
Abstract
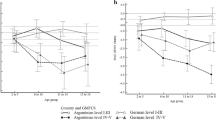
The purpose of this study was to create growth-percentiles for Caucasian children with cerebral palsy (CP). The studied parameters were height and age. In a retrospective analysis, we converted measurements collected in our center to create disorder-specific percentiles of normative data. Patients were stratified due to sex (male and female) and to mobility levels using the gross motor function classification system (GMFCS) (A = walking; GMFCS I–III, B = non walking; GMFCS IV–V) into four groups. In total, 2363 measurements in patients 0–18 years were collected. The mean age for group “Am” was 6.8 years (n = 862), group “Bm” 7.6 years (n = 563), group “Af” 7.7 years (n = 600), and group “Bf” 8.2 years (n = 366). The created percentiles for all groups were below the reference percentiles for healthy Caucasian children (KiGGS). The median curve for children with GMFCS levels I–III is slightly above the 3rd percentile, whereas the 50th percentile for GMFCS levels IV–V is mostly below the 3rd KiGGS centile.
Conclusion: In conclusion, children with cerebral palsy are smaller than healthy children. The difference between 50th percentile of CP patients compared to healthy children supports the need for the use of disorder-specific growth charts. Those charts can help clinicians differentiate growth disorders in patients with CP.
What is Known: | |
• Children with cerebral palsy are shorter than healthy children and height is influenced by level of ambulation. | |
• Currently, only reference percentiles of American children with mixed ethical backgrounds are available to evaluate growth. | |
What is New: | |
• This paper presents disorder-specific reference percentiles for longitudinal growth of Caucasian children with cerebral palsy depending on motor function. | |
• These percentiles allow to asses longitudinal growth in children with cerebral palsy to detect other additional diseases impairing growth. |




Similar content being viewed by others


Abbreviations
- CP:
-
Cerebral palsy
- IGF-1:
-
Insulin-like growth factor
- LEP:
-
Life Expectancy Project
- GMFCS:
-
Gross motor function classification system
References
Bonthuis M, van Stralen KJ, Verrina E, Edefonti A, Molchanova EA, Hokken-Koelega ACS, Schaefer F, Jager KJ (2012) Use of national and international growth charts for studying height in European children: development of up-to-date European height-for-age charts. PLoS One 7(8):e42506
Brooks J. Life Expectancy Project 2011 [Available from: http://www.lifeexpectancy.org/articles/NewGrowthCharts/All.pdf]. Accessed January 2018
Brooks J, Day S, Shavelle R, Strauss D (2011) Low weight, morbidity, and mortality in children with cerebral palsy: new clinical growth charts. Pediatrics 128(2):e299–e307
Butler MG, Lee J, Manzardo AM, Gold JA, Miller JL, Kimonis V, Driscoll DJ (2015) Growth charts for non-growth hormone treated Prader-Willi syndrome. Pediatrics. 135(1):e126–e135
Christesen HT, Pedersen BT, Pournara E, Petit IO, Júlíusson PB (2016) Short stature: comparison of WHO and national growth standards/references for height. PLoS One 11(6):e0157277
Cole TJ, Green PJ (1992) Smoothing reference centile curves: the LMS method and penalized likelihood. Stat Med 11(10):1305–1319
Day SM, Strauss DJ, Vachon PJ, Rosenbloom L, Shavelle RM, Wu YW (2007) Growth patterns in a population of children and adolescents with cerebral palsy. Dev Med Child Neurol 49(3):167–171
Finbraten AK, Syversen U, Skranes J, Andersen GL, Stevenson RD, Vik T (2015) Bone mineral density and vitamin D status in ambulatory and non-ambulatory children with cerebral palsy. Osteoporos Int 26(1):141–150
Frost HM (1997) Biomechanical control of knee alignment: some insights from a new paradigm. Clin Orthop Relat Res 335:335–342
Fung EB, Samson-Fang L, Stallings VA, Conaway M, Liptak G, Henderson RC et al (2002) Feeding dysfunction is associated with poor growth and health status in children with cerebral palsy. J Am Diet Assoc 102(3):361–373
Indrayan A (2014) Demystifying LMS and BCPE methods of centile estimation for growth and other health parameters. Indian Pediatr 51(1):37–43
Kim JS, Han ZA, Song DH, Oh HM, Chung ME (2013) Characteristics of dysphagia in children with cerebral palsy, related to gross motor function. Am J Phys Med Rehabil 92(10):912–919
Krick J, Van Duyn MA (1984) The relationship between oral-motor involvement and growth: a pilot study in a pediatric population with cerebral palsy. J Am Diet Assoc 84(5):555–559
Krick J, Murphy-Miller P, Zeger S, Wright E (1996) Pattern of growth in children with cerebral palsy. J Am Diet Assoc 96(7):680–685
Neuhauser H SA, Schaffrath-Rosario A, Dortschy R, Kurth BM (2013) Referenzperzentile für anthropometrische Maßzahlen und Blutdruck aus der Studie zur Gesundheit von Kindern und Jugendlichen in Deutschland (KiGGS). Gesundheitsberichterstattung des Bundes. Gesundheitsberichterstattung des Bundes: Robert-Koch-Institut; 2013
Oftedal S, Davies PSW, Boyd RN, Stevenson RD, Ware RS, Keawutan P, Benfer KA, Bell KL (2016) Longitudinal growth, diet, and physical activity in young children with cerebral palsy. Pediatrics. 138:e20161321
Palisano R, Rosenbaum P, Walter S, Russell D, Wood E, Galuppi B (1997) Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev Med Child Neurol 39(4):214–223
Ranke MB, Pflüger H, Rosendahl W, Stubbe P, Enders H, Bierich JR et al (1983) Turner syndrome: spontaneous growth in 150 cases and review of the literature. Eur J Pediatr 141(2):81–88
Reilly S, Skuse D (1992) Characteristics and management of feeding problems of young children with cerebral palsy. Dev Med Child Neurol 34(5):379–388
Rigby RA, Stasinopoulos DM (2013) Automatic smoothing parameter selection in GAMLSS with an application to centile estimation. Stat Methods Med Res 23(4):318–332
Rivkees SA, Bode HH, Crawford JD (1988) Long-term growth in juvenile acquired hypothyroidism: the failure to achieve normal adult stature. N Engl J Med 318(10):599–602
Robson H, Siebler T, Shalet SM, Williams GR (2002) Interactions between GH, IGF-I, glucocorticoids, and thyroid hormones during skeletal growth. Pediatr Res 52(2):137–147
Rogol AD, Clark PA, Roemmich JN (2000) Growth and pubertal development in children and adolescents: effects of diet and physical activity. Am J Clin Nutr 72(2 Suppl):521s–528S
Rosenbaum P, Paneth N, Leviton A, Goldstein M, Bax M, Damiano D et al (2007) A report: the definition and classification of cerebral palsy April 2006. Developmental medicine and child neurology. Supplement. 109:8–14
Royston P (1991) Constructing time-specific reference ranges. Stat Med 10(5):675–690
Royston P, Wright EM (2000) Goodness-of-fit statistics for age-specific reference intervals. Stat Med 19(21):2943–2962
Shapiro BK, Green P, Krick J, Allen D, Capute AJ (1986) Growth of severely impaired children: neurological versus nutritional factors. Dev Med Child Neurol 28(6):729–733
Sterling HM (1960) Height and weight of children with cerebral palsy and acquired brain damage. Arch Phys Med Rehabil 41:131–135
Stevenson RD, Conaway M, Chumlea WC, Rosenbaum P, Fung EB, Henderson RC, Worley G, Liptak G, O’Donnell M, Samson-Fang L, Stallings VA, of the North American Growth in Cerebral Palsy Study (2006) Growth and health in children with moderate-to-severe cerebral palsy. Pediatrics. 118(3):1010–1018
Surveillance of Cerebral Palsy in E (2000) Surveillance of cerebral palsy in Europe: a collaboration of cerebral palsy surveys and registers. Surveillance of cerebral palsy in Europe (SCPE). Dev Med Child Neurol 42(12):816–824
Tobis JS, Saturen P, Larios G, Posniak AO (1961) Study of growth patterns in cerebral palsy. Arch Phys Med Rehabil 42:475–481
van Buuren S, Fredriks M (2001) Worm plot: a simple diagnostic device for modelling growth reference curves. Stat Med 20(8):1259–1277
van der Eerden BC, Karperien M, Wit JM (2003) Systemic and local regulation of the growth plate. Endocr Rev 24(6):782–801
Zonta MB, Ramalho-Junior A, Puppi M, Bruck I, Magdalena N, Muzzolon SR et al (2014) Side-to-side growth discrepancies in children with hemiplegic cerebral palsy: association with function, activity and social participation. Arq Neuropsiquiatr 72(5):360–367
Funding
This study was supported by the Koeln Fortune Program/Faculty of Medicine, University of Cologne by a thesis grant to PE and by a research grant from IPSEN PHARMA GmbH. The sponsor was not involved in the study design, collection, analysis, and interpretation of data or writing of the report. The decision to submit the paper was exclusively done by the authors without any involvement of the sponsors. The data was not presented before.
Author information
Authors and Affiliations
Contributions
PE, OS and ES designed the research project. PE KM, CS, ID and OS collected the data and OS, SH and ID performed the statistical analysis. ID, CS, KM ES and OS cared for the patients. EP, SH and OS drafted the manuscript. All authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This study was approved by the ethics committee of the University of Cologne (15-241).
Additional information
Communicated by Peter de Winter
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Egenolf, P., Duran, I., Stark, C. et al. Development of disorder-specific normative data for growth in children with cerebral palsy. Eur J Pediatr 178, 811–822 (2019). https://doi.org/10.1007/s00431-019-03360-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-019-03360-5