
Abstract
Silexan is a proprietary active substance produced from Lavandula angustifolia, with proven anxiolytic efficacy in subthreshold and generalized anxiety disorder as well as in mixed anxiety and depressive disorder with beneficial impact on anxiety-related sleep disturbances. The pharmacological profile and clinical observations suggest that Silexan may also have an antidepressant effect. To investigate the effect of Silexan on co-occurring depressive symptoms, we present a meta-analysis of the five placebo-controlled clinical trials hitherto performed with Silexan in subthreshold anxiety (n = 3) and anxiety disorders (n = 2). Patients of all trials received Silexan 1 × 80 mg/day or placebo for 10 weeks according to random assignment. Assessment of the antidepressant effect was based on item ‘depressed mood’ from the Hamilton Anxiety Rating Scale (HAMA) administered in all trials and on the total scores of the Montgomery Åsberg Depression Rating Scale (MADRS) or the Hamilton Depression Rating Scale (HAMD) used in three trials. After 10-week treatment, patients receiving Silexan showed significantly more pronounced score reduction for HAMA item ‘depressed mood’ than those in the placebo group (p = 0.01). Significant superiority of Silexan over placebo could also be shown for mean MADRS or HAMD total score reduction (three studies; p < 0.01). Silexan-treated patients with more severe depressive symptoms at baseline showed more pronounced improvements than those with milder symptoms. Our meta-analysis clearly shows that Silexan has a beneficial effect on co-occurring depressive symptoms in patients with subthreshold anxiety and anxiety disorders and may, hence, lead to important therapeutic implications for depressive disorders.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Anxiety disorders and major depression are the most prevalent mental ilnesses, accounting for more than half of the disease burden attributable to psychiatric diseases worldwide [1]. For anxiety and mood disorders, a meta-analysis based on 85 surveys covering more than 60 countries found lifetime prevalences of 12.9% and 9.6% as well as 12-month prevalences of 6.7% and 5.4%, respectively [2]. In Europe and the United States, these figures are even higher. In large epidemiological studies, 12-month prevalences were 14% and 18%, respectively, for anxiety disorders as well as 7.8% and 9.5%, respectively, for mood disorders [3,4,5].
Clinical experience as well as empirical data indicate that anxiety and depression are highly comorbid [6, 7]. Moreover, anxiety has been shown to predict later depression and vice versa, both on an individual symptom level and on the disorder level [8]. It has been estimated that up to 90% of patients with an anxiety disorder also exhibit symptoms of depression [9], and between 30 and 63% also meet the criteria for concurrent major depressive episode (MDE) [10]. Among the most central symptoms in both depression and anxiety are anhedonia, sad mood, and worry [11]. Due to symptom overlap, it is not surprising that the Hamilton Anxiety Rating Scale (HAMA) [12] includes items that assess depressed mood as well as symptoms overlapping with major depressive disorder (MDD, e.g., concentration), while the Hamilton Depression Rating Scale (HAMD) [13] includes items that assess anxiety.
Comorbid anxiety and depression are typically associated with a more severe clinical presentation than either condition alone [14], including greater severity and longer duration of illness, more severe functional impairment, and ultimately poorer clinical outcomes [15]. Patients with comorbid anxiety and depression were found to be more treatment resistant than those with either condition alone [7, 10, 16,17,18,19]. Moreover, it has been observed that co-morbidity of anxiety and depression increases the risk of exacerbation, e.g., patients suffering from subthreshold anxiety disorder with co-morbid depressive symptoms or with mixed anxiety and depressive disorder (MADD) may be at an increased risk of progressing to generalized anxiety disorder (GAD) or to MDD [9, 20]. The observation that subthreshold anxiety often constitutes a predictor of subsequent GAD or MDD is, therefore, of great value for prevention and may have important implications for treatment [21].
Nonclinical data indicate that there may be common neurobiological pathways to both anxiety and depression, most notably a dysregulation of the norepinephrine and serotonin (5-HT) neurotransmitter systems [22]. An increased neurotransmitter-release due to an enhanced Ca2+−influx mainly through N- and P/Q-type voltage dependent calcium channels (VDCCs) [23] and variations in serotonin-1A (5-HT1A) receptor binding [24, 25] may play a role in both types of disorder.
The interpretation is supported by the fact that substances with proven efficacy in the treatment of depression have been demonstrated to be efficacious in anxiety disorders as well. This is particularly true for selective serotonin reuptake inhibitors (SSRIs), whose efficacy in anxiety and depression has been linked to their agonistic action on the 5-HT1A receptor subtype [26, 27]. Consequently, agents such as SSRIs and selective norepinephrine reuptake inhibitors (SNRIs) that were originally developed as antidepressants are also recommended as first line treatment for anxiety disorders (e.g., [28]). There also appears to be a growing interest in the anxiolytic and antidepressant effects of preparations from lavender, with six reviews and meta-analyses published during 2019 and 2020 alone [29,30,31,32,33,34].
For Silexan,Footnote 1 an essential oil for oral administration manufactured from Lavandula angustifolia flowers, a potent inhibition of VDCCs in synaptosomes, primary hippocampal neurons and stably overexpressing cell lines [35], attenuating the overreaching, situationally inadequate stress response of the central nervous system associated with anxiety and mood disorders has been assumed (e.g., [36]). The active substance was shown to significantly increase the density of 5-HT1A receptors and to reduce the serotonin-1A receptor binding potential, leading to increases in extracellular serotonin, dopamine, and norepinephrine [37, 38]. A comprehensive characterization of the pharmacological profile of Silexan has been provided elsewhere [39, 40].
Silexan is the active substance of a medicinal product used for the treatment of anxiety. Treatment with Silexan was shown to be safe, without causing pharmacological interactions, sedation, or withdrawal symptoms at daily doses of 80 or 160 mg [39]. Randomized, double-blind, controlled clinical trials have demonstrated that Silexan has a significant anxiolytic effect in subthreshold anxiety disorder, MADD, and GAD [31, 41]. Results from these trials indicate that Silexan may also have an antidepressant effect [42] which could be explained by its impact on serotonergic mechanisms typically observed for serotonergic substances as SSRIs and SNRIs for instance [37, 38, 40, 43]. This might be of relevance especially in terms of its beneficial effects on sleep disturbances that rank among the most common and burdensome symptoms in both anxiety and depressive disorders [44]. In a retrospective case series on the use of Silexan in patients suffering from MDD and symptoms of psychomotor agitation, insomnia and anxiety, a reduction of anxiety-related symptoms and sleep disturbances, psychological anxiety and somatic anxiety was observed [45]. In addition, results from a recently published meta-analysis investigating all existing placebo-controlled clinical trials in anxiety patients treated with Silexan revealed statistically significant and clinically meaningful effects of Silexan over placebo in improving somatic symptoms as insomnia, fatigue and pain, which count to frequently occurring symptoms of both, anxiety and depressive disorders [46].
While compounds originally developed as antidepressants have been shown to be efficacious in the treatment of anxiety disorders as well, it might, therefore, be promising to assess the potential of Silexan, which was originally investigated as an anxiolytic agent, in the treatment of depression. Since the randomized, controlled trials performed with Silexan have consistently used the HAMA as a primary outcome measure and have thus assessed depressed mood as a co-morbidity symptom, we performed a meta-analysis of these trials with focus on the effect of Silexan on co-occurring depressive symptoms in patients suffering from subthreshold anxiety and anxiety disorders.
Methods
Included trials
Until the end of the year 2020, five 10-week, randomized, double-blind, placebo-controlled clinical trials investigating Silexan in subthreshold anxiety and in anxiety disorders were completed with sponsorship of the manufacturer [41, 47,48,49,50]. We performed free-text searches of all fields of PubMed as well as of the European Union (EU) Clinical Trials Register, the International Standard Randomized Controlled Trial Number (ISRCTN) Registry and of the ClinicalTrials.gov registry to identify any additional trials with Silexan in patients with anxiety disorders. Search terms were ‘anxiety’ in combination with either ‘Silexan’, ‘Lasea’, ‘WS1265’ or ‘WS 1265’ (‘WS 1265’ was the internal code used by the manufacturer for Silexan) and suppressing the automatic PubMed translation of ‘Silexan’ to ‘lavender oil’ when building the search query. The literature from the earliest record until 30 December 2020 was covered.
Interventions
Trials were eligible if participants received monotherapy with Silexan 1 × 80 mg/day as immediate-release soft gelatin capsules or a matching placebo for 10 weeks. Silexan is an essential oil manufactured from Lavandula angustifolia flowers by steam distillation that complies with the monograph Lavender oil of the European Pharmacopoeia and exceeds the quality requirements of the monograph. Batch to batch consistency is assured by a well-defined, standardized manufacturing process.
Analyses were performed on study participants who received either the recommended daily dose of the marketed product, i. e., 1 × 80 mg Silexan, or placebo. Results of treatment groups including active controls or Silexan administered at daily doses other than 80 mg/day were not considered in our meta-analysis.
Meta-analysis outcomes
The present meta-analysis was conducted according to a prospectively defined analysis plan. The mean change from baseline to the individual end of treatment in the HAMA item ‘depressed mood’ defined as ‘loss of interest, lack of pleasure in hobbies, depression, early waking, diurnal swing’ and assessed by means of a five-point verbal rating scale ranging from 0 (‘not present’) to 4 points (‘very severe’) was compared between the treatment groups.
Moreover, the effect of Silexan on co-morbid depression/depressive symptoms in subthreshold anxiety and anxiety disorders was assessed by comparing mean changes from baseline of the total score of the HAMD or of the Montgomery Åsberg Depression Rating Scale (MADRS), if available, with the HAMD being the first choice in cases, where both scales were used. Furthermore, the mean change in the self-rated Hospital Anxiety and Depression Scale (HADS) [51] and the brief, observer-rated Raskin Depression Rating Scale (RDRS) [52] served as additional outcomes for the assessment of depressive symptoms.
For those cases in which the protocols did not require patients to be suffering from co-occurring depressive symptoms, we also performed a subgroup analysis for HAMA item ‘depressed mood’ that included only patients who presented with a score of at least 2 points (‘moderate’) at baseline. This cutoff was chosen in accordance with Kasper et al. [50], who used the same minimum score as an inclusion criterion in their trial for assuring that patients were suffering from comorbid subthreshold depression. For the subgroup analysis on the depression rating scales, we used cutoff scores of ≥ 7 points for the MADRS and of ≥ 8 points for the HAMD total scores that have been found to be indicative of at least mild depression [53, 54].
Statistical methods
We performed a patient-level meta-analysis. The applicable analysis data set comprised the full analysis set (FAS) of the original protocols. For comparability with the published trial results, missing data were imputed by carrying forward the last valid observation.
To characterize the study populations, descriptive statistics were computed for age, sex, and premature withdrawal rate. The meta-analysis was based on a two-stage approach [55, 56]: within each trial, meta-analysis outcomes were analyzed using analysis of covariance (ANCOVA) with the difference between baseline and end of treatment for the outcome of interest as the dependent variable, treatment as a factor, and the baseline value of the analyzed outcome as a covariate. Marginal (adjusted) mean values and their standard deviations were then used as input for a random-effects meta-analysis on the treatment group mean value difference. Inverse variance weighting was used for combining the results of the single trials, and the DerSimonian–Laird method was applied for calculating the variance between the trials. As effect sizes, mean differences (MD) were calculated for the change of HAMA item ‘depressed mood’ and standardized mean differences (SMD) using Hedges’ g with bias correction for HAMD/MADRS total score changes. All p values are two-sided; values ≤ 0.05 were considered descriptively significant.
Heterogeneity between the trials was assessed using the I2 statistic in accordance with the criteria proposed by Deeks, et al. [57].
This meta-analysis was computed with R software (versions 3.1.2 and 3.6.0) using functions ‘metacont’ and ‘forest’ included in package meta (versions 4.3–2 and 4.13–0). All other analyses were performed in SAS statistical software version 9.4 for Windows.
Results
Characteristics of included trials
Searching PubMed resulted in 31 matches, none of which referred to a double-blind, randomized, placebo-controlled, therapeutic clinical trial in patients with subthreshold anxiety and anxiety disorders beyond those already mentioned. Searches in the indicated trial registers also did not add any clinical trials meeting these criteria.
The five trials included into our analysis were performed according to essentially similar protocols that differed mainly in the diagnosis for inclusion and in the derived inclusion and exclusion criteria as well as in some secondary outcome measures (Table 1). All trials have been approved by the appropriate ethics committee and have, therefore, been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. Trial A [48], trial B [47] and trial C [50] assessed patients with subthreshold anxiety, and trial D [41] as well as trial E [49] investigated patients suffering from GAD. In all trials, the participants were male or female outpatients between 18 and 65 years of age and treated by a psychiatrist or by a general practitioner. In addition to meeting the diagnostic criteria for the diagnoses for inclusion shown in Table 1, eligible participants had to have a baseline HAMA total score ≥ 18 points and had to meet other anxiety specific eligibility criteria as shown in Table 1. In trials D and E, the HAMD was administered mainly for excluding patients suffering from MDD as primary diagnosis. All participants of trial C had to be suffering from comorbid, subthreshold anxiety and depression in accordance with the diagnosis for inclusion.
The schedule of each trial started with a 3–7-day qualification phase after which eligible patients were randomized to receive Silexan or placebo for 10 weeks. Eligibility criteria had to be met both at the start (screening) and at the end (baseline) of the qualification phase. In trials A, B, D, and E, patients were not required to be suffering from co-occurring depressive symptoms. In trials A, B, D, and E, post-baseline outcome assessments were scheduled every 2 weeks, while the protocol of trial C included assessments at the end of weeks 1, 2, 4, 7, and 10.
Study participants received either Silexan 1 × 80 mg/day as immediate-release soft gelatin capsules or a matching placebo for 10 weeks. Trial D was a dose-finding trial that also included treatment arms with 10 and 40 mg/day Silexan. In trial E, paroxetine served as an active control, and another group received Silexan 160 mg/day.
For trials C, D, and E, the effect of Silexan on comorbid depression or on co-occurring depressive symptoms could be assessed based on the change of the total score of the HAMD (trials D and E) or the MADRS (trial C) between baseline and individual end of treatment. The total scores of the MADRS and the HAMD observer-rated depression scales served as the main instruments for assessing severity of depression according to the original protocols of trials C, D, and E. In trials D and E, HAMD assessments were obtained at baseline as well as at weeks 4 and 10 of randomized treatment. In trial C, the MADRS was administered at baseline and at all post-baseline visits. Moreover, the self-rated Hospital Anxiety and Depression Scale [HADS; 60] was used in trial C, and the brief, observer-rated Raskin Depression Rating Scale [RDRS; 44] was administered in trials D and E as additional secondary outcomes for the assessment of depression.
Characteristics of trial participants
In the pooled data set, a total of 1213 patients (Silexan N = 610; placebo N = 603) had been randomized and 1172 (Silexan N = 587; placebo N = 585) had been analyzed for efficacy in the FAS of the underlying five trials (Table 2). Since levels of depression tended to decrease during the randomized treatment period (see details below) and missing data (mainly resulting from premature withdrawal) were imputed by carrying the last observed value forward, premature withdrawal might have caused some bias of the depression scale results against Silexan.
The study participants’ age averaged around 46 years. More than 2/3 of the patients of all trials were female.
Within each trial, the baseline treatment group mean values for the HAMA item ‘depressed mood’ did not differ significantly (never exceeding 2.5 points). Baseline scores were highest in trial C performed in MADD, which was the only trial that included only patients with comorbid subthreshold depression at baseline, and lowest in the GAD trials D and E, both of which explicitly excluded patients with more severe depression. In trials C through E, the baseline total scores of the MADRS and the HAMD also support the baseline comparability of the treatment groups regarding their average severity of depressive symptoms (Table 3). Moreover, the baseline treatment group mean values for the MADRS (trial C) and for the HAMD total score (trials D and E) were in a range typically found in patients with mild to moderate intensity of depression [53, 54].
HAMA item ‘depressed mood’
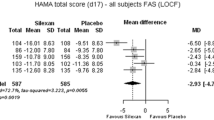
With respect to the pooled mean reduction in the outcome HAMA item ‘depressed mood’ between baseline and treatment end, we found a significant superiority of Silexan over placebo (MD = − 0.21, 95% confidence interval; CI − 0.38 to − 0.04; p = 0.01) (Fig. 1 Panel A). In the subset of patients with a baseline score ≥ 2 points (i. e., those who had at least moderate depressive symptoms at baseline, including all patients from trial C, where this was an inclusion criterion), the overall meta-analysis effect of Silexan was even more pronounced than in the complete FAS (MD = − 0.27, 95% CI − 0.47 to − 0.07; p < 0.01) (Fig. 1 Panel B).

Meta-analysis of Hamilton Anxiety Rating Scale item ‘depressed mood’, intraindividual change between baseline and end of treatment (last observation carried forward). Panel A: all patients in the full analysis set; Panel B: patients with a baseline score ≥ 2 points
With I2 = 67% for the FAS and I2 = 44% for the subset with at least moderate depressive symptoms at baseline, Fig. 1 also indicates substantial heterogeneity between the trials. This was mainly attributable to the fact that the participants of trials D and E, who had substantially lower depression scores at baseline, due to the exclusion criteria in these trials (Tables 1, 2), showed lower absolute score reductions during randomized treatment, and thus also smaller absolute treatment group differences.
For the trials performed in patients with subthreshold anxiety, Fig. 2 shows the mean value differences between Silexan and placebo (including the associated 95% Cis) for HAMA item ‘depressed mood’. Descriptively significant advantages for Silexan were observed from day 42 of randomized treatment in trial A, between day 14 (patients with a baseline score ≥ 2 points) or day 28 (FAS) and day 56 in trial B, and from day 14 in trial C (p ≤ 0.05). In trials B and C, the stabilization or decrease of the difference between Silexan and placebo after day 28 was attributable to an increasingly large placebo effect, while the scores in the Silexan group stabilized (trial B) or decreased at a slower rate than during the initial weeks of randomized treatment (trial C).

Hamilton Anxiety Rating Scale item ‘depressed Mood’ change from baseline—mean value differences between Silexan and placebo for all patients in the full analysis set (Panel A) and for patients with a baseline score ≥ 2 points (Panel B; negative values favor Silexan)
MADRS and HAMD
The mean total score reduction in MADRS/HAMD was significantly higher in the pooled Silexan group compared with the placebo group (SMD = − 0.3, 95% CI − 0.44 to − 0.16; p < 0.01) (Table 3), with minimal heterogeneity between the trials (I2 = 0%; Fig. 3).

Meta-analysis of depression rating scales total score, intraindividual change between baseline and end of treatment (trial C: Montgomery Åsberg Depression Rating Scale; trials D, E: Hamilton Anxiety Rating Scale; SMD: standardized mean value difference; last observation carried forward). Panel A: all patients in the full analysis set; Panel B: patients with at least mild depression at baseline
As all patients in trial C and the majority of participants of trials D and E had at least mild symptoms of depression (i. e., a MADRS total score ≥ 7 or a HAMD total score ≥ 8) at baseline, the results in the FAS and in the ‘Depression’ subset were similar, with slightly larger effect sizes favoring Silexan in trials D and E as well as overall in the ‘Depression’ subset.
Other depression scales (full analysis set)
In trial C, average intraindividual decreases by 2.2 ± 5.0 (mean ± SD) and by 1.8 ± 4.1 points were observed in the self-rated HADS between baseline and end of treatment (p = 0.52) for Silexan and placebo, respectively, for the depression sub-score, following baseline values of 10.7 ± 4.7 and of 10.5 ± 4.2 points.
In trials D and E, the RDRS was mainly used as an additional secondary outcome for the assessment of depression to assure the exclusion of patients suffering from a MDE as primary diagnosis. In trial D, the RDRS total score in the Silexan group decreased by 0.8 ± 1.5 points from a baseline average of 5.2 ± 1.1 points, compared to a baseline mean value of 5.1 ± 1.1 points and a decrease by 0.5 ± 1.4 points in the placebo group (p = 0.14). In trial E, the patients in the Silexan 80 mg/day group showed a RDRS baseline mean value of 5.1 ± 1.1 points and a decrease between baseline and end of treatment by 0.7 ± 1.6 points, compared to a baseline value of 5.2 ± 1.1 points and a decrease by 0.4 ± 1.6 points for placebo (p = 0.17).
Discussion
This meta-analysis of five double-blind, randomized, placebo-controlled trials in subthreshold anxiety and anxiety disorders found that Silexan, which has already been demonstrated to be an efficacious anxiolytic compound [31, 39], is also effective in reducing co-occurring depressive symptoms.
In the trials in subthreshold anxiety disorder in which no specific depression scale was administered, Silexan was associated with a reduction of the treatment group mean value for depressed mood at or above 50% of the baseline value, notably in patients with at least moderate symptoms of depression at baseline, with significant superiority over placebo in two trials and a borderline significant result in the third, based on HAMA item ‘depressed mood’.
In the only trial investigating patients with MADD, where comorbid subthreshold depression at baseline was required as a part of the clinical diagnosis for inclusion, a significant antidepressant effect of Silexan over placebo was observed for the MADRS total score already after 4-week randomized treatment, and the treatment group difference remained significant until the end of the trial after 10 weeks.
For the two trials in GAD, which explicitly excluded patients with more severe depression, one needs to consider that patients were only eligible for inclusion if they presented with a HAMD total score ≤ 17 points and with a score < 2 points for HAMA item ‘depressed mood’ at both screening and baseline, which resulted in study populations with comparatively low rates for comorbid depressive symptoms. It is, therefore, not surprising that a single-item measure such as HAMA item ‘depressed mood’, with its limited sensitivity for change over time, did not capture a meaningful antidepressant effect in this specific patient population. By contrast, a clear antidepressant effect of Silexan over placebo was observed for HAMD total score change, with significant superiority in one of the two GAD trials even though only patients with predominantly mild depressive symptoms were included.
In summary, our meta-analysis indicates that co-occurring depressive symptoms improved significantly during treatment with Silexan. This observation is consistent with the existing psychopharmacotherapeutic evidence supporting a possible direct antidepressant effect of the herbal medicinal product [35, 37]. In vitro, Silexan was shown to improve synaptic neuroplasticity, which is discussed as a common pathway for the mechanisms of action of most antidepressants [58, 59]. Similarly to previous observations in antidepressants, a significant effect on neurite outgrowth in PC12 cells and on synapse density in primary hippocampal neurons has been assumed for Silexan [43]. In vivo, Friedland, et al. [43] performed a forced swimming test in rats, a behavioral model commonly used to assess activity of antidepressant therapies and found that the effects of Silexan were comparable to those of imipramine that served as an active control. Moreover, linalool, one of the major constituents of Silexan, was found to show antidepressant-like properties in an immobilization test performed in mice [60]. Whether the alleviation of depressive symptoms could be mediated by the anxiolytic effect of Silexan, might be subject to further investigation.
The abovementioned results and consequent assumptions on beneficial and clinically meaningful effects of Silexan on both, anxious and depressive symptoms, might be further underlined by findings derived from clinical trials reporting superior effects of Silexan on sleep disturbances, psychomotor agitation and somatic symptoms including fatigue and pain for instance, which represent frequent and burdensome manifestations occurring in the course of both clinical phenotypes [44,45,46]. It might be noteworthy in this regard that the recently published meta-analysis focusing on Silexan effects on somatic symptoms and physical health in general was conducted in a patient population that is identical with that investigated in the present meta-analysis, whereby a similar approach using HAMA items to evaluate the respective target-symptoms was employed [46].
As was already shown previously, Silexan is well tolerated and does not cause pharmacological interactions or withdrawal symptoms at daily doses of 80 or 160 mg [39]. A good tolerability of psychopharmacotherapy with Silexan can also be assumed as a result of our findings, which show a pooled drop-out rate of 12.0% detected for Silexan compared to 10.6% for placebo (Table 2).
While no clinical trials with Silexan in patients with primary MDD have been completed yet, it is a strength of this investigation that our analyses cover all randomized, placebo-controlled trials performed with the herbal product in subthreshold anxiety and anxiety disorders, representing the complete existing body of evidence for the effect of Silexan on co-occurring depressive symptoms. A limitation of our analyses could be the fact that the assessment of the antidepressant effect in two of the five trials (A and B) had to rely solely on a single item from the HAMA questionnaire. In trial C performed in MADD, the results obtained for this item were consistent with those for the MADRS. However, in contrast to the results obtained for the HAMD, the single-item measure apparently lacked the sensitivity for monitoring intraindividual change of depressive symptom intensity in the at most mildly depressed patients of trials D and E performed in GAD. In summary, the resultant heterogeneous clinical manifestations of comorbid depressive symptoms in patients with primary (subthreshold) anxiety disorders might explain the subtle differences in the observed antidepressant effects and should be considered while interpreting the present results.
Our analyses also reveal that patients with more severe depressive symptoms at baseline tended to show more pronounced symptom alleviation during treatment with Silexan. Since not all trial participants showed substantial symptoms of depression, the analyses based on the FAS of the studies may have underestimated the true antidepressant effect of Silexan.
Finally, it should be considered that the present work is based on data which were gathered and published by authors of the same research group who are largely represented in this and a further recently published meta-analysis [46]. The detected effect sizes might, hence, exhibit potentially higher similarities than it would be the case, when studies of different research groups would be involved, which may result from the way how the distinct parameters were analyzed, how the patients were recruited and sampled, and how the data were assessed by the study interviewers [61, 62]. A specific example of the latter phenomenon represented by a similar network meta-analysis including 4 papers published by Kasper et al. [63] has already been discussed in the aforementioned meta-analysis, highlighting that all included studies were performed in accordance with Good Clinical and Scientific Practice [46]. Hence, the data and the reported results should be considered robust and scientifically sound.
In conclusion, the results of our meta-analysis underline that Silexan, at the marketed dosage of 1 × 80 mg/day, has a significant alleviating effect on co-occurring depressive symptoms in patients suffering from subthreshold anxiety and an anxiety disorder. While our analysis does not provide conclusive evidence as to whether this is a direct antidepressant effect or an effect mediated by the anxiolytic activity of the compound, evidence from in-vitro and in-vivo pharmacological experiments as well as information about Silexan’s mechanism of action could explain a direct antidepressant effect that may result from an improvement of neuroplasticity and its effects on monoaminergic neurotransmission [37, 38, 40, 43, 64]. Taken together, the results thus indicate that Silexan reduces depressive symptoms in anxiety patients and, in addition, might have a beneficial effect in patients with depressive disorders. This should be confirmed in future trials.
Data availability
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Code availability
Not applicable.
Notes
Silexan® is the active substance of Lasea® (Dr. Willmar Schwabe GmbH & Co. KG, Karlsruhe, Germany).
References
Whiteford HA, Degenhardt L, Rehm J, Baxter AJ, Ferrari AJ, Erskine HE, Charlson FJ, Norman RE, Flaxman AD, Johns N, Burstein R, Murray CJL, Vos T (2013) Global burden of disease attributable to mental and substance use disorders: findings from the global burden of disease study 2010. Lancet 382:1575–1586
Steel Z, Marnane C, Iranpour C, Chey T, Jackson JW, Patel V, Silove D (2014) The global prevalence of common mental disorders: a systematic review and meta-analysis 1980–2013. Int J Epidemiol 43:476–493
Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE (2005) Lifetime prevalence and age-of-onset distributions of dsm-iv disorders in the national comorbidity survey replication. Arch Gen Psychiatry 62:593–602
Kessler RC, Chiu WT, Demler O, Merikangas KR, Walters EE (2005) Prevalence, severity, and comorbidity of 12-month dsm-iv disorders in the national comorbidity survey replication. Arch Gen Psychiatry 62:617–627
Wittchen HU, Jacobi F, Rehm J, Gustavsson A, Svensson M, Jönsson B, Olesen J, Allgulander C, Alonso J, Faravelli C, Fratiglioni L, Jennum P, Lieb R, Maercker A, van Os J, Preisig M, Salvador-Carulla L, Simon R, Steinhausen H-C (2011) The size and burden of mental disorders and other disorders of the brain in Europe 2010. Eur Neuropsychopharmacol 21:655–679
Bui E, Fava M (2017) From depression to anxiety, and back. Acta Psychiatr Scand 136:341–342
Saha S, Lim CCW, Cannon DL, Burton L, Bremner M, Cosgrove P, Huo YJ, McGrath J (2021) Co-morbidity between mood and anxiety disorders: a systematic review and meta-analysis. Depress Anxiety 38:286–306
Jacobson NC, Newman MG (2017) Anxiety and depression as bidirectional risk factors for one another: a meta-analysis of longitudinal studies. Psychol Bull 143:1155–1200
Möller H-J, Bandelow B, Volz H-P, Barnikol UB, Seifritz E, Kasper S (2016) The relevance of “mixed anxiety and depression” as a diagnostic category in clinical practice. Eur Arch Psychiatry Clin Neurosci 266:725–736
Kircanski K, LeMoult J, Ordaz S, Gotlib IH (2017) Investigating the nature of co-occurring depression and anxiety: comparing diagnostic and dimensional research approaches. J Affect Disord 216:123–135
Beard C, Millner AJ, Forgeard MJ, Fried EI, Hsu KJ, Treadway MT, Leonard CV, Kertz SJ, Björgvinsson T (2016) Network analysis of depression and anxiety symptom relationships in a psychiatric sample. Psychol Med 46:3359–3369
Hamilton M (1959) The assessment of anxiety states by rating. Br J Med Psychol 32:50–55
Hamilton M (1967) Development of a rating scale for primary depressive illness. Br J Soc Clin Psychol 6:278–296
Talkovsky AM, Green KL, Osegueda A, Norton PJ (2017) Secondary depression in transdiagnostic group cognitive behavioral therapy among individuals diagnosed with anxiety disorders. J Anxiety Disord 46:56–64
Lyndon GJ, Prieto R, Wajsbrot DB, Allgulander C, Bandelow B (2019) Efficacy of venlafaxine extended release in major depressive disorder patients: effect of baseline anxiety symptom severity. Int Clin Psychopharmacol 34:110–118
Bartova L, Dold M, Kautzky A, Fabbri C, Spies M, Serretti A, Souery D, Mendlewicz J, Zohar J, Montgomery S, Schosser A, Kasper S (2019) Results of the European Group for the Study of Resistant Depression (GSRD)—basis for further research and clinical practice. World J Biol Psychiatry 20:427–448
Dold M, Bartova L, Souery D, Mendlewicz J, Serretti A, Porcelli S, Zohar J, Montgomery S, Kasper S (2017) Clinical characteristics and treatment outcomes of patients with major depressive disorder and comorbid anxiety disorders—results from a european multicenter study. J Psychiatr Res 91:1–13
Kautzky A, Dold M, Bartova L, Spies M, Kranz GS, Souery D, Montgomery S, Mendlewicz J, Zohar J, Fabbri C, Serretti A, Lanzenberger R, Dikeos D, Rujescu D, Kasper S (2019) Clinical factors predicting treatment resistant depression: affirmative results from the European multicenter study. Acta Psychiatr Scand 139:78–88
Kautzky A, Möller H-J, Dold M, Bartova L, Seemüller F, Laux G, Riedel M, Gaebel W, Kasper S (2021) Combining machine learning algorithms for prediction of antidepressant treatment response. Acta Psychiatr Scand 143:36–49
Haller H, Cramer H, Lauche R, Gass F, Dobos GJ (2014) The prevalence and burden of subthreshold generalized anxiety disorder: a systematic review. BMC Psychiatry 14:128
Meier SM, Petersen L, Mattheisen M, Mors O, Mortensen PB, Laursen TM (2015) Secondary depression in severe anxiety disorders: a population-based cohort study in Denmark. Lancet Psychiatry 2:515–523
Ressler KJ, Nemeroff CB (2000) Role of serotonergic and noradrenergic systems in the pathophysiology of depression and anxiety disorders. Depress Anxiety 12(Suppl 1):2–19
Musazzi L, Racagni G, Popoli M (2011) Stress, glucocorticoids and glutamate release: effects of antidepressant drugs. Neurochem Int 59:138–149
Akimova E, Lanzenberger R, Kasper S (2009) The serotonin-1a receptor in anxiety disorders. Biol Psychiatry 66:627–635
Savitz J, Lucki I, Drevets WC (2009) 5-ht(1a) receptor function in major depressive disorder. Prog Neurobiol 88:17–31
Berk M (2000) Selective serotonin reuptake inhibitors in mixed anxiety-depression. Int Clin Psychopharmacol 15(Suppl 2):S41-45
Stahl SM (1997) Mixed depression and anxiety: Serotonin1a receptors as a common pharmacologic link. J Clin Psychiatry 58(Suppl 8):20–26
Bandelow B, Sher L, Bunevicius R, Hollander E, Kasper S, Zohar J, Möller HJ, WFSBP Task Force on Mental Disorders in Primary Care, WFSBP Task Force on Anxiety Disorders, OCD and PTSD (2012) Guidelines for the pharmacological treatment of anxiety disorders, obsessive-compulsive disorder and posttraumatic stress disorder in primary care. Int J Psychiatry Clin Pract 16:77–84
Donelli D, Antonelli M, Bellinazzi C, Gensini GF, Firenzuoli F (2019) Effects of lavender on anxiety: a systematic review and meta-analysis. Phytomedicine 65:153099
Kang H-J, Nam ES, Lee Y, Kim M (2019) How strong is the evidence for the anxiolytic efficacy of lavender?: Systematic review and meta-analysis of randomized controlled trials. Asian Nurs Res (Korean Soc Nurs Sci) 13:295–305
Möller H-J, Volz H-P, Dienel A, Schläfke S, Kasper S (2019) Efficacy of silexan in subthreshold anxiety: meta-analysis of randomised, placebo-controlled trials. Eur Arch Psychiatry Clin Neurosci 269:183–193
Ogata K, Ataka K, Suzuki H, Yagi T, Okawa A, Fukumoto T, Zhang B, Nakata M, Yada T, Asakawa A (2020) Lavender oil reduces depressive mood in healthy individuals and enhances the activity of single oxytocin neurons of the hypothalamus isolated from mice: a preliminary study. Evid Based Complement Altern Med 2020:5418586
Sayed AM, Morsy S, Tawfik GM, Naveed S, Minh-Duc NT, Hieu TH, Ali ZA, Shinkar A, Doheim MF, Hashan MR, Huy NT (2020) The best route of administration of lavender for anxiety: a systematic review and network meta-analysis. Gen Hosp Psychiatry 64:33–40
Yap WS, Dolzhenko AV, Jalal Z, Hadi MA, Khan TM (2019) Efficacy and safety of lavender essential oil (silexan) capsules among patients suffering from anxiety disorders: a network meta-analysis. Sci Rep 9:18042
Schuwald AM, Nöldner M, Wilmes T, Klugbauer N, Leuner K, Müller WE (2013) Lavender oil-potent anxiolytic properties via modulating voltage dependent calcium channels. PLoS ONE 8:e59998
Satpute AB, Mumford JA, Naliboff BD, Poldrack RA (2012) Human anterior and posterior hippocampus respond distinctly to state and trait anxiety. Emotion 12:58–68
Baldinger P, Höflich AS, Mitterhauser M, Hahn A, Rami-Mark C, Spies M, Wadsak W, Lanzenberger R, Kasper S (2015) Effects of silexan on the serotonin-1a receptor and microstructure of the human brain: a randomized, placebo-controlled, double-blind, cross-over study with molecular and structural neuroimaging. Int J Neuropsychopharmacol 18:1–9
Kehr J, Yoshitake T, Koch E, Noeldner M (2010) Effects of intraperitoneal administration of silexan, an essential oil from flowers of lavandula angustifolia on extracellular levels of noradrenaline, dopamine and serotonin in the prefrontal cortex of freely moving rats. Planta Med 76:1316–1316
Kasper S, Müller WE, Volz H-P, Möller H-J, Koch E, Dienel A (2018) Silexan in anxiety disorders: clinical data and pharmacological background. World J Biol Psychiatry 19:412–420
Müller WE, Sillani G, Schuwald A, Friedland K (2021) Pharmacological basis of the anxiolytic and antidepressant properties of silexan®, an essential oil from the flowers of lavender. Neurochem Int 143:104899
Kasper S, Möller H-J, Volz H-P, Schläfke S, Dienel A (2017) Silexan in generalized anxiety disorder: investigation of the therapeutic dosage range in a pooled data set. Int Clin Psychopharmacol 32:195–204
Kasper S, Dienel A (2013) Silexan (ws® 1265) vermindert begleitende depressive symptome bei patienten mit angsterkrankungen. Z Phytother 34:V01
Friedland K, Silani G, Schuwald A, Stockburger C, Koch E, Nöldner M, Müller WE (2021) Neurotrophic properties of silexan, an essential oil from the flowers of lavender-preclinical evidence for antidepressant-like properties. Pharmacopsychiatry 54:37–46
Seifritz E, Schläfke S, Holsboer-Trachsler E (2019) Beneficial effects of silexan on sleep are mediated by its anxiolytic effect. J Psychiatr Res 115:69–74
Fißler M, Quante A (2014) A case series on the use of lavendula oil capsules in patients suffering from major depressive disorder and symptoms of psychomotor agitation, insomnia and anxiety. Complement Ther Med 22:63–69
von Känel R, Kasper S, Bondolfi G, Holsboer-Trachsler E, Hättenschwiler J, Hatzinger M, Imboden C, Heitlinger E, Seifritz E (2021) Therapeutic effects of Silexan on somatic symptoms and physical health in patients with anxiety disorders: a meta-analysis. Brain Behav 11(4):e01997. https://doi.org/10.1002/brb3.1997
Kasper S, Anghelescu I, Dienel A (2015) Efficacy of orally administered silexan in patients with anxiety-related restlessness and disturbed sleep—a randomized, placebo-controlled trial. Eur Neuropsychopharmacol 25:1960–1967
Kasper S, Gastpar M, Müller WE, Volz H-P, Möller H-J, Dienel A, Schläfke S (2010) Silexan, an orally administered lavandula oil preparation, is effective in the treatment of ‘subsyndromal’ anxiety disorder: a randomized, double-blind, placebo controlled trial. Int Clin Psychopharmacol 25:277–287
Kasper S, Gastpar M, Müller WE, Volz H-P, Möller H-J, Schläfke S, Dienel A (2014) Lavender oil preparation silexan is effective in generalized anxiety disorder—a randomized, double-blind comparison to placebo and paroxetine. Int J Neuropsychopharmacol 17:859–869
Kasper S, Volz H-P, Dienel A, Schläfke S (2016) Efficacy of silexan in mixed anxiety-depression—a randomized, placebo-controlled trial. Eur Neuropsychopharmacol 26:331–340
Zigmond AS, Snaith RP (1983) The hospital anxiety and depression scale. Acta Psychiatr Scand 67:361–370
Raskin A, Schulterbrandt J, Reatig N, McKeon JJ (1969) Replication of factors of psychopathology in interview, ward behavior and self-report ratings of hospitalized depressives. J Nerv Ment Dis 148:87–98
Snaith RP, Harrop FM, Newby DA, Teale C (1986) Grade scores of the montgomery-asberg depression and the clinical anxiety scales. Br J Psychiatry 148:599–601
Zimmerman M, Martinez JH, Young D, Chelminski I, Dalrymple K (2013) Severity classification on the hamilton depression rating scale. J Affect Disord 150:384–388
Burke DL, Ensor J, Riley RD (2017) Meta-analysis using individual participant data: one-stage and two-stage approaches, and why they may differ. Stat Med 36:855–875
Riley RD, Lambert PC, Abo-Zaid G (2010) Meta-analysis of individual participant data: rationale, conduct, and reporting. BMJ 340:c221
Deeks JJ, Higgins JPT, Altman DG (2020) Analysing data and undertaking meta-analyses. In: Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (Eds.). Cochrane handbook for systematic reviews of interventions version 61 (updated September 2020). The cochrane collaboration, Available from www.training.cochrane.org/handbook
Duman RS, Aghajanian GK, Sanacora G, Krystal JH (2016) Synaptic plasticity and depression: new insights from stress and rapid-acting antidepressants. Nat Med 22:238–249
Harmer CJ, Duman RS, Cowen PJ (2017) How do antidepressants work? New perspectives for refining future treatment approaches. Lancet Psychiatry 4:409–418
Guzmán-Gutiérrez SL, Gómez-Cansino R, García-Zebadúa JC, Jiménez-Pérez NC, Reyes-Chilpa R (2012) Antidepressant activity of litsea glaucescens essential oil: Identification of β-pinene and linalool as active principles. J Ethnopharmacol 143:673–679
Cooper HM (2009) Research synthesis and meta-analysis: a step-by-step approach. Applied social research methods series, 4th edn. Sage, Thousand Oaks
Van den Noortgate W, López-López JA, Marín-Martínez F, Sánchez-Meca J (2013) Three-level meta-analysis of dependent effect sizes. Behav Res Methods 45(2):576–594
Yap WS, Dolzhenko AV, Jalal Z, Hadi MA, Khan TM (2019) Efficacy and safety of lavender essential oil (Silexan) capsules among patients suffering from anxiety disorders: a network meta-analysis. Sci Rep 9(1):18042
Hashimoto K (2019) Impact of FAAH gene, hyperactivation in emotion processing brain regions and Lavender oil preparation Silexan in anxiety. Eur Arch Psychiatry Clin Neurosci 269(2):145–146
Covi L, Rickels K, Lipman RS, McNair DM, Smith VK, Downing R, Kahn R, Fisher S (1981) Effects of psychotropic agents on primary depression. Psychopharmacol Bull 17:100–103
Montgomery SA, Åsberg M (1979) A new depression scale designed to be sensitive to change. Br J Psychiatry 134:382–389
Acknowledgements
Medical Writing for the first manuscript draft was provided by Dr. Andreas Völp, Psy Consult Scientific Services, Hamburg, Germany. The authors thank Sandra Schläfke of the sponsor’s biometric unit for data analysis and statistical support.
Funding
Open access funding provided by Medical University of Vienna. This research and its publication were financially supported by Dr. Willmar Schwabe GmbH & Co. KG, Karlsruhe, Germany, manufacturer of Silexan. The sponsor provided conceptualization of the study design, analysis of data, and medical writing and gave editorial support. The final decision on content was retained by the authors.
Author information
Authors and Affiliations
Contributions
H-PV, H-JM, and SK contributed to the conception and design of the study. LB, MD, H-PV, ES, H-JM, and SK contributed to the interpretation of data and drafting of the manuscript. All authors critically revised the manuscript and gave their final approval for submission.
Corresponding author
Ethics declarations
Conflict of interest
LB has received travel grants and consultant/speaker honoraria from AOP Orphan, Medizin Medien Austria, Vertretungsnetz, Schwabe Austria, Janssen and Angelini. MD has received travel grants and consultant/speaker honoraria from Janssen-Cilag. Within the last 3 years, H-PV has served as a consultant or on advisory boards for Astra/Zeneca, Eli Lilly, Lundbeck, Pfizer, Schwabe, Janssen, Otsuka, Angelini, and Sage and has served on speakers’ bureaus for Astra/Zeneca, Eli Lilly, Lundbeck, Schwabe, Janssen, Bayer, Recordati and neuraxpharm. ES received in the last 3 years honoraria and grants for advice and educational lectures from Lundbeck Switzerland, Schwabe Switzerland and Germany, Janssen Switzerland, Otsuka Switzerland, Mepha Pharma Switzerland, Otsuka Pharma Switzerland, Ricordati Switzerland and Sunovion Pharma UK and Angelini. H-JM has received grant/research support, consulting fees and honoraria within the last years from AstraZeneca, Lundbeck, Otsuka, and Schwabe. SK has received grant/research support from Lundbeck; he has served as a consultant or on advisory boards for Angelini, Biogen, Esai, Janssen, IQVIA, Lundbeck, Mylan, Recordati, Sage and Schwabe; and he has served on speakers bureaus for Aspen Farmaceutica S.A., Angelini, Biogen, Janssen, Lundbeck, Neuraxpharma, Recordati, Sage, Sanofi, Schwabe, Servier and Sun Pharma.
Ethical approval
Our research complies with internationally accepted standards for research practice and reporting. The present investigation was carried out in accordance with the latest version of the Declaration of Helsinki.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bartova, L., Dold, M., Volz, HP. et al. Beneficial effects of Silexan on co-occurring depressive symptoms in patients with subthreshold anxiety and anxiety disorders: randomized, placebo-controlled trials revisited. Eur Arch Psychiatry Clin Neurosci 273, 51–63 (2023). https://doi.org/10.1007/s00406-022-01390-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00406-022-01390-z