
Abstract
Purpose
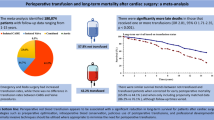
Aspirin may prevent organ dysfunction in critically ill patients and mitigate transfusion associated acute lung injury. We hypothesized that aspirin use might be associated with decreased morbidity and mortality in massively transfused cardiac surgery patients.
Methods
A single center retrospective cohort study was performed using data from an 8.5-year period (2006–2014). Massive transfusion was defined as receiving at least 2400 ml (8 units) of red blood cell units intraoperatively. A propensity score model was created to account for the likelihood of receiving aspirin and matched pairs were identified using global optimal matching. The primary endpoint, in-hospital mortality, was compared between aspirin users and non-users. Secondary outcomes including: ICU hours, mechanical lung ventilation hours, prolonged mechanical lung ventilation (>24 h), pneumonia, stroke, acute renal failure, atrial fibrillation, deep sternal wound infection, and multiple organ dysfunction syndrome were also compared.
Results
Of 7492 cardiac surgery patients, 452 (6 %) were massively transfused and mortality was 30.6 %. There were 346 patients included in the matched cohort. No significant association was found between preoperative aspirin use and in-hospital mortality; absolute risk reduction with aspirin = 7.5 % (95 % CI −2.0 to 16.9 %, p = 0.12). Preoperative aspirin use was associated with fewer total mechanical lung ventilation hours (p = 0.02) and less prolonged mechanical lung ventilation; absolute risk reduction = 11.0 % (95 % CI 1.1–20.5 %, p = 0.02).
Conclusions
Preoperative aspirin use is not associated with decreased in-hospital mortality in massively transfused cardiac surgery patients, but may be associated with less mechanical lung ventilation time.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Life threatening hemorrhage and massive transfusion occur in trauma, obstetrics, liver transplantation and cardiac surgery and are associated with a high mortality of up to 20 % [1]. Few interventions have been shown to improve survival in these patients. Administration of antifibrinolytic drugs has become a common practice in cardiac surgery to mitigate blood loss, but antifibrinolytic drugs have not been shown to decrease mortality in massively transfused cardiac surgery patients [2–4].
Up to 8 % of cardiac surgery patients require massive transfusion and severe hemorrhage is independently associated with mortality [5, 6]. Allogeneic transfusion is associated with numerous postoperative complications including: pulmonary complications, sepsis, atrial fibrillation, renal failure, and stroke [7]. To our knowledge, no interventions have been shown to decrease the non-infectious complications of massive transfusion, such as lung injury, to date.
Aspirin may decrease organ failure in the critically ill [8]. It may also improve pulmonary function in patients at risk for acute respiratory distress syndrome (ARDS) and transfusion related acute lung injury (TRALI) [9, 10]. In a single center cohort of aortic valve replacement surgery patients, we previously found that preoperative aspirin was not associated with a reduced risk of ARDS [11]. Alternatively, studies have shown that aspirin improves oxygenation in cardiac surgery patients and attenuates cardiopulmonary bypass (CPB) induced lung injury, possibly by reducing thromboxane production [12, 13]. Aspirin has also been associated with increased bleeding and transfusion risks in cardiac surgery and non-cardiac surgery patients, making its continued use during the perioperative period controversial [14, 15]. We hypothesized that preoperative aspirin use might be associated with decreased pulmonary morbidity and mortality in massively transfused cardiac surgery patients.
Patients and methods
Setting, participants, and data sources
The institutional review board at The University of Maryland School of Medicine approved the study. All adult patients having cardiac surgery at our center between January 1st 2006 and June 30th 2014 were screened for massive intraoperative transfusion using our institutional Society for Thoracic Surgeons (STS) database. This database is regularly updated and maintained by a dedicated data manager in our hospital’s cardiac surgery department. Standards for data management are established and monitored by the STS. Massive transfusion was defined as receiving 2400 ml (8 units) of packed red blood cells (RBCs) during surgery. The study period was selected because it represented a contemporary period of relatively consistent data collection practices and clinical practices.
Variables
Definitions for variables were based upon STS database specifications (versions 2.61 and 2.73) (http://www.sts.org). The following bleeding and transfusion specific variables were available in the database: preoperative hematocrit, preoperative warfarin use, intraoperative RBC transfusion, intraoperative fresh frozen plasma (FFP) transfusion, intraoperative platelet transfusion, postoperative RBC transfusion, postoperative FFP transfusion, postoperative platelet transfusion, antifibrinolytic medications, administration of recombinant activated FVII, and reoperation for bleeding. We also collected preoperative international normalized ratio (INR) and platelet count. Transfusion volumes were estimated using the following volume conversions per unit: 300 ml = 1 unit of RBCs, 250 ml = 1 unit of FFP, and 200 ml = 1 apheresis platelet unit.
In addition to bleeding and transfusion data we collected the following variables: age, sex, weight, height, diabetes mellitus, dyslipidemia, hypertension, history of end stage renal disease requiring dialysis, baseline creatinine, infectious endocarditis, chronic lung disease, peripheral vascular disease, cerebral vascular disease, previous cardiac interventions, congestive heart failure within 2 weeks of surgery, prior myocardial infarction, left ventricular ejection fraction, preoperative beta blocker use, preoperative statin use, type of surgery, year of surgery, urgency of procedure, and CPB time.
Blood transfusion practices
During the study period, transfusions were administered at the discretion of attending anesthesiologists, cardiac surgeons, and intensivists. General lower limit transfusion thresholds for cardiac surgery patients at our institution are: RBC transfusion for a hemoglobin level less than 7 mg/dl, FFP transfusion for bleeding patients with an INR greater than 1.5, platelet transfusion in bleeding patients with a platelet count less than 100,000 platelets/μl, and cryoprecipitate transfusion in bleeding patients with a fibrinogen level less than 200 mg/dl. Three different antifibrinolytics were used during the study period, including epsilon-aminocaproic acid, tranexamic acid, and aprotinin, but most patients received epsilon-aminocaproic acid with a single bolus dose of 10 g and 1 g/h infusion until 6 h after surgery.
Exposure variable
Preoperative aspirin use was based on the STS database definition, where it is coded as a dichotomous variable indicating whether a patient took aspirin within 5 days of surgery. There was no information on aspirin dose or specific time of last administration.
Outcome variables
All outcome variables were defined according to the STS database specifications. The primary outcome variable was in-hospital mortality. The secondary outcome variables were total ventilator hours, prolonged mechanical lung ventilation (defined as > 24 h by the STS), total intensive care unit (ICU) hours, postoperative pneumonia, postoperative stroke, postoperative acute renal failure, postoperative atrial fibrillation, postoperative deep sternal wound infection, and postoperative multiple organ dysfunction syndrome (MODS). All patients were cared for in the intensive care unit collaboratively by intensivists and cardiac surgeons. There were no standardized protocols for postoperative mechanical lung ventilation during the study period except in patients with ARDS who received a 6 ml/kg tidal volume based on predicted body weight.
Statistical methods
Statistical analyses were performed using SAS 9.3 (Cary, NC, USA). All tests were two-tailed with a p value less than 0.05 considered statistically significant. All cardiac surgery patients during the study period were analyzed to determine whether aspirin use was generally associated with an increased risk of intraoperative RBC transfusion. The Wilcoxon rank-sum test was used to test for a difference in intraoperative RBC transfusion between aspirin users and non-users. We also compared the rate of massive transfusion between aspirin users and non-users in the entire cardiac surgery population. This analysis was performed to rule out the possibility of preferential selection of aspirin users into the massive transfusion cohort.
Massively transfused patients, defined by receiving ≥2400 ml (8 units) of intraoperative RBCs, were then identified from the full cohort and stratified by aspirin use. Patient characteristics were compared using the Wilcoxon rank-sum tests for continuous variables and chi-squared tests for categorical variables. Because baseline characteristics were highly imbalanced between aspirin users and non-users a propensity score model for aspirin use was created to reduce bias and control for confounding.
Propensity scores were calculated using a non-parsimonious logistic regression model with aspirin as the dependent variable and multiple independent variables. Independent variables were selected for inclusion based on recommendations in the published literature [17–19]. All independent variables were associated with either the outcome variable alone (mortality) or the outcome variable and exposure variable (mortality and aspirin use). The following independent variables were included in the final model: type of surgery, urgency of surgery, year of surgery, cardiopulmonary bypass time, antifibrinolytic use, age, sex, weight, height, preoperative platelet count, preoperative hematocrit, preoperative INR, baseline hemodialysis, baseline creatinine, chronic lung disease, hypertension, diabetes, dyslipidemia, peripheral vascular disease, cerebral vascular disease, infective endocarditis, prior myocardial infarction, previous cardiac intervention, congestive heart failure within 2 weeks of surgery, beta blocker use, statin use, and warfarin use.
Once a propensity score was calculated for each patient, propensity score matching was performed using a global optimal matching algorithm [20]. Matched pairs were identified and included in a final matched cohort. Patients in the matched cohort were then divided into those who received aspirin and those who did not. The data set was complete except for 48 patients (13.9 %) who had no information of postoperative mechanical lung ventilation hours. Of these patients, 23 were in the aspirin group and 25 were in the control group. Continuous variables were summarized for the aspirin group and control group as the median value and interquartile range (Q1, Q3) and categorical variables were summarized as the number and percent of total. To evaluate how well the propensity score model and matching algorithm balanced important covariates between groups, standardized differences were calculated for all variables that were entered into the propensity score model. Residual imbalance between the two groups was considered to be present when standardized differences were greater than 0.2.
Continuous outcome variables were compared between the exposure and control groups using the Wilcoxon rank-sum test. Dichotomous outcome variables were compared between the exposure and control groups using the chi-square test and absolute risk reductions with 95 % confidence intervals were calculated for all variables. For absolute risk reductions that were found to be statistically significant, a number needed to treat was reported.
Results
A total of 7492 patients had cardiac surgery during the study period. Of these, 4545 patients (60.6 %) were taking aspirin preoperatively. Preoperative aspirin use had a crude association with intraoperative RBC transfusion in the full cohort, suggesting that aspirin may have increased the risk for bleeding among all cardiac surgery patients. The median volume of intraoperative RBC transfusion was 600 ml in aspirin users and 300 ml in non-users, p = 0.02. A total of 452 patients were massively transfused with 6.3 % of non-aspirin users and 5.8 % of aspirin-users being massively transfused (p = 0.36). Of the patients that were massively transfused, 58.6 % were taking aspirin preoperatively, which was less than the proportion taking aspirin in the full cohort. The final propensity score matched cohort of massively transfused patients included 346 patients (173 pairs) with a median difference in propensity score between pairs of 0 (interquartile range = 0.00, 0.22).
Baseline characteristics of massively transfused patients taking aspirin and those not taking aspirin prior to matching are shown in Table 1. The two groups were highly imbalanced. Characteristics of patients in the matched cohort are shown in Table 2. Most covariates became balanced between the groups, but statin use and dyslipidemia could not be well balanced in the data set without reducing the total number of matched pairs to a very low level. There were no significant differences in RBC, FFP, or platelet transfusion between the two groups after matching, as is shown in Table 3.
Patient outcomes are shown in Table 4. In-hospital mortality for the matched cohort was 28.6 %. There was no significant difference in mortality between aspirin users and non-users; absolute risk reduction = 7.5 % (−2.0 to 16.9 %, p = 0.12). There were also no significant differences in operative mortality, postoperative day of death, cause of death, postoperative pneumonia, postoperative stroke, postoperative acute renal failure, postoperative atrial fibrillation, deep sternal wound infection, or multiple organ dysfunction syndrome (MODS) between groups. Aspirin users did have fewer total mechanical lung ventilation hours, less prolonged mechanical lung ventilation, and fewer total ICU hours (p = 0.02, and 0.02, 0.05 respectively). The distributions of total mechanical lung ventilation hours in aspirin users and non-users are shown in Fig. 1. The absolute risk reduction for prolonged mechanical lung ventilation (> 24 h) was 11.0 % for aspirin users (95 % CI 1.1 to 20.5 %, p = 0.02), suggesting that exposure of 9 patients to aspirin before massive transfusion could prevent 1 case of prolonged mechanical lung ventilation. Exclusion of patients who died during the first 48 h after surgery from the dataset had no effect on the difference in total mechanical lung ventilation time (p = 0.008 for the Wilcoxon rank-sum test comparing ventilation hours).

Box and whisker plots showing total mechanical lung ventilation hours in aspirin users and non-users
Discussion
Massive blood transfusion is associated with a high mortality rate and numerous complications. Previous observational studies suggested that high ratios of transfused FFP and platelets to RBCs might decrease early mortality by improving hemostasis and limiting hemorrhage [21–23]. However, a recent randomized controlled trial in 680 patients with severe trauma and hemorrhage did not confirm these findings [23]. To our knowledge, no studies have evaluated whether pharmacologic strategies can decrease the non-infectious complications of transfusion. Although control of hemorrhage and resuscitation are the most immediate concerns in treating patients with massive bleeding, patients often die from late complications including lung injury, infection, and renal failure.
Allogeneic blood transfusion impairs normal endothelial cell function. One recent study demonstrated that transfusion of RBCs decreases endothelial cell production of nitric oxide within 24 h [24]. Reduced nitric oxide production leads to microvascular vasoconstriction, platelet activation, and enhanced inflammation, all of which may contribute to poor clinical outcomes [25]. We hypothesized that aspirin might be beneficial in massively transfused patients because it has been shown to induce nitric oxide release from endothelial cells and may help to preserve normal endothelial function during transfusion [26]. Aspirin also stimulates anti-inflammatory effects in endothelial cells via histone acetylation, which can decrease monocyte infiltration [27]. Finally, in an animal model of TRALI, aspirin was shown to mitigate lung injury by reducing platelet neutrophil aggregation in the pulmonary circulation [10]. Aspirin may also help to reduce lung injury related to ischemia during CPB. In a previous study of 14 patients having coronary artery bypass surgery, preoperative aspirin use reduced thromboxane production in the lung by approximately 70 % during CPB, suggesting a protective effect [12].
Our results suggest that preoperative aspirin use is associated with fewer mechanical lung ventilation hours in cardiac surgery patients that are massively transfused. It is unclear what mechanism accounts for this potential benefit. One possibility is that preservation of normal endothelial cell function in the lung results in improved ventilation perfusion matching. Alternatively, aspirin’s antiplatelet effects may decrease platelet-neutrophil aggregation in the lung, decreasing the amount of injury and deadspace ventilation. We believe the latter explanation is less likely given that many native platelets with residual aspirin effect are lost in the hemorrhaging patient. The difference in prolonged mechanical ventilation (defined as > 24 h by the STS) that we found could not be explained by early deaths in the aspirin group as there were only 7 patients who died within 24 h of surgery and 3 of them were taking aspirin compared to 4 who were not. The major implication of these findings is that in cardiac surgery patients who are at risk for massive transfusion, it may not be beneficial to stop aspirin before surgery because aspirin use is not associated with increased mortality and it appears to be associated with less mechanical ventilation time. These results should not, however, be extrapolated to all surgical patients as aspirin might be harmful and increase bleeding risk in lower risk surgical patients [16].
The findings of our current study differ from our previous findings in aortic valve replacement surgery patients where preoperative aspirin was not associated with a decreased risk of postoperative ARDS or reduction in mechanical lung ventilation hours [11]. The most likely explanation is that our previous cohort was composed primarily of low risk patients, which was reflected by a low rate of ARDS (5.5 %). This cohort is composed of high risk patients with a high overall mortality rate and much longer median ventilator hours: median ventilator hours in this study; 65 h for aspirin and 89 h for controls vs 15 h for aspirin and 15 h for controls in the prior study.
Our study has a number of limitations. First, the surgical population is heterogeneous because our analysis used patients from a single center and massive transfusion is an infrequent event. Because of this heterogeneity, it is possible that there were systematic differences in the exposure and control groups leading to bias in our risk estimates. There may also have been heterogeneity in mechanical lung ventilation practice during the study period. Secondly, aspirin use is recorded in the STS database dichotomously as having been taken within 5 days of surgery and we had no specific information about dose or time of last administration. Therefore, we cannot say when the optimal time frame for drug administration would be or what an optimal dose would be. In our study we assumed that patients had residual aspirin effect because its typical effect is 7–10 days in platelets. However, for platelet independent mechanisms (e.g. endothelial cells), the duration of action is less clear. Because our study is observational we cannot determine causality. There could be unobserved confounders that were left out of the model and certain variables such as statin use and dyslipidemia could not be balanced in the available dataset despite using propensity score matching. Finally, our findings may not be generalizable to all cardiac surgery patients or non-cardiac surgery patients.
The main strength of our study is that it examined a large cohort of massively transfused cardiac surgery patients from a single center, which has a relatively consistent practice. Also, to our knowledge, there are no previous clinical data suggesting pulmonary benefits from a pharmacologic agent in massively transfused patients. Other agents have been shown to reduce morbidity in massively transfused cardiac surgery patients, but this is primarily through reduced bleeding (e.g.: antifibrinolytics and rFVIIa). Results have been inconsistent with these agents though, depending on the population studied. There are also persistent safety concerns including renal failure with aprotinin and arterial and venous thromboses with rFVIIa [28–30]. Some studies have suggested that perioperative aspirin use may be associated with increased risks of transfusion and bleeding, but in massively transfused patients the contribution to bleeding is probably minimal. In addition, all patients in our cohort received antifibrinolytics which have been shown to mitigate the increased bleeding risks from aspirin [31].
In summary, in a single center propensity score matched cohort of massively transfused cardiac surgery patients, preoperative aspirin use was not associated with a decreased risk of in-hospital mortality. However, patients taking aspirin had less mechanical lung ventilation time and fewer ICU hours. Our findings should be confirmed in a large dataset, due to the importance of the clinical question and potential risks for bleeding with aspirin.
References
Turan A, Yang D, Bonilla A, Shiba A, Sessler DI, Saager L, Kurz A. Morbidity and mortality after massive transfusion in patients undergoing non-cardiac surgery. Can J Anaesth. 2013;60(8):761–70.
Ortmann E, Besser MW, Klein AA. Antifibrinolytic agents in current anaesthetic practice. Br J Anaesth. 2013;111:549–63.
Dhir A. Antifibrinolytics in cardiac surgery. Ann Card Anaesth. 2013;16(2):117–25.
Simmons J, Sikorski RA, Pittet JF. Tranxeamic acid: from trauma to routine perioperative use. Curr Opin Anestheiol. 2015;28:191–200.
Karkouti K, O’Farrell R, Yau TM, Beattie WS. Prediction of massive blood transfusion in cardiac surgery. Can J Anaesth. 2006;53(8):781–94.
Karkouti K, Wijeysundera DN, Yau TM, Beattie WS, Abdelnaem E, McCluskey SA. The independent association of massive blood loss with mortality in cardiac surgery. Transfusion. 2004;44(10):1453–62.
de Christo Dorneles C, Bodanese LC, da Costa Guaragna JCV, Macagnan FE, de Christo Dorneles C, Coelho JC, Borges AP, Goldani MA, Petracco JB. The impact of blood transfusion on morbidity and mortality after cardiac surgery. Rev Bras Cir Cardiovasc. 2011;26(2):222–9.
Losche W, Boettel J, Kabisch B, Winning J, Claus RA, Bauer M. Do aspirin and other antiplatelet drugs reduce the mortality in critically ill patients. Thrombosis 2012;720254.
Kor DJ, Erlich J, Gong M, Malinchoc M, Carter R, Gajic O, Talmor D. Association of pre-hospitalization aspirin therapy and acute lung injury: results of a multicenter international observational study of at-risk-patients. Crit Care Med. 2011;39(11):2393–400.
Looney MR, Nguyen JX, Hu Y, VanZiffle JA, Lowell CA, Matthay MA. Platelet depletion and aspirin treatment protect mice in a two-event model of transfusion related acute lung injury. J Clin Invest. 2009;119(11):3450–61.
Mazzeffi M, Kassa W, Gammie J, Tanaka K, Roman P, Zhan M, Griffith B, Rock P. Preoperative aspirin use and lung injury after aortic valve replacement surgery: a retrospective cohort study. Anesth Analg. 2015;121(2):271–7.
Erez E, Erman A, Snir E, Raanani E, Abramov D, Sulkes J, Boner G, Vidne BA. Thromboxane production in human lung during cardiopulmonary bypass: beneficial effect of aspirin? Ann Thorac Surg. 1998;65(1):101–6.
Gerrah R, Elami A, Stamler A, Smirnov A, Stoeger Z. Preoperative aspirin administration improves oxygenation in patients undergoing coronary artery bypass grafting. Chest. 2005;127(5):1622–6.
Goldhammer JE, Marhefka GD, Daskalakis C, Berguson MW, Bowen JE, Diehl JT, Sun J. The effect of aspirin on bleeding and transfusion in contemporary cardiac surgery. PLoS ONE. 2015;10(7):e0134670.
Alghamdi AA, Moussa F, Fremes SE. Does the use of preoperative aspirin increase the risk of bleeding in patients undergoing coronary artery bypass grafting surgery? Systematic review and meta-analysis. J Card Surg. 2007;22(3):247–56.
POISE-2 investigators: aspirin in patients undergoing noncardiac surgery. New Engl J Med 2014;370:1494–1503.
Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav Res. 2011;46(3):399–424.
Garrido MM, Kelley AS, Paris J, Roza K, Meier DE, Morrison RS, Aldridge MD. Methods for constructing and assessing propensity scores. Health Serv Res. 2014;49(5):1701–20.
D’Agostino RB. Propensity scores in cardiovascular research. Circulation. 2007;115:2340–3.
Coca-Perraillon M. Local and global optimal propensity score matching. SAS global forum, statistics and data analysis 2007:1–9.
Holcolmb J, del Junco DJ, Fox EE, Wade CE, Cohen MJ, Schreiber MA, Alarcon LH, Bai Y, Brasel KJ, Bulger EM, Cotton BA, Matijevic N, Muskat P, Myers JG, Phelan HA, White CE, Zhang J, Rahbar MH. The prospective observational multicenter major trauma transfusion (PROMMTT) study: comparative effectiveness of a time-varying treatment with competing risks. JAMA Surg. 2013;148(2):127–36.
Borgman MA, Spinella PC, Holcolmb JB, Blackbourne LH, Wade CE, Lefering R, Bouillon B, Maegele M. The effect of FFP:RBC ratio on morbidity and mortality in trauma patients based on transfusion prediction score. Vox Sang. 2011;101(1):44–54.
PROPRR Study Group. Transfusion of plasma, platelets, and red blood cells in a 1:1:1 vs. a 1:1:2 ratio and mortality in patients with severe trauma: the PROPRR randomized clinical trial. JAMA. 2015;313(5):471–82.
Neuman R, Hayek S, Rahman A, Poole JC, Menon V, Sher S, Newman JL, Karatela S, Polhemus D, Lefer DJ, De Staercke C, Hooper C, Quyyumi AA, Roback JD. Effects of storage-aged red blood cell transfusions on endothelial function in hospitalized patients. Transfusion. 2014;55(4):782–90.
Roback JD. Vascular effects of the red blood cell storage lesion. Hematology Am Soc Hematol Educ Program 2011;475–9.
Taubert D, Berkels R, Grosser N, Schroder H, Grundemann D, Schomig E. Aspirin induces nitric oxide release from vascular endothelium: a novel mechanism of action. Br J Pharmacol. 2004;143(1):159–65.
Passacquale G, Phinikaridou A, Warboys C, Cooper M, Lavin B, Alfieri A, Andia ME, Botnar RM, Ferro A. Aspirin induced histone acetylation in endothelial cells enhances synthesis of the secreted isoform of netrin-1 thus inhibiting monocyte vascular infiltration. Brit J Pharm. 2015;172:3548–64.
Umscheid CA, Kohl BA, Williams K. Antifibrinolytic use in adult cardiac surgery. Curr Opin Hematol. 2007;14:455–67.
Zangrillo A, Mizzi A, Biondi-Zoccai G, Bignami E, Calabro MG, Pappalardo F, Dedola E, Tritapepe L, Marino G, Landoni G. Recombinant activated factor VII in cardiac surgery: a meta-analysis. J Cardiothorac Vasc Anesth. 2009;23(1):34–40.
Levi M, Levy JH, Andersen HF, Truloff DT. Safety of recombinant activated factor VII in randomized clinical trials. N Engl J Med. 2010;363:1791–800.
McIlroy DR, Myles PS, Phillips LE, Smith JA. Antifibrinolytics in cardiac surgical patients receiving aspirin: a systematic review and meta-analysis. Br J Anaesth. 2009;102(2):168–78.
Acknowledgments
We would like to acknowledge Filiz Constantini for helping to supply the STS data for this study.
Author information
Authors and Affiliations
Corresponding author
About this article

Cite this article
Mazzeffi, M., Galvagno, S., Gammie, J.S. et al. Impact of aspirin use on morbidity and mortality in massively transfused cardiac surgery patients: a propensity score matched cohort study. J Anesth 30, 817–825 (2016). https://doi.org/10.1007/s00540-016-2213-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00540-016-2213-2