
Abstract
Background and Objective
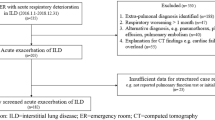
Despite the high mortality of acute exacerbations of interstitial lung disease (AE-ILD), there is minimal evidence to guide management decisions. We aimed to assess the feasibility and outcomes of a standardized management protocol for AE-ILD.
Methods
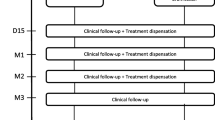
We performed a retrospective cohort study of patients with AE-ILD admitted to hospital between January 2015 and August 2019. Patients were managed with a standardized protocol including chest computed tomography (CT) at diagnosis, pulse corticosteroid treatment, and a follow-up CT 7 days after corticosteroid pulse. The association between idiopathic pulmonary fibrosis (IPF) versus non-IPF diagnosis and transplant-free survival within 1-year of AE-ILD was assessed using adjusted Cox proportional hazards regression survival analysis. Associations with CT chest improvement 7 days after corticosteroid pulse were secondarily assessed.
Results
89 patients with AE-ILD were identified. 1-year transplant-free and overall survival were 20.2 and 51.7%, respectively. Protocol adherence to pulse corticosteroids was high (95.5%). A diagnosis of IPF was associated with higher risk of death or transplant at 1-year versus a non-IPF diagnosis [hazard ratio (HR) 2.23, 95% CI 1.19–4.17, p = 0.012]. There were no significant associations with 7-day CT improvement; however, CT improvement was associated with higher transplant-free survival (p = 0.02) and a lower risk of in-hospital mortality (χ2 = 7.06, p = 0.01) on unadjusted analysis.
Conclusions
IPF is associated with a higher risk of death or transplant at 1-year as compared to a non-IPF diagnosis in patients with AE-ILD managed using a standardized protocol. Improvement on CT chest 7 days after corticosteroid pulse is associated with better survival.


Similar content being viewed by others

Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request and approval by applicable research ethics board.
Abbreviations
- AE:
-
Acute exacerbation
- CCI:
-
Charlson comorbidity index
- CHP:
-
Chronic hypersensitivity pneumonitis
- CI:
-
Confidence interval
- CT:
-
Computed tomography
- CTD:
-
Connective tissue disease
- DLco:
-
Diffusing capacity of carbon monoxide
- FVC:
-
Forced vital capacity
- GVHD:
-
Graft versus host disease
- HR:
-
Hazard ratio
- ILD:
-
Interstitial lung disease
- IPAF:
-
Idiopathic pneumonia with autoimmune features
- IPF:
-
Idiopathic pulmonary fibrosis
- IQR:
-
Interquartile range
- MDD:
-
Multidisciplinary discussion
- NSIP:
-
Non-specific interstitial pneumonia
- PPI:
-
Proton pump inhibitor
- 6MWD:
-
6-Minute walk test distance
References
Ley B, Collard HR, King TE Jr (2011) Clinical course and prediction of survival in idiopathic pulmonary fibrosis. Am J Respir Crit Care Med 183(4):431–440
Song JW et al (2011) Acute exacerbation of idiopathic pulmonary fibrosis: incidence, risk factors and outcome. Eur Respir J 37(2):356–363
Kolb M et al (2018) Acute exacerbations of progressive-fibrosing interstitial lung diseases. Eur Respir Rev 27(150):180071
Toyoda Y et al (2016) Clinical features and outcome of acute exacerbation of interstitial pneumonia associated with connective tissue disease. J Med Invest 63(3–4):294–299
Tachikawa R et al (2012) Clinical features and outcome of acute exacerbation of interstitial pneumonia: collagen vascular diseases-related versus idiopathic. Respiration 83(1):20–27
Cao M et al (2019) Acute exacerbations of fibrosing interstitial lung disease associated with connective tissue diseases: a population-based study. BMC Pulm Med 19(1):215
Enomoto N et al (2019) Differences in clinical features of acute exacerbation between connective tissue disease-associated interstitial pneumonia and idiopathic pulmonary fibrosis. Chron Respir Dis 16:1479972318809476
Murohashi K et al (2019) Clinical significance of Charlson comorbidity index as a prognostic parameter for patients with acute or subacute idiopathic interstitial pneumonias and acute exacerbation of collagen vascular diseases-related interstitial pneumonia. J Thorac Dis 11(6):2448–2457
Suzuki A et al (2020) Acute exacerbations of fibrotic interstitial lung diseases. Respirology 25(5):525–534
Salonen J et al (2020) Prognosis and causes of death of patients with acute exacerbation of fibrosing interstitial lung diseases. BMJ Open Respir Res 7(1):563
Takei R et al (2017) Impact of lymphocyte differential count > 15% in BALF on the mortality of patients with acute exacerbation of chronic fibrosing idiopathic interstitial pneumonia. BMC Pulm Med 17(1):67
Collard HR et al (2016) acute exacerbation of idiopathic pulmonary fibrosis. An international working group report. Am J Respir Crit Care Med 194(3):265–275
Raghu G et al (2015) An official ATS/ERS/JRS/ALAT clinical practice guideline: Treatment of idiopathic pulmonary fibrosis. An update of the 2011 clinical practice guideline. Am J Respir Crit Care Med 192(2):e3-19
Novelli L et al (2016) Corticosteroid and cyclophosphamide in acute exacerbation of idiopathic pulmonary fibrosis: a single center experience and literature review. Sarcoidosis Vasc Diffuse Lung Dis 33(4):385–391
Arai T et al (2017) High-dose prednisolone after intravenous methylprednisolone improves prognosis of acute exacerbation in idiopathic interstitial pneumonias. Respirology 22(7):1363–1370
Papiris SA et al (2015) Survival in Idiopathic pulmonary fibrosis acute exacerbations: the non-steroid approach. BMC Pulm Med 15:162
Atkins CP, Loke YK, Wilson AM (2014) Outcomes in idiopathic pulmonary fibrosis: a meta-analysis from placebo controlled trials. Respir Med 108(2):376–387
Raghu G et al (2011) An official ATS/ERS/JRS/ALAT statement: idiopathic pulmonary fibrosis: evidence-based guidelines for diagnosis and management. Am J Respir Crit Care Med 183(6):788–824
Raghu G et al (2018) Diagnosis of idiopathic pulmonary fibrosis. An official ATS/ERS/JRS/ALAT clinical practice guideline. Am J Respir Crit Care Med 198(5):e44–e68
Landis JR, Koch GG (1977) The measurement of observer agreement for categorical data. Biometrics 33(1):159–174
Abe S et al (2012) Polymyxin B-immobilized fiber column (PMX) treatment for idiopathic pulmonary fibrosis with acute exacerbation: a multicenter retrospective analysis. Intern Med 51(12):1487–1491
Simon-Blancal V et al (2012) Acute exacerbation of idiopathic pulmonary fibrosis: outcome and prognostic factors. Respiration 83(1):28–35
Arai T et al (2016) Heterogeneity of incidence and outcome of acute exacerbation in idiopathic interstitial pneumonia. Respirology 21(8):1431–1437
Kato M et al (2019) Prognostic differences among patients with idiopathic interstitial pneumonias with acute exacerbation of varying pathogenesis: a retrospective study. Respir Res 20(1):287
Al-Hameed FM, Sharma S (2004) Outcome of patients admitted to the intensive care unit for acute exacerbation of idiopathic pulmonary fibrosis. Can Respir J 11(2):117–122
Leuschner G, Behr J (2017) Acute exacerbation in interstitial lung disease. Front Med 4:176
Kim DS et al (2006) Acute exacerbation of idiopathic pulmonary fibrosis: frequency and clinical features. Eur Respir J 27(1):143–150
Hariri LP et al (2010) Acute fibrinous and organizing pneumonia in systemic lupus erythematosus: a case report and review of the literature. Pathol Int 60(11):755–759
Hariri LP et al (2012) Distinct histopathology of acute onset or abrupt exacerbation of hypersensitivity pneumonitis. Hum Pathol 43(5):660–668
Prahalad S et al (2005) Fatal acute fibrinous and organizing pneumonia in a child with juvenile dermatomyositis. J Pediatr 146(2):289–292
Muir TE et al (1997) Organizing diffuse alveolar damage associated with progressive systemic sclerosis. Mayo Clin Proc 72(7):639–642
Kitaichi M (1990) Pathologic features and the classification of interstitial pneumonia of unknown etiology. Bull Chest Dis Res Inst Kyoto Univ 23(1–2):1–18
Kondoh Y et al (1993) Acute exacerbation in idiopathic pulmonary fibrosis. Analysis of clinical and pathologic findings in three cases. Chest 103(6):1808–1812
MacDonald SL et al (2001) Nonspecific interstitial pneumonia and usual interstitial pneumonia: comparative appearances at and diagnostic accuracy of thin-section CT. Radiology 221(3):600–605
Rice AJ et al (2003) Terminal diffuse alveolar damage in relation to interstitial pneumonias. An autopsy study. Am J Clin Pathol 119(5):709–714
Parambil JG, Myers JL, Ryu JH (2005) Histopathologic features and outcome of patients with acute exacerbation of idiopathic pulmonary fibrosis undergoing surgical lung biopsy. Chest 128(5):3310–3315
Furuya K et al (2017) Pirfenidone for acute exacerbation of idiopathic pulmonary fibrosis: a retrospective study. Respir Med 126:93–99
Kreuter M et al (2019) Differing severities of acute exacerbations of idiopathic pulmonary fibrosis (IPF): insights from the INPULSIS(R) trials. Respir Res 20(1):71
Vianello A et al (2019) Pirfenidone improves the survival of patients with idiopathic pulmonary fibrosis hospitalized for acute exacerbation. Curr Med Res Opin 35(7):1187–1190
Fujimoto K et al (2012) Acute exacerbation of idiopathic pulmonary fibrosis: high-resolution CT scores predict mortality. Eur Radiol 22(1):83–92
Sokai A et al (2017) Asymmetry in acute exacerbation of idiopathic pulmonary fibrosis. ERJ Open Res 3(2):00036–02016
Agarwal R, Jindal SK (2008) Acute exacerbation of idiopathic pulmonary fibrosis: a systematic review. Eur J Intern Med 19(4):227–235
Ambrosini V et al (2003) Acute exacerbation of idiopathic pulmonary fibrosis: report of a series. Eur Respir J 22(5):821–826
Inase N et al (2003) Cyclosporin A followed by the treatment of acute exacerbation of idiopathic pulmonary fibrosis with corticosteroid. Intern Med 42(7):565–570
Farrand E et al (2020) Corticosteroid use is not associated with improved outcomes in acute exacerbation of IPF. Respirology 25(6):629–635
Acknowledgements
No funding was required for this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
CJA, KC, JK and GG report no conflicts of interest. DR reports Salary Support from the Sandra Faire and Ivan Fecan Professorship in Rehabilitation Medicine. SS reports grants and personal fees from Boehringer-Ingelheim and Hoffman-La Roche Ltd. and personal fees from AstraZeneca, outside the submitted work. JHF reports grants from the Canadian Pulmonary Fibrosis Foundation and personal fees Boehringer-Ingelheim and AstraZeneca, outside the submitted work.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Adams, C.J., Chohan, K., Rozenberg, D. et al. Feasibility and Outcomes of a Standardized Management Protocol for Acute Exacerbation of Interstitial Lung Disease. Lung 199, 379–387 (2021). https://doi.org/10.1007/s00408-021-00463-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00408-021-00463-5