
Abstract
Background
In a group of children admitted to the paediatric intensive care unit (PICU) receiving continuous kidney replacement therapy (CKRT), we aim to evaluate the data about their hemodynamic, ventilation and analgo-sedation profile in the first 24 h of treatment and possible associations with mortality.
Methods
Retrospective cohort study of children admitted to the PICU of the University Hospital of Padova undergoing CKRT between January 2011 and March 2021. Data was collected at baseline (T0), after 1 h (T1) and 24 h (T24) of CKRT treatment. The differences in outcome measures were compared between these time points, and between survivors and non-survivors.
Results
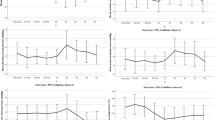
Sixty-nine patients received CKRT, of whom 38 (55%) died during the PICU stay. Overall, the vasoactive inotropic score and the adrenaline dose increased at T1 compared to T0 (p = 0.012 and p = 0.022, respectively). Compared to T0, at T24 patients showed an improvement in the following ventilatory parameters: Oxygenation Index (p = 0.005), Oxygenation Saturation Index (p = 0.013) PaO2/FiO2 ratio (p = 0.005), SpO2/FiO2 ratio (p = 0.002) and Mean Airway Pressure (p = 0.016). These improvements remained significant in survivors (p = 0.01, p = 0.027, p = 0.01 and p = 0.015, respectively) but not in non-survivors. No changes in analgo-sedative drugs have been described.
Conclusions
CKRT showed a significant impact on hemodynamics and ventilation in the first 24 h of treatment. We observed a significant rise in the inotropic/vasoactive support required after 1 h of treatment in the overall population, and an improvement in the ventilation parameters at 24 h only in survivors.
Graphical abstract

A higher resolution version of the Graphical abstract is available as Supplementary information
Similar content being viewed by others


Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on request.
References
Kaddourah A, Basu RK, Bagshaw SM, Goldstein SL (2017) Epidemiology of acute kidney injury in critically ill children and young adults. N Engl J Med 376:11–20. https://doi.org/10.1056/NEJMoa1611391
Kwiatkowski DM, Sutherland SM (2017) Acute kidney injury in pediatric patients. Best Pract Res Clin Anaesthesiol 31:427–439. https://doi.org/10.1016/j.bpa.2017.08.007
Goldberg R, Dennen P (2008) Long-term outcomes of acute kidney injury. Adv Chronic Kidney Dis 15:297–307. https://doi.org/10.1053/j.ackd.2008.04.009
Boschee ED, Cave DA, Garros D et al (2014) Indications and outcomes in children receiving renal replacement therapy in pediatric intensive care. J Crit Care 29:37–42. https://doi.org/10.1016/j.jcrc.2013.09.008
de Galasso L, Picca S, Guzzo I (2020) Dialysis modalities for the management of pediatric acute kidney injury. Pediatr Nephrol 35:753–765. https://doi.org/10.1007/s00467-019-04213-x
Goldstein SL, Somers MJG, Baum MA et al (2005) Pediatric patients with multi-organ dysfunction syndrome receiving continuous renal replacement therapy. Kidney Int 67:653–658. https://doi.org/10.1111/j.1523-1755.2005.67121.x
van Bommel E, Bouvy ND, So KL et al (1995) Acute dialytic support for the critically ill: intermittent hemodialysis versus continuous arteriovenous hemodiafiltration. Am J Nephrol 15:192–200. https://doi.org/10.1159/000168832
Yetimakman AF, Kesici S, Tanyildiz M et al (2019) A report of 7-year experience on pediatric continuous renal replacement therapy. J Intensive Care Med 34:985–989. https://doi.org/10.1177/0885066617724339
Westrope CA, Fleming S, Kapetanstrataki M et al (2018) Renal replacement therapy in the critically Ill child. Pediatr Crit Care Med 19:210–217. https://doi.org/10.1097/PCC.0000000000001431
Palmieri TL (2010) Complications of continuous renal replacement therapy in children: are all created equal? Crit Care 14:105. https://doi.org/10.1186/cc8229
Goldstein SL (2011) Continuous renal replacement therapy: mechanism of clearance, fluid removal, indications and outcomes. Curr Opin Pediatr 23:181–185. https://doi.org/10.1097/MOP.0b013e328342fe67
Gorga SM, Sahay RD, Askenazi DJ et al (2020) Fluid overload and fluid removal in pediatric patients on extracorporeal membrane oxygenation requiring continuous renal replacement therapy: a multicenter retrospective cohort study. Pediatr Nephrol 35:871–882. https://doi.org/10.1007/s00467-019-04468-4
Arikan AA, Zappitelli M, Goldstein SL et al (2012) Fluid overload is associated with impaired oxygenation and morbidity in critically ill children. Pediatr Crit Care Med 13:253–258. https://doi.org/10.1097/PCC.0b013e31822882a3
Payen D, de Pont AC, Sakr Y et al (2008) A positive fluid balance is associated with a worse outcome in patients with acute renal failure. Crit Care 12:R74. https://doi.org/10.1186/cc6916
Joannidis M, Forni LG, Klein SJ et al (2020) Lung-kidney interactions in critically ill patients: consensus report of the acute disease quality initiative (ADQI) 21 workgroup. Intensive Care Med 46:654–672. https://doi.org/10.1007/s00134-019-05869-7
Yang W, Hong J, Zeng Q et al (2016) Improvement of oxygenation in severe acute respiratory distress syndrome with high-volume continuous Veno-venous hemofiltration. Glob Pediatr Health 3:2333794X16645699. https://doi.org/10.1177/2333794X16645699
Douvris A, Zeid K, Hiremath S et al (2019) Mechanisms for hemodynamic instability related to renal replacement therapy: a narrative review. Intensive Care Med 45:1333–1346. https://doi.org/10.1007/s00134-019-05707-w
Fernández S, Santiago MJ, González R et al (2019) Hemodynamic impact of the connection to continuous renal replacement therapy in critically ill children. Pediatr Nephrol 34:163–168. https://doi.org/10.1007/s00467-018-4047-7
Schortgen F, Soubrier N, Delclaux C et al (2000) Hemodynamic tolerance of intermittent hemodialysis in critically ill patients: usefulness of practice guidelines. Am J Respir Crit Care Med 162:197–202. https://doi.org/10.1164/ajrccm.162.1.9907098
Thadani S, Fogarty T, Mottes T et al (2022) Hemodynamic instability during connection to continuous kidney replacement therapy in critically ill pediatric patients. Pediatr Nephrol. https://doi.org/10.1007/s00467-022-05424-5
Shawwa K, Kompotiatis P, Jentzer J et al (2019) Hypotension within one-hour from starting CRRT is associated with in-hospital mortality. J Crit Care 54:7–13. https://doi.org/10.1016/j.jcrc.2019.07.004
Thompson AJ (2008) Drug dosing during continuous renal replacement therapies. J Pediatr Pharmacol Ther 13:99–113. https://doi.org/10.5863/1551-6776-13.2.99
Bouajram RH, Awdishu L (2021) A Clinician’s Guide to Dosing Analgesics, Anticonvulsants, and Psychotropic Medications in Continuous Renal Replacement Therapy. Kidney Int Rep 6:2033–2048. https://doi.org/10.1016/j.ekir.2021.05.004
Dubinsky S, Watt K, Saleeb S et al (2022) Pharmacokinetics of commonly used medications in children receiving continuous renal replacement therapy: A systematic review of current literature. Clin Pharmacokinet 61:189–229. https://doi.org/10.1007/s40262-021-01085-z
Bugge JF (2001) Pharmacokinetics and drug dosing adjustments during continuous venovenous hemofiltration or hemodiafiltration in critically ill patients. Acta Anaesthesiol Scand 45:929–934. https://doi.org/10.1034/j.1399-6576.2001.450802.x
Schwartz GJ, Brion LP, Spitzer A (1987) The use of plasma creatinine concentration for estimating glomerular filtration rate in infants, children, and adolescents. Pediatr Clin North Am 34:571–590. https://doi.org/10.1016/s0031-3955(16)36251-4
Schwartz GJ, Muñoz A, Schneider MF et al (2009) New equations to estimate GFR in children with CKD. J Am Soc Nephrol 20:629–637. https://doi.org/10.1681/ASN.2008030287
Gao A, Cachat F, Faouzi M et al (2013) Comparison of the glomerular filtration rate in children by the new revised Schwartz formula and a new generalized formula. Kidney Int 83:524–530. https://doi.org/10.1038/ki.2012.388
Acute Kidney Injury Work Group Kidney Disease: Improving Global Outcomes (KDIGO), KDIGO Clinical Practice Guideline for Acute Kidney Injury. chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://kdigo.org/wp-content/uploads/2016/10/KDIGO-2012-AKI-Guideline-English.pdf. Accessed June 2023
Sutherland SM, Byrnes JJ, Kothari M et al (2015) AKI in hospitalized children: comparing the pRIFLE, AKIN, and KDIGO definitions. Clin J Am Soc Nephrol 10:554–561. https://doi.org/10.2215/CJN.01900214
Selewski DT, Cornell TT, Heung M et al (2014) Validation of the KDIGO acute kidney injury criteria in a pediatric critical care population. Intensive Care Med 40:1481–1488. https://doi.org/10.1007/s00134-014-3391-8
Leteurtre S, Duhamel A, Salleron J et al (2013) PELOD-2: an update of the PEdiatric logistic organ dysfunction score. Crit Care Med 41:1761–1773. https://doi.org/10.1097/CCM.0b013e31828a2bbd
Schlapbach LJ, Straney L, Bellomo R et al (2018) Prognostic accuracy of age-adapted SOFA, SIRS, PELOD-2, and qSOFA for in-hospital mortality among children with suspected infection admitted to the intensive care unit. Intensive Care Med 44:179–188. https://doi.org/10.1007/s00134-017-5021-8
McIntosh AM, Tong S, Deakyne SJ et al (2017) Validation of the vasoactive-inotropic score in pediatric sepsis. Pediatr Crit Care Med 18:750–757. https://doi.org/10.1097/PCC.0000000000001191
Koponen T, Karttunen J, Musialowicz T et al (2019) Vasoactive-inotropic score and the prediction of morbidity and mortality after cardiac surgery. Br J Anaesth 122:428–436. https://doi.org/10.1016/j.bja.2018.12.019
DesPrez K, McNeil JB, Wang C et al (2017) Oxygenation saturation index predicts clinical outcomes in ARDS. Chest 152:1151–1158. https://doi.org/10.1016/j.chest.2017.08.002
Muniraman HK, Song AY, Ramanathan R et al (2019) Evaluation of oxygen saturation index compared with oxygenation index in neonates with hypoxemic respiratory failure. JAMA Netw Open 2:e191179. https://doi.org/10.1001/jamanetworkopen.2019.1179
Thomas NJ, Shaffer ML, Willson DF et al (2010) Defining acute lung disease in children with the oxygenation saturation index. Pediatr Crit Care Med 11:12–17. https://doi.org/10.1097/PCC.0b013e3181b0653d
Marini JJ, Ravenscraft SA (1992) Mean airway pressure: physiologic determinants and clinical importance–Part 1: Physiologic determinants and measurements. Crit Care Med 20:1461–1472
Marini JJ, Ravenscraft SA (1992) Mean airway pressure: physiologic determinants and clinical importance–Part 2: Clinical implications. Crit Care Med 20:1604–1616
Sahetya SK, Wu TD, Morgan B et al (2020) Mean airway pressure as a predictor of 90-day mortality in mechanically ventilated patients. Crit Care Med 48:688–695. https://doi.org/10.1097/CCM.0000000000004268
Benjamini Y, Hochberg Y (1995) Controlling the false discovery rate: a practical and powerful approach to multiple testing. J Roy Stat Soc: Ser B (Methodol) 57:289–300. https://doi.org/10.1111/j.2517-6161.1995.tb02031.x
Harris PA, Taylor R, Minor BL et al (2019) The REDCap consortium: Building an international community of software platform partners. J Biomed Inform 95:103208. https://doi.org/10.1016/j.jbi.2019.103208
R Core Team (2020) R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. https://www.R-project.org/
Steyerberg EW (2016) Frank E. Harrell, Jr., Regression modeling strategies: With applications, to linear models, logistic and ordinal regression, and survival analysis, 2nd ed. Heidelberg: Springer. Biometrics 72:1006–1007. https://doi.org/10.1111/biom.12569
Alobaidi R, Morgan C, Basu RK et al (2018) Association between fluid balance and outcomes in critically Ill children: A systematic review and meta-analysis. JAMA Pediatr 172:257–268. https://doi.org/10.1001/jamapediatrics.2017.4540
Mehta RL (2009) Fluid balance and acute kidney injury: the missing link for predicting adverse outcomes? Nat Clin Pract Nephrol 5:10–11. https://doi.org/10.1038/ncpneph0988
Acknowledgements
We thank Nadia Coscini for her help in extensively reviewing the English grammar and syntax throughout the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors report no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Imberti, S., Comoretto, R., Ceschia, G. et al. Impact of the first 24 h of continuous kidney replacement therapy on hemodynamics, ventilation, and analgo-sedation in critically ill children. Pediatr Nephrol 39, 879–887 (2024). https://doi.org/10.1007/s00467-023-06155-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-023-06155-x