
Abstract
Purpose
Parturients with a history of a cesarean delivery (CD) in the first delivery (P1), undergoing induction of labor (IOL) in the subsequent delivery (P2) are at increased risk for obstetric complications. The primary aim was to study if “the stage of labor” at previous cesarean (elective/latent/first/second) is associated with a successful IOL. The secondary aim was to search for other obstetric characteristics associated with a successful IOL.
Methods
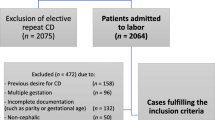
A retrospective longitudinal follow-up study in a large tertiary medical center. All parturients at term who underwent IOL at P2 with a singleton fetus in cephalic presentation, with a prior CD, between the years 2006 and 2014 were included. A univariate analysis was performed including the stage of labor at previous cesarean, birth weight of newborn at P1 and P2, gestational week of delivery at P2, time of interpregnancy interval, indication and mode of IOL, epidural analgesia and augmentation of labor at P2. Significant factors were incorporated in a multivariate logistic regression model.
Results
During the study period, 150 parturients underwent IOL (P2) subsequent to a previous CD (P1). VBAC was achieved in 78 (52%). We found no association between the stages of labor in which the previous CD was performed to a successful IOL. Applying the multivariate logistic regression revealed that augmentation of labor with oxytocin, OR 4.17, [1.73–10.05], epidural analgesia OR 3.30 [1.12–9.73] and birth weight (P2) < 4000 g, OR 5.88, [1.11–33.33] were associated with a successful IOL.
Conclusion
The stage of labor at previous CD should not be incorporated among the variables found to be associated with a successful IOL. As a result of our findings, clinician's will be able to adjust a personalized consult prior to initiating IOL.
Similar content being viewed by others


References
Boerma T, Ronsmans C, Melesse DY, Barros AJD, Barros FC, Juan L, Moller AB, Say L, Hosseinpoor AR, Yi M, de Lyra Rabello Neto D, Temmerman M (2018) Global epidemiology of use of and disparities in caesarean sections. Lancet 392(10155):1341–1348
Betran AP, Torloni MR, Zhang J et al (2015) What is the optimal rate of caesarean section at population level? A systematic review of ecologic studies. Reprod Health 12:57
Visser GHA, Ayres-de-Campos D, Barnea ER, de Bernis L, Di Renzo GC, Vidarte MFE, Lloyd I, Nassar AH, Nicholson W, Shah PK, Stones W, Sun L, Theron GB, Walani S (2018) FIGO position paper: how to stop the caesarean section epidemic. Lancet 392(10155):1286–1287
Lydon-Rochelle M, Holt VL, Easterling TR, Martin DP (2001) Risk of uterine rupture during labor among women with a prior cesarean delivery. N Engl J Med 345:3–8
Rageth JC, Juzi C, Grossenbacher H (1999) Delivery after previous cesarean: a risk evaluation. Swiss working group of obstetric and gynecologic institutions. Obstet Gynecol 93:332–337
Landon MB, Hauth JC, Leveno KJ, Spong CY, Leindecker S, Varner MW et al (2004) Maternal and perinatal outcomes associated with a trial of labor after prior cesarean delivery. N Engl J Med 351:2581–2589
Kwee A, Bots ML, Visser GHA, Bruinse HW (2006) Obstetric management and outcome of pregnancy in women with a history of caesarean section in the Netherlands. Eur J Obstet Gynecol Reprod Biol 132:171–176
Agnew G, Turner MJ (2009) Vaginal prostaglandin gel to induce labour in women with one previous caesarean section. J Obstet Gynaecol (Lahore) 29:209–211
Ye J, Betran AP, Guerrero Vela M, Souza JP, Zhang J (2014) Searching for the optimal rate of medically necessary cesarean delivery. Birth 41:237–244
WHO recommendations: non-clinical interventions to reduce unnecessary caesarean sections https://apps.who.int/iris/bitstream/handle/10665/275377/9789241550338-eng.pdf?ua=1. Accessed 29 Feb 2020
Kugelman N, Sagi-Dain L, Kleifeld S, Kedar R, Bardicef M, Toledano-Hacohen M, Damti A (2020) Can recurrent cesarean section due to arrest of descent be predicted by newborn weight difference? Eur J Obstet Gynecol Reprod Biol. 245:73–76. https://doi.org/10.1016/j.ejogrb.2019.12.008(Epub 2019 Dec 23)
Funding
This study was not funded by any organization.
Author information
Authors and Affiliations
Contributions
DA: protocol development, data collection and management, data analysis, and manuscript writing/editing. RR: protocol development, data collection and management, data analysis, and manuscript writing/editing. MR: protocol development and manuscript writing/editing. MB-L: data collection and management, manuscript. AS: data collection and management, data analysis SG-G: data collection and management, data analysis OR: protocol development, data collection and management, data analysis, and manuscript writing/editing.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have nothing to disclose and that they have no financial or non-financial conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. For this type of study, formal consent is not required. This article does not contain any studies with animals performed by any of the authors. The Shaare Zedek Medical Center institutional review board approved the study (0038-16), with waiver of informed consent due to the retrospective, observational design of the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Amitai, D., Rotem, R., Rottenstreich, M. et al. Induction of labor at second delivery subsequent to a primary cesarean: is stage of labor at previous cesarean a factor?. Arch Gynecol Obstet 303, 659–663 (2021). https://doi.org/10.1007/s00404-020-05776-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00404-020-05776-z