y et al (2016) An initial biomechanical investigation of fusionless anterior tether constructs for controlled scoliosis correction. Spine J 16:408–413. https://doi.org/10.1016/j.spinee.2015.11.004
Wilmanns N, Beckmann A, Nicolini LF, et al (2021) Biomechanical in vitro and finite element study on different sagittal alignment postures of the lumbar spine during multiaxial daily motion. Submitt to J Biomech Eng
Pehlivanoglu T, Oltulu I, Ofluoglu E et al (2020) Thoracoscopic vertebral body tethering for adolescent idiopathic scoliosis: a minimum of 2 years’ results of 21 patients. J Pediatr Orthop 40:575–580. https://doi.org/10.1097/BPO.0000000000001590
Alanay A, Yucekul A, Abul K et al (2020) Thoracoscopic Vertebral Body Tethering for Adolescent Idiopathic Scoliosis. Spine (Phila Pa 1976) Publish Ah. https://doi.org/10.1097/BRS.0000000000003643
Nohara A, Kawakami N, Seki K et al (2015) The effects of spinal fusion on lumbar disc degeneration in patients with adolescent idiopathic scoliosis: a minimum 10-year follow-up. Spine Deform 3:462–468. https://doi.org/10.1016/j.jspd.2015.04.001
Rousseau M-A, Lazennec J-Y (2016) Degenerative disease supra- and infra-jacent to fused lumbar and lumbo-sacral levels. Orthop Traumatol Surg Res 102:S1–S8. https://doi.org/10.1016/j.otsr.2015.12.003
Schulte TL, Leistra F, Bullmann V et al (2007) Disc height reduction in adjacent segments and clinical outcome 10 years after lumbar 360° fusion. Eur Spine J 16:2152–2158. https://doi.org/10.1007/s00586-007-0515-7
Holewijn RM, de Kleuver M, van der Veen AJ et al (2017) A novel spinal implant for fusionless scoliosis correction: a biomechanical analysis of the motion preserving properties of a posterior periapical concave distraction device. Glob Spine J 7:400–409. https://doi.org/10.1177/2192568217699377
Funding
Open Access funding enabled and organized by Projekt DEAL. This study was supported by Globus Medical, Inc.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Data availability
All data and materials comply with field standards.
Ethics approval
The present cadaveric study was approved by the ethical committee board of the RWTH Aachen University (No. EK 280/20).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Nicolini, L.F., Kobbe, P., Seggewiß, J. et al. Motion preservation surgery for scoliosis with a vertebral body tethering system: a biomechanical study. Eur Spine J 31, 1013–1021 (2022). https://doi.org/10.1007/s00586-021-07035-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-021-07035-4