
Abstract
Background
Telemedicine has been shown to improve patient access to medical care while potentially improving overall healthcare efficiency. It has not been consistently explored on an acute care surgery service as a method of increasing clinic availability and efficiency within a safety-net hospital system. Socioeconomic hardships associated with an in-person clinic visit can deter patients with limited resources. A virtual clinic for post-operative laparoscopic cholecystectomy patients was developed. We hypothesized that a virtual follow-up increases clinic efficiency and availability for new patients without compromising patient safety.
Methods
A retrospective review of patient and clinic outcomes before and after implementing virtual post-op visits for uncomplicated laparoscopic cholecystectomy patients on an acute care surgery service was performed. Providers called post-operative patients using a standardized questionnaire. Data included outpatient clinic composition (new vs. post-operative patients), elective operations scheduled, emergency department visits, and loss to follow-up rates.
Results
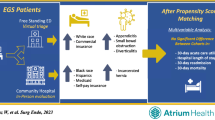
February to March 2017 was the baseline pre-intervention period, while February to March 2019 was post-intervention. Pre-intervention clinics consisted of 17% new and 50% post-op visits, in comparison to 31% new and 27% post-op visits in the post-intervention group (p < 0.01). Elective operations scheduled increased slightly from 8.4 to 11.5 per 100 patient visits, but was not statistically significant (p = 0.09). There was no change in the number of post-operative patients returning to the emergency department (p = 0.91) or loss to follow-up (p = 0.30) rates.
Conclusions
Through the implementation of virtual post-operative visits for laparoscopic cholecystectomy patients, clinic efficiency improved by increasing new patient encounters, decreasing post-operative volume, and trending towards increased operations scheduled. This change did not compromise patient safety. Further implementation of telemedicine on an acute care surgery service is a promising method to expand services offered to an at-risk population and increase efficiency in a resource-limited environment.

Similar content being viewed by others


References
Kvedar J, Coye MJ, Everett W (2014) Connected health: a review of technologies and strategies to improve patient care with telemedicine and telehealth. Health Aff (Millwood) 33(2):194–199
Lesher AP, Shah SR (2018) Telemedicine in the perioperative experience. Semin Pediatr Surg 27(2):102–106
Harting MT, Wheeler A, Ponsky T, Nwomeh B, Snyder CL, Bruns NE, Lesher A, Pandya S, Dickie B, Shah SR, for the APSA Informatics, and Telemedicine Committee, (2019) Telemedicine in pediatric surgery. J Pediatr Surg 54(3):587–594
Gunter RL, Chouinard S, Fernandes-Taylor S, Wiseman JT, Clarkson S, Bennett K, Greenberg CC, Kent KC (2016) Current use of telemedicine for post-discharge surgical care: A systematic review. J Am Coll Surg 222(5):915–927
Acknowledgments
All residents and advanced practice providers on the Emergency General Surgery Service who conducted the virtual visits. Mohsin Ahmad and Tai Nguyen for collecting and validating the data. All residents, hospital staff, clinic staff, advanced practice providers and faculty who have been involved in the establishment and continual improvement of the Virtual Post-Op Clinic at Parkland Memorial Hospital.
Funding
No sources to disclose.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Drs. Parnell, Kuhlenschmidt, Madni, Scott, Oltmann, Luk and Ms. Chernyakhovsky, Donovan, Garofalo, and Hambrick have no conflicts of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Parnell, K., Kuhlenschmidt, K., Madni, D. et al. Using telemedicine on an acute care surgery service: improving clinic efficiency and access to care. Surg Endosc 35, 5760–5765 (2021). https://doi.org/10.1007/s00464-020-08055-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-020-08055-9