
Abstract
Introduction
Complex ankle fractures frequently involve the posterior malleolus. Many classifications describing posterior malleolar fractures (PMF) exist. The aim of this study was to provide a systematic literature review to outline existing PMF classifications and estimate their accuracy.
Methods
The databases PubMed and Scopus were searched without time limits. Only specific PMF classifications were included; general ankle and/or pilon fracture classifications were excluded. Selection and data extraction was performed by three independent observers. The systematic literature search was performed according to the current criteria of Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA). The methodological quality of the included studies was quantified using the modified Coleman score.
Results
A total of 110 studies with a total of 12.614 patients were included. Four main classifications were identified: Those describing the size of the posterior malleolar fracture (n = 66), Haraguchi (n = 44), Bartoníček/Rammelt (n = 21) and Mason (n = 12). The quality of the studies was moderate to good with a median Coleman-score of 43.5 (14–79) and a weighted median Coleman-score of 42.5 points. All classifications achieved a substantial to perfect score regarding the inter- and intraobserver reliability, with Mason scoring the lowest in comparison.
Conclusions
None of the reviewed PMF classifications has been able to establish itself decisively in the literature. Most of the classifications are insufficient in terms of a derivable treatment algorithm or a prognosis with regard to outcome. However, as the Bartoníček/Rammelt classification has the greatest potential due to its treatment algorithm, its reliability in combination with consistent predictive values, its usage in clinical practice and research appears advisable.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Ankle fractures present as one of the most common fractures with a prevalence of 4–9% [1, 2]. Posterior malleolar fracture (PMF), also known as malleolus tertius, posterior tibial fracture, or Volkmann-fragment appears in up to 44% of ankle fractures [3,4,5]. If the posterior malleolus is affected, therapy results may be worse and its presence in ankle fractures is known to be of negative prognostic value [1, 4, 6,7,8,9,10].
Decision-making to fixate PMF is still highly debatable and traditionally often based on fracture size measurement on radiographs, with lack of accuracy and poor reliability [11,12,13,14,15,16,17,18]. Nowadays, it is generally believed that the morphology of the fragment is more closely related to the fracture pattern and is, therefore, more important in classifying the fracture [14, 19,20,21]. Consequently, with regard to the proportion of the affected joint surface and recommendation for surgical fixation of PMF, there is a shift away from the 1/3 dogma [7, 17, 22,23,24,25,26,27,28]. With increasing understanding of fracture morphology and the routine use of computed tomography (CT), efforts have been made in recent years to establish new classification systems based on CT imaging [14, 29, 30]. Until now, there is no international consensus regarding classification and treatment of PMF [24, 31, 32].
A good classification system helps the orthopedic surgeon to identify and characterize a problem, suggest a potential prognosis, and offer guidance in determining the appropriate treatment method for a particular condition. To achieve optimal therapeutic results, a complete understanding of the morphology is indispensable.
Therefore, the aims of this systematic review were first, to determine how many studies use a classification of the PMF; second, to identify and to describe which classifications of PMF exist; third to examine which classification system does have the most reliable (inter- and intra- observer) scores; and fourth, to evaluate the predictive value of the classifications in terms of postoperative outcomes.
Materials and methods
Search strategy
The study protocol was registered in the PROSPERO database (CRD42021264268). The review was performed and reported according to the PRISMA 2020 checklist [33].
The electronic databases of the Cochrane Central Register of Controlled Trials, MEDLINE via PubMed and Scopus were searched systematically. The search was performed on the 20th of March 2021. The following search algorithm was used: (posterior AND ankle AND fracture) OR (posterior AND (malleolus OR malleolar) AND fracture) OR (ankle AND volkmann) OR (trimalleolar AND fracture) OR (posterior AND pilon AND fracture). A final update of the search was conducted 12th of May 2022 using the same search string. Furthermore, reference lists of relevant reviews and included articles were screened for additional articles. Bidirectional citation search was used including backward and forward citation search methods [34]. There were no limitations on journal or publication date of the article.
Study selection
Studies reporting data on classification systems of trimalleolar ankle fractures were screened for using a PMF classification. Inclusion and exclusion criteria were cross checked by three reviewers (HW, JT, EM), first by screening the title and abstract, second by reading the full text. Clinical studies were included for data extraction. Cadaveric studies, review articles, case reports with fewer than 10 cases, studies that did not include a posterior malleolus specific classification, and studies not written in English, were excluded.
Data extraction
The study selection and data extraction were independently performed by two review authors (JT, EM). Disagreements were discussed in a consensus meeting and if a disagreement persisted, a third reviewer (HW) made the final decision. Data were extracted from the included studies using a Microsoft Office® Excel spreadsheet. This included the following data: study design, sample size and source, fragment characteristics (e.g., classification, displacement, treatment), reliability- and validity scores and additional data the classification addressed, like treatment allocation and prognostic value of it, were collected. Names of used classification system were listed and their frequency in use was counted.
Study quality assessment
The methodological quality of the included studies was quantified using a modified Coleman score [35]. The modified Coleman score was applied by two independent reviewers (HW, JT) (Online Resource 1). The score is composed of two parts. Part A assesses study size, average follow-up time, percentage of patients with follow-up, number of interventions, study type, diagnostic certainty, description of surgical method, and postoperative rehabilitation. Part B is comprised of outcome criteria, procedure for assessing outcomes, and description of the subject selection process. The maximum score to be achieved is 100 points.
Statistical analysis
The data were processed descriptively, therefore, no meta-analysis was performed. Patient demographic characteristics (number of patients/feet, patient age and sex) were summarized. Weighted median scores were calculated for the modified Coleman score and for the age of the evaluated patient cohort. Data analysis was performed using IBM SPSS Statistics Version 26.0 (IBM Corp., Armonk, NY, USA). The kappa values of inter- and intraobserver reliability were interpreted as defined by Landis and Koch (< 0.20: slight, 0.21–0.40: fair, 0.41–0.60: moderate, 0.61–0.80: substantial, 0.81–1.00: almost perfect) [36].
Results
Included studies
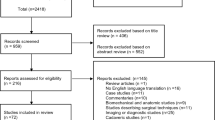
Evaluation of the databases revealed 3.377 studies potentially relevant for inclusion. After excluding duplicates, title and abstract of the remaining studies were assessed. 380 studies were eligible for full-text analysis, after applying the exclusion criteria (no clinical study, case reports < 10 patients, no classification/no PMF-specific classification), 110 remaining relevant studies were included in this review. The selection process was performed according to “Preferred Reporting Items for Systematic Review and Meta-Analyses” (PRISMA) and is shown in Fig. 1 [33].

PRISMA flow chart
Study characteristics
A total of 110 studies, published between 1965 and 2022, using 143 classification systems, were included. The studies include a number of 12.614 patients with 12.633 ankle fractures and a weighted median age of 44.55 years (13–100). 5.963 patients were female and 5.231 male, 11 studies did not report gender distribution [6, 20, 24, 37,38,39,40,41,42,43,44]. There were 22 prospective studies, 88 retrospective studies; 11 studies were multicenter, and 99 single center studies (Table 1). Detailed information about patient demographics is demonstrated in Table 2. Four specific classifications for the PMF were found: a classification based on the relation of the fragment size compared to the size of the tibial joint surface [45] (referred to as PMF Classification according to fracture size) and 3 CT-based classifications according to Haraguchi, Bartoníček/Rammelt, and Mason [14, 29, 30].
PMF classification according to fracture size
Sixty-six studies that used the size of the PMF in relation to the joint surface as a classification could be included. Of these, 35 studies used radiographs and 30 studies used CT to estimate size, one study did not provide a clear statement in this regard. Only one studied inter- and intraobserver reliability, measuring a substantial Kappa of 0.64 and 0.63 respectively [13]. The majority of these studies used either a cut-off value of 25% for fixation of the PMF (26 studies) or fixed the posterior malleolus regardless of size (28 studies). The remaining studies used either 20% (4 studies), 30% (2 studies), or > 1/3 of the joint area (5 studies) as the cut-off value, 1 study fixed the PMF in young patients or in the presence of subluxation from 10%, and 3 studies did not provide any information (Table 3). Nine studies reported a better outcome with reduction of smaller posterior malleolus fragments [4, 6, 7, 46,47,48,49,50,51], whereas seven studies reported no difference between fixation and no fixation of smaller posterior malleolus fragments [52,53,54,55,56,57,58].
Haraguchi classification
The first CT-based classification found, was developed 2006 by Haraguchi et al. which classified PMF into 3 distinct types [14]. Type I is described as a posterolateral-oblique wedge-shaped fragment involving the posterolateral corner of the tibial plafond, type II as a transverse medial-extension fracture line extending from the fibular notch to the medial malleolus, and type III is characterized as a small-shell type fragment at the posterior lip of the tibial plafond (Fig. 2). So far, Haraguchi's classification has been mentioned in 101 studies and was applied in 44 of them, which were, therefore, included and can be seen in Table 4. Three studies reported on the reliability of the classification, all showing substantial interobserver reliability (Fleiss kappa 0.70/Cohen’s kappa 0.799/Cohen’s kappa 0.797) and substantial to almost perfect intraobserver reliability (Fleiss kappa 0.77/Cohen’s kappa 0.985) [24, 32, 59]. Modifications of the Haraguchi classification were found three times. Kumar et al. divided Haraguchi type II into subtype A: a single fracture line extending from the fibular notch of the tibia to the medial malleolus, and subtype B: a posterior fracture lines forming 2 separate fragments, which was also applied by Sheikh et al. [60]. Wang et al. also modified Haraguchi type II by categorizing the fracture line into an anterolateral oblique line (subtype I) and into a small avulsion (subtype II) [61]. Palmanovich et al. divided the posterior segment by a central line, perpendicular to the bimalleolar line, into medial and lateral sub-segments, creating a 4-quadrant grid; each posterior malleolar fracture was then categorized based on the fragment’s location into “postero-lateral”, “postero-medial” and “postero-central” [62]. In terms of predictive values, type II fractures were regarded to show worse outcome [19, 59, 63], have higher presence of osteoarthritis [59], and are more likely to require placement of 2 syndesmotic screws [41]. The use of a posteromedial approach for type II fractures have resulted in good Olerud and Molander ankle score (OMAS)[64]. Mertens et al. observed an improving AOFAS score from type I to type III [65], Xie et al. found most intercalary fragments (more than 2/3) in type I fractures [28], and Kang et al. reported a better outcome with surgical treatment of type I fractures smaller than 25% [49].

Overview of the Haraguchi classification based on CT images (axial views). a Haraguchi type I b Haraguchi type II c Haraguchi type III
Bartoníček/Rammelt classification
Another CT-based classification was presented by Bartoníček/Rammelt in 2015 [29]. Five different fracture types were defined: type 1 as an extraincisural fragment with intact fibula notch, type 2 as a posterolateral fragment including the fibula notch, a posteromedial two-part fragment extending to the medial malleolus as type 3 fracture, a posterolateral fragment larger than one-third of the notch as type 4 fracture, and finally irregular osteoporotic fragments as type 5 fracture (Fig. 3). It also includes a treatment algorithm. The Bartoníček/Rammelt classification has been found 46 times in the literature, of these, 21 studies have used it as a classification system, which were included in this study and are shown in Table 5. There is one modification made by Tucek et al., who divided Bartoníček type 4 into three subtypes: subtype 1 as a fracture line that passes laterally past the malleolar groove, subtype 2 as a fracture line that involves the malleolar groove, and subtype 3 as an intercollicular fracture line or a line involving the posterior colliculus [66]. Two studies reported reliability of the classification, both showing substantial interobserver reliability (Fleiss kappa 0.78/Cohen’s kappa 0.744) and almost perfect intraobserver reliability (Fleiss kappa 0.81/Cohen’s kappa 0.936) [24, 32]. Regarding the predictive outcome value, type 1 fractures showed to have better outcome than type 2 fractures [65], and a significantly improved clinical outcome was achieved in type 4 fractures when they were surgically fixed [54]. With increasing fracture type, clinical outcome became worse [1, 21, 63].

Overview of the Bartoníček/Rammelt classification based on CT images (axial views). a Bartoníček type 1 b Bartoníček type 2 c Bartoníček type 3 d Bartoníček type 4
Mason classification
In 2017, Mason et al. developed a CT-based classification of PMF ascending in severity of injury [30]. Therefore, Mason described type 1 as an extra-articular avulsion fracture following a rotational force applied to the foot when the ankle is in plantarflexion and the talus unloaded. Rotational forces applied to a loaded foot result in a type 2A fracture in form of a primary triangular posterolateral fragment. A type 2B fracture with a secondary posteromedial fragment, usually angled at 45° to the primary fragment, occurs when the talus continues to rotate in the mortise. A type 3 fracture is characterized by a coronal fracture line that involves the entire posterior plafond due to an axial loading of a plantarflexed talus (Fig. 4). Until now, Mason's classification has been mentioned 22 times in literature, and used for classification in 12 studies, which were included and can be found in Table 6. One modification of Mason type 2B fracture was found. Vosoughi et al. divided it into a large intra-articular pilon fragment and a small extra-articular fragment [67]. Interobserver reliability ranged from substantial to almost perfect values (Cohen’s kappa 0.919/Fleiss kappa 0.61/Cohen’s kappa 0.717) as did intraobserver reliability (Fleiss kappa 0.65/Cohen’s kappa 0.957) [24, 30, 32]. As for the predictive outcome value, type 3 fractures tend to show worse postoperative outcome [68].

Overview of the Mason classification based on CT images (axial views). a Mason type 1 b Mason type 2A c Mason type 2B d Mason type 3
Quality assessment of included studies
The Coleman score achieved a total median value of 43.5 points (14–79), composed of Part A with a median of 26 points, and Part B with 18 points. Based on the number of patients included, the weighted median total Coleman score was 42.5. Coleman score points are shown in Table 1.
Discussion
By reviewing the literature, 4 classifications were found describing PMF: a classification based on the fragment proportion in relation to the distal tibial joint surface [45] and the three CT-based classifications according to Haraguchi, Bartoníček/Rammelt, and Mason [14, 29, 30]. The earliest and most commonly used classification was the PMF Classification according to fracture size as first specified by Nelson and Jensen, who postulate a recommendation for treatment of PMF with a fragment size exceeding more than 1/3 of the articular surface on lateral radiographs based on a study sample consisting of 8 patients [45]. With 66 included studies, this classification accounts for the largest proportion of classifications used by surgeons in clinical practice. In the included studies the most used cut-off value was 25%, but also values of 20%, 30% or 1/3 of the articular surface were used.
There are still controversial opinions for osteosynthetic treatment of PMF [69]: McDaniel and Wilson demonstrated, that if a PMF of less than 25% of the tibial joint area was not reduced, it did not significantly affect the overall outcome [58]. De Vries et al. and Xu et al. found no evidence for fixing PMF smaller than 25%, as outcome scoring systems showed no significant better outcome [52, 53], as well as Guo et al. for PMF in tibial spiral fractures [54]. Comparing the outcome of treating PMF less than 25% with that of not fixing it no significant difference in the AOFAS Score was found [55,56,57]. On the other hand, a trend toward better clinical and radiological outcome in patients in whom PMF was fixed was observed and, therefore, authors recommend PMF fixation of even smaller fragments that cannot be satisfactorily reduced by ligamentotaxis [6, 46, 47, 49, 50]. Baumbach et al. and Tosun et al. postulated even that in PMF of all sizes, syndesmotic stability is significantly more likely to be restored if treated by open reduction internal fixation [48, 51]. In relation to the total number of studies using this classification, the number of studies in terms of predictive outcome values is rather limited. In the matter of inter- and intraobserver reliability, the available evidence is also meager, Büchler et al. were the only ones to study this, providing good results with an inter- and intraobserver reliability of kappa of 0.64 and 0.63, respectively [13]. Of all studies that asses the PMF classification according to fracture size, all but two [6, 49] are of retrospective design. Especially in the earlier studies, the evaluation of the fracture was not optimal, since this was done mainly on the basis of lateral radiographs.
The use of radiographs was found to be limited for the accurate size estimation of PMF [12, 14, 18, 70], therefore, it recently came to the increasing use of computed tomography (CT) in the diagnosis of trimalleolar ankle fractures [18, 47, 54]. Subsequently, the conviction increases that not the size, but the fracture morphology is crucial for the improvement of outcome [19]. Factors such as syndesmotic stability, joint congruity, postoperative step-off, reconstruction of the incisura, intercalary fragments and talar subluxation are thought to be of prognostic importance to consider when treating PMF [7, 23, 48, 50, 51, 53, 58, 63, 71,72,73,74,75,76]. Hence, a paradigm shift has occurred [21, 24, 31, 77], as also the systematic review by Odak et al. has previously shown [22].
This is where the three CT-based classifications come to the fore. The classification used in the majority of studies is the one proposed by Haraguchi [14]. Most probably due to being the first CT-based classification and due to the simple and clear structure dividing the fracture in three types. Since 2015, however, a preference for the Bartoníček/Rammelt classification has emerged, with the main strengths of this classification being the ascending severity of the classification and the derived therapy recommendations [29]. After noting that the Haraguchi classification did not map the mechanism of injury, Mason developed the most recent classification, also considering the injury mechanism [30].
Some objections against Haraguchi’s classification have arisen with the time. First, the classification is not based on severity and thus does not relate to functional outcome [78]. Second, that the classification was based only on axial sectional images and, therefore, fractures were only assessed in one plane, vertical size expansion not being estimated [31], that medial injuries were not evaluated, which may lead to misjudgments [17, 32], and that the extent of involvement of the tibial incisura was not specified, wherefore type I fractures include a wide range of both small and large posterolateral fragments [59]. Most multi-fragmentary fractures cannot be defined using this classification [79]. Also, the three modifications found [61, 62, 80] may suggest that Haraguchi’s classification is not as advanced to represent all fracture types. Regarding the predictive value of the classifications in terms of postoperative outcomes, some authors have shown that type II fractures have worse clinical outcomes [19, 59, 63], whereas Mertens et al. observed an improvement in the AOFAS score from type I to type III [65].
The Bartoníček/Rammelt classification was developed on the basis of a larger patient population. It ascends in severity and contains a therapy recommendation [29, 81]. Zhang et al. were able to show that the potency of the Bartoníček/Rammelt classification also applies to distal tibial spiral fractures with associated PMF [82]. One objection is the imprecise definition of type 5 fractures, which includes all fractures that cannot be classified as type 1–4. We were not able to find an image of such a type 5 fracture: neither in the original article nor in our own fracture-database. Another objection is the difficulty of estimating 1/3 of the tibial incision to distinguish between a type 2 and type 4 fracture [32]. There is a consistent opinion on worse outcome with increasing fracture type [1, 63, 65]. Only Neumann et al. saw an increase in the AOFAS score and no difference in the Olerud and Molander ankle score (OMAS) [21].
The authors of the Mason classification see the advantage in the ascending degree of severity of the classification considering the accident mechanism. They have also introduced treatment recommendations based on their classification. Gandham et al. even made a recommendation on the appropriate operative approaches [30, 68, 83]. However, they described the classification using schematic drawings and also do not define the tibial incisura [32]. In addition, a multi-fragmentary fracture of the entire tibial plafond may be mistaken for a two-part posterolateral and posteromedial fracture (type 2B) [32]. With the exception of one study describing a worse outcome in Mason type 3 fractures [68], there are no further statements on predictive values. Until now, Mason’s classification has not yet been able to establish itself in literature with only 12 included studies. In addition, half of all studies using Mason’s classification were conducted by the author's own research group, and it was Mason himself who found the highest interobserver reliability in his study (kappa 0.919) whereas other authors found considerable lower reliability scores (Fleiss kappa 0.61 / Cohen’s kappa 0.717) [24, 30, 32, 43, 44, 67, 68, 83].
Intra- and interobserver reliability are substantial to perfect for all classifications, with Mason scoring the lowest in comparison to the other classifications [24, 32]. However, none of the classifications can adequately describe the complexity of posterior malleolus fracture, as factors such as extent of articular surface impaction, degree of dislocation or intercalary fragments among others are not taken into account [32, 79].
Several important classifications were excluded because they are not PMF-specific. This includes the AO classification originally published in 1987 by Müller/AO, being a universal classification depicting all skeletal injuries. It is a valuable, international classification, which has its justification, and which has been used for years [84, 85]. With the routine use of CT imaging to reliably diagnose and classify trimalleolar fractures [9], authors have shown that all fractures involve the articular surface of the distal tibia [14, 29, 81]. This in contrast to the specification of the AO’s classification through Heim, dividing posterior malleolar fractures into extra- and intra-articular fractures [86]. The AO classification, based on standard plain radiographs, is therefore not suitable for considering the significance and morphology of PMF, nor is it applicable in addressing specific questions regarding PMFs [24, 48, 87].
Classification systems of posterior pilon fractures were also considered to be non-PMF-specific. Hence, the differentiation of pilon fractures from trimalleolar ankle fractures still often causes difficulties in clinical practice [75, 88, 89]. This has led to the emergence of a subset of PMF, also known as the “posterior pilon” variant, which has recently gained popularity [61, 87, 90,91,92,93]. However, there is still no clear definition and the understanding of it varies [75, 81, 94, 95]. In addition, there are studies showing that posterior pilon fractures are a separate entity due to morphological differences [61, 94].
Other excluded classifications were sub-entities of PMF fractures. For example, a classification of PMF in tibial shaft fractures (TSF) [96, 97], and one also involving talar subluxation [98].
A few more limitations are worth noting, with majorly the limited quality of the included studies. Limitations affecting the Coleman score include the predominantly retrospective nature of the included studies and small patient cohorts. Therefore, the results of this study could only be presented in a descriptive manner. Only studies written in English were considered, excluding further useful contributions written in other languages.
In conclusion, this review demonstrates that there has been a shift from usage of the PMF classification by fracture size to the newer CT-based classifications, however, none have been able to establish itself in the literature so far. Summarizing all of the previously described points, we believe that, to date, no classification is able to adequately describe the complexity of the PMF. Also, the classifications are weak in terms of a derivable treatment algorithm or prognosis of outcome. According to this review, the Bartoníček/Rammelt classification has the most potential to prevail in the literature and in clinical practice due to its treatment algorithm, its reliability in combination with consistent predictive outcome values.
References
Maluta T, Samaila EM, Amarossi A, Dorigotti A, Ricci M, Vecchini E, Magnan B (2021) Can treatment of posterior malleolus fractures with tibio-fibular instability be usefully addressed by Bartonicek classification? Foot Ankle Surg. https://doi.org/10.1016/j.fas.2021.02.009
Elsoe R, Ceccotti AA, Larsen P (2018) Population-based epidemiology and incidence of distal femur fractures. Int Orthop 42(1):191–196. https://doi.org/10.1007/s00264-017-3665-1
Court-Brown CM, McBirnie J, Wilson G (1998) Adult ankle fractures–an increasing problem? Acta Orthop Scand 69(1):43–7. https://doi.org/10.3109/17453679809002355
Jaskulka RA, Ittner G, Schedl R (1989) Fractures of the posterior tibial margin: their role in the prognosis of malleolar fractures. J Trauma 29(11):1565–70. https://doi.org/10.1097/00005373-198911000-00018
Koval KJ, Lurie J, Zhou W, Sparks MB, Cantu RV, Sporer SM, Weinstein J (2005) Ankle fractures in the elderly: what you get depends on where you live and who you see. J Orthop Trauma 19(9):635–9. https://doi.org/10.1097/01.bot.0000177105.53708.a9
Tejwani NC, Pahk B, Egol KA (2010) Effect of posterior malleolus fracture on outcome after unstable ankle fracture. J Trauma 69(3):666–9. https://doi.org/10.1097/TA.0b013e3181e4f81e
Langenhuijsen JF, Heetveld MJ, Ultee JM, Steller EP, Butzelaar RM (2002) Results of ankle fractures with involvement of the posterior tibial margin. J Trauma 53(1):55–60. https://doi.org/10.1097/00005373-200207000-00012
Broos PL, Bisschop AP (1991) Operative treatment of ankle fractures in adults: correlation between types of fracture and final results. Injury 22(5):403–6. https://doi.org/10.1016/0020-1383(91)90106-o
Roberts V, Mason LW, Harrison E, Molloy AP, Mangwani J (2019) Does functional outcome depend on the quality of the fracture fixation? Mid to long term outcomes of ankle fractures at two university teaching hospitals. Foot Ankle Surg 25(4):538–541. https://doi.org/10.1016/j.fas.2018.04.008
Regier M, Petersen JP, Hamurcu A, Vettorazzi E, Behzadi C, Hoffmann M, Grossterlinden LG, Fensky F, Klatte TO, Weiser L, Rueger JM, Spiro AS (2016) High incidence of osteochondral lesions after open reduction and internal fixation of displaced ankle fractures: Medium-term follow-up of 100 cases. Injury 47(3):757–61. https://doi.org/10.1016/j.injury.2015.10.029
Ebraheim NA, Mekhail AO, Haman SP (1999) External rotation-lateral view of the ankle in the assessment of the posterior malleolus. Foot Ankle Int 20(6):379–83. https://doi.org/10.1177/107110079902000607
Ferries JS, DeCoster TA, Firoozbakhsh KK, Garcia JF, Miller RA (1994) Plain radiographic interpretation in trimalleolar ankle fractures poorly assesses posterior fragment size. J Orthop Trauma 8(4):328–31. https://doi.org/10.1097/00005131-199408000-00009
Buchler L, Tannast M, Bonel HM, Weber M (2009) Reliability of radiologic assessment of the fracture anatomy at the posterior tibial plafond in malleolar fractures. J Orthop Trauma 23(3):208–12. https://doi.org/10.1097/BOT.0b013e31819b0b23
Haraguchi N, Haruyama H, Toga H, Kato F (2006) Pathoanatomy of posterior malleolar fractures of the ankle. J Bone Joint Surg Am 88(5):1085–92. https://doi.org/10.2106/JBJS.E.00856
Magid D, Michelson JD, Ney DR, Fishman EK (1990) Adult ankle fractures: comparison of plain films and interactive two- and three-dimensional CT scans. AJR Am J Roentgenol 154(5):1017–23. https://doi.org/10.2214/ajr.154.5.2108536
Yao L, Zhang W, Yang G, Zhu Y, Zhai Q, Luo C (2014) Morphologic characteristics of the posterior malleolus fragment: a 3-D computer tomography based study. Arch Orthop Trauma Surg 134(3):389–94. https://doi.org/10.1007/s00402-013-1844-0
Meijer DT, Doornberg JN, Sierevelt IN, Mallee WH, van Dijk CN, Kerkhoffs GM, Stufkens SA, Ankle Platform Study Collaborative—Science of Variation G (2015) Guesstimation of posterior malleolar fractures on lateral plain radiographs. Injury 46(10):2024–9. https://doi.org/10.1016/j.injury.2015.07.019
Stringfellow TD, Walters ST, Nash W, Ahluwalia R, Posterior Malleolus Study G (2021) Management of posterior malleolus fractures: a multicentre cohort study in the United Kingdom. Foot Ankle Surg 27(6):629–635. https://doi.org/10.1016/j.fas.2020.08.003
Blom RP, Meijer DT, de Muinck Keizer RO, Stufkens SAS, Sierevelt IN, Schepers T, Kerkhoffs G, Goslings JC, Doornberg JN (2019) Posterior malleolar fracture morphology determines outcome in rotational type ankle fractures. Injury 50(7):1392–1397. https://doi.org/10.1016/j.injury.2019.06.003
Mangnus L, Meijer DT, Stufkens SA, Mellema JJ, Steller EP, Kerkhoffs GM, Doornberg JN (2015) Posterior malleolar fracture patterns. J Orthop Trauma 29(9):428–35. https://doi.org/10.1097/BOT.0000000000000330
Neumann AP, Rammelt S (2021) Ankle fractures involving the posterior malleolus: patient characteristics and 7-year results in 100 cases. Arch Orthop Trauma Surg. https://doi.org/10.1007/s00402-021-03875-3
Odak S, Ahluwalia R, Unnikrishnan P, Hennessy M, Platt S (2016) Management of posterior malleolar fractures: a systematic review. J Foot Ankle Surg 55(1):140–5. https://doi.org/10.1053/j.jfas.2015.04.001
Gardner MJ, Streubel PN, McCormick JJ, Klein SE, Johnson JE, Ricci WM (2011) Surgeon practices regarding operative treatment of posterior malleolus fractures. Foot Ankle Int 32(4):385–93. https://doi.org/10.3113/FAI.2011.0385
Pfluger P, Harder F, Muller K, Biberthaler P, Cronlein M (2022) Evaluation of ankle fracture classification systems in 193 trimalleolar ankle fractures. Eur J Trauma Emerg Surg. https://doi.org/10.1007/s00068-022-01959-2
Evers J, Fischer M, Raschke M, Riesenbeck O, Milstrey A, Gehweiler D, Gueorguiev B, Ochman S (2021) Leave it or fix it? How fixation of a small posterior malleolar fragment neutralizes rotational forces in trimalleolar fractures. Arch Orthop Trauma Surg. https://doi.org/10.1007/s00402-021-03772-9
Weigelt L, Hasler J, Flury A, Dimitriou D, Helmy N (2020) Clinical and radiological mid- to long-term results after direct fixation of posterior malleolar fractures through a posterolateral approach. Arch Orthop Trauma Surg 140(11):1641–1647. https://doi.org/10.1007/s00402-020-03353-2
Mak MF, Stern R, Assal M (2018) Repair of syndesmosis injury in ankle fractures: current state of the art. EFORT Open Rev 3(1):24–29. https://doi.org/10.1302/2058-5241.3.170017
Xie W, Lu H, Xu H, Quan Y, Liu Y, Fu Z, Zhang D, Jiang B (2021) Morphological analysis of posterior malleolar fractures with intra-articular impacted fragment in computed tomography scans. J Orthop Traumatol 22(1):52. https://doi.org/10.1186/s10195-021-00615-6
Bartonicek J, Rammelt S, Kostlivy K, Vanecek V, Klika D, Tresl I (2015) Anatomy and classification of the posterior tibial fragment in ankle fractures. Arch Orthop Trauma Surg 135(4):505–16. https://doi.org/10.1007/s00402-015-2171-4
Mason LW, Marlow WJ, Widnall J, Molloy AP (2017) Pathoanatomy and Associated Injuries of Posterior Malleolus Fracture of the Ankle. Foot Ankle Int 38(11):1229–1235. https://doi.org/10.1177/1071100717719533
Bartonicek J, Rammelt S, Tucek M (2017) Posterior malleolar fractures: changing concepts and recent developments. Foot Ankle Clin 22(1):125–145. https://doi.org/10.1016/j.fcl.2016.09.009
Kleinertz H, Mueller E, Tessarzyk M, Frosch KH, Schlickewei C (2022) Computed tomography-based classifications of posterior malleolar fractures and their inter- and intraobserver reliability: a comparison of the Haraguchi, Bartonicek/Rammelt, and Mason classifications. Arch Orthop Trauma Surg. https://doi.org/10.1007/s00402-021-04315-y
Moher D, Liberati A, Tetzlaff J, Altman DG, Group P (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6(7):e1000097. https://doi.org/10.1371/journal.pmed.1000097
Hinde S, Spackman E (2015) Bidirectional citation searching to completion: an exploration of literature searching methods. Pharmacoeconomics 33(1):5–11. https://doi.org/10.1007/s40273-014-0205-3
Coleman BD, Khan KM, Maffulli N, Cook JL, Wark JD (2000) Studies of surgical outcome after patellar tendinopathy: clinical significance of methodological deficiencies and guidelines for future studies. Victorian Institute of Sport Tendon Study Group. Scand J Med Sci Sports 10(1):2–11. https://doi.org/10.1034/j.1600-0838.2000.010001002.x
Landis JR, Koch GG (1977) The measurement of observer agreement for categorical data. Biometrics 33(1):159–74
Warner WC, Farber LA (1965) Trimalleolar fractures. South Med J 58(10):1292–5. https://doi.org/10.1097/00007611-196510000-00022
Olerud C, Molander H (1986) Bi- and trimalleolar ankle fractures operated with nonrigid internal fixation. Clin Orthop Relat Res 206:253–60
Heim D, Schmidlin V, Ziviello O (2002) Do type B malleolar fractures need a positioning screw? Injury 33(8):729–34. https://doi.org/10.1016/s0020-1383(01)00199-1
de Muinck Keizer RO, Meijer DT, van der Gronde BA, Teunis T, Stufkens SA, Kerkhoffs GM, Goslings JC, Doornberg JN (2016) Articular gap and step-off revisited: 3D quantification of operative reduction for posterior malleolar fragments. J Orthop Trauma 30(12):670–675. https://doi.org/10.1097/BOT.0000000000000676
Sobol GL, Shaath MK, Reilly MC, Adams MR, Sirkin MS (2018) The incidence of posterior malleolar involvement in distal spiral tibia fractures: is it higher than we think? J Orthop Trauma 32(11):543–547. https://doi.org/10.1097/BOT.0000000000001307
Mitchell PM, Harms KA, Lee AK, Collinge CA (2019) Morphology of the posterior malleolar fracture associated with a spiral distal tibia fracture. J Orthop Trauma 33(4):185–188. https://doi.org/10.1097/BOT.0000000000001398
Jayatilaka MLT, Philpott MDG, Fisher A, Fisher L, Molloy A, Mason L (2019) Anatomy of the insertion of the posterior inferior tibiofibular ligament and the posterior malleolar fracture. Foot Ankle Int 40(11):1319–1324. https://doi.org/10.1177/1071100719865896
Philpott MDG, Jayatilaka MLT, Millward G, Molloy A, Mason L (2020) Posterior approaches to the ankle—an analysis of 3 approaches for access to the posterior malleolar fracture. Foot (Edinb) 45:101725. https://doi.org/10.1016/j.foot.2020.101725
Nelson M, Jensen N (1940) The treatment of trimalleolar fractures of the ankle. Surg Gynecol Obstet 71:509–514
Mingo-Robinet J, Lopez-Duran L, Galeote JE, Martinez-Cervell C (2011) Ankle fractures with posterior malleolar fragment: management and results. J Foot Ankle Surg 50(2):141–5. https://doi.org/10.1053/j.jfas.2010.12.013
Evers J, Barz L, Wahnert D, Gruneweller N, Raschke MJ, Ochman S (2015) Size matters: the influence of the posterior fragment on patient outcomes in trimalleolar ankle fractures. Injury 46(4):S109–S113. https://doi.org/10.1016/S0020-1383(15)30028-0
Baumbach SF, Herterich V, Damblemont A, Hieber F, Bocker W, Polzer H (2019) Open reduction and internal fixation of the posterior malleolus fragment frequently restores syndesmotic stability. Injury 50(2):564–570. https://doi.org/10.1016/j.injury.2018.12.025
Kang C, Hwang DS, Lee JK, Won Y, Song JH, Lee GS (2019) Screw fixation of the posterior malleolus fragment in ankle fracture. Foot Ankle Int 40(11):1288–1294. https://doi.org/10.1177/1071100719865895
McHale S, Williams M, Ball T (2020) Retrospective cohort study of operatively treated ankle fractures involving the posterior malleolus. Foot Ankle Surg 26(2):138–145. https://doi.org/10.1016/j.fas.2019.01.003
Tosun B, Selek O, Gok U, Ceylan H (2018) Posterior malleolus fractures in trimalleolar ankle fractures: malleolus versus transyndesmal fixation. Indian J Orthop 52(3):309–314. https://doi.org/10.4103/ortho.IJOrtho_308_16
De Vries JS, Wijgman AJ, Sierevelt IN, Schaap GR (2005) Long-term results of ankle fractures with a posterior malleolar fragment. J Foot Ankle Surg 44(3):211–7. https://doi.org/10.1053/j.jfas.2005.02.002
Xu HL, Li X, Zhang DY, Fu ZG, Wang TB, Zhang PX, Jiang BG, Shen HL, Wang G, Wang GL, Wu XB (2012) A retrospective study of posterior malleolus fractures. Int Orthop 36(9):1929–36. https://doi.org/10.1007/s00264-012-1591-9
Guo J, Liu L, Yang Z, Hou Z, Chen W, Zhang Y (2017) The treatment options for posterior malleolar fractures in tibial spiral fractures. Int Orthop 41(9):1935–1943. https://doi.org/10.1007/s00264-016-3388-8
Saygılı MS, Özkul B, Çetinkaya E, Tekin AC, Bayhan AI, Kalkar I, Akbulut D, Demir B (2017) Operative versus non-operative treatment of posterior malleolus fragment in trimalleolar fracture: a retrospective cohort study. Biomed Res 28(14):6498–6503
Pilskog K, Gote TB, Odland HEJ, Fjeldsgaard KA, Dale H, Inderhaug E, Fevang JM (2021) Traditional approach vs posterior approach for ankle fractures involving the posterior malleolus. Foot Ankle Int 42(4):389–399. https://doi.org/10.1177/1071100720969431
Yamamoto N, Iwamoto K, Tomita Y, Iwamoto Y, Kiyono M, Yoshimura M, Noda T, Kawasaki K, Ozaki T (2022) Pre-and postoperative factors associated with functional outcomes in patients with posterior malleolar fractures. Injury. https://doi.org/10.1016/j.injury.2022.02.046
McDaniel WJWilson FC (1977) Trimalleolar fractures of the ankle. An end result study. Clin Orthop Relat Res (122):37–45.
Raeder BW, Andersen MR, Madsen JE, Jacobsen SB, Frihagen F, Figved W (2021) Prognostic value of the Haraguchi classification in posterior malleolar fractures in A0 44-C type ankle fractures. Injury 52(10):3150–3155. https://doi.org/10.1016/j.injury.2021.07.038
Sheikh HQ, Mills EJ, McGregor-Riley JC, Chadwick C, Davies MB (2020) The effect of computerised tomography on operative planning in posterior malleolus ankle fractures. Foot Ankle Surg 26(6):676–680. https://doi.org/10.1016/j.fas.2019.08.007
Wang J, Wang X, Xie L, Zheng W, Chen H, Cai L (2020) Comparison of radiographs and CT features between posterior Pilon fracture and posterior malleolus fracture: a retrospective cohort study. Br J Radiol 93(1110):20191030. https://doi.org/10.1259/bjr.20191030
Palmanovich E, Ohana N, Yaacobi E, Segal D, Iftach H, Sharfman ZT, Vidra M, Atzmon R (2020) Preoperative planning and surgical technique for optimizing internal fixation of posterior malleolar fractures: CT versus standard radiographs. J Orthop Surg Res 15(1):119. https://doi.org/10.1186/s13018-020-01637-2
Blom RP, Hayat B, Al-Dirini RMA, Sierevelt I, Kerkhoffs G, Goslings JC, Jaarsma RL, Doornberg JN, Group EFX-tS (2020) Posterior malleolar ankle fractures. Bone Joint J 102-B(9):1229–1241. https://doi.org/10.1302/0301-620X.102B9.BJJ-2019-1660.R1
Bali N, Aktselis I, Ramasamy A, Mitchell S, Fenton P (2017) An evolution in the management of fractures of the ankle: safety and efficacy of posteromedial approach for Haraguchi type 2 posterior malleolar fractures. Bone Joint J 99-B(11):1496–1501. https://doi.org/10.1302/0301-620X.99B11.BJJ-2017-0558.R1
Mertens M, Wouters J, Kloos J, Nijs S, Hoekstra H (2020) Functional outcome and general health status after plate osteosynthesis of posterior malleolus fractures—the quest for eligibility. Injury 51(4):1118–1124. https://doi.org/10.1016/j.injury.2020.02.109
Tucek M, Rammelt S, Kostlivy K, Bartonicek J (2021) CT controlled results of direct reduction and fixation of posterior malleolus in ankle fractures. Eur J Trauma Emerg Surg 47(4):913–920. https://doi.org/10.1007/s00068-020-01309-0
Vosoughi AR, Jayatilaka MLT, Fischer B, Molloy AP, Mason LW (2019) CT analysis of the posteromedial fragment of the posterior malleolar fracture. Foot Ankle Int 40(6):648–655. https://doi.org/10.1177/1071100719830999
Mason LW, Kaye A, Widnall J, Redfern J, Molloy A (2019) Posterior malleolar ankle fractures: an effort at improving outcomes. JB JS Open Access 4(2):e0058. https://doi.org/10.2106/JBJS.OA.18.00058
Veltman ES, Halma JJ, de Gast A (2016) Longterm outcome of 886 posterior malleolar fractures: a systematic review of the literature. Foot Ankle Surg 22(2):73–7. https://doi.org/10.1016/j.fas.2015.05.003
Abdelgawad AA, Kadous A, Kanlic E (2011) Posterolateral approach for treatment of posterior malleolus fracture of the ankle. J Foot Ankle Surg 50(5):607–11. https://doi.org/10.1053/j.jfas.2011.04.022
Drijfhout van Hooff CC, Verhage SM, Hoogendoorn JM (2015) Influence of fragment size and postoperative joint congruency on long-term outcome of posterior malleolar fractures. Foot Ankle Int 36(6):673–8. https://doi.org/10.1177/1071100715570895
Verhage SM, Krijnen P, Schipper IB, Hoogendoorn JM (2019) Persistent postoperative step-off of the posterior malleolus leads to higher incidence of post-traumatic osteoarthritis in trimalleolar fractures. Arch Orthop Trauma Surg 139(3):323–329. https://doi.org/10.1007/s00402-018-3056-0
Miller AN, Carroll EA, Parker RJ, Boraiah S, Helfet DL, Lorich DG (2009) Direct visualization for syndesmotic stabilization of ankle fractures. Foot Ankle Int 30(5):419–26. https://doi.org/10.3113/FAI.2009.0419
Miller AN, Carroll EA, Parker RJ, Helfet DL, Lorich DG (2010) Posterior malleolar stabilization of syndesmotic injuries is equivalent to screw fixation. Clin Orthop Relat Res 468(4):1129–35. https://doi.org/10.1007/s11999-009-1111-4
Sultan F, Zheng X, Pan Z, Zheng Q, Li H, Wang J (2020) Characteristics of intercalary fragment in posterior malleolus fractures. Foot Ankle Surg 26(3):289–294. https://doi.org/10.1016/j.fas.2019.03.011
Karaca S, Enercan M, Ozdemir G, Kahraman S, Cobanoglu M, Kucukkaya M (2016) Importance of fixation of posterior malleolus fracture in trimalleolar fractures: a retrospective study. Ulus Travma Acil Cerrahi Derg 22(6):553–558. https://doi.org/10.5505/tjtes.2016.44844
Heim D, Niederhauser K, Simbrey N (2010) The Volkmann dogma: a retrospective, long-term, single-center study. Eur J Trauma Emerg Surg 36(6):515–9. https://doi.org/10.1007/s00068-010-0061-6
Schoenmakers S, Houben M, van Hoeve S, Willems P, Meijer K, Poeze M (2022) The influence of size and comminution of the posterior malleolus fragment on gait in trimalleolar ankle fractures. Clin Biomech (Bristol, Avon) 91:105550. https://doi.org/10.1016/j.clinbiomech.2021.105550
Quan Y, Lu H, Xu H, Liu Y, Xie W, Zhang B, Zhang D, Jiang B (2021) The distribution of posterior malleolus fracture lines. Foot Ankle Int 42(7):959–966. https://doi.org/10.1177/1071100721996700
Kumar A, Mishra P, Tandon A, Arora R, Chadha M (2018) Effect of CT on management plan in malleolar ankle fractures. Foot Ankle Int 39(1):59–66. https://doi.org/10.1177/1071100717732746
Bartonicek J, Rammelt S, Tucek M, Nanka O (2015) Posterior malleolar fractures of the ankle. Eur J Trauma Emerg Surg 41(6):587–600. https://doi.org/10.1007/s00068-015-0560-6
Zhang Y, Qin X, Song L, Li X (2018) The risk of violating the posterior malleolar fracture when nailing the ipsilateral concomitant spiral distal tibial fracture. BMC Musculoskelet Disord 19(1):123. https://doi.org/10.1186/s12891-018-1994-x
Gandham S, Millward G, Molloy AP, Mason LW (2020) Posterior malleolar fractures: A CT guided incision analysis. Foot (Edinb) 43:101662. https://doi.org/10.1016/j.foot.2019.101662
Müller ME, Nazarian S, Koch P, Schatzker J (2012) The comprehensive classification of fractures of long bones. Springer Science & Business Media, Berlin
Meinberg EG, Agel J, Roberts CS, Karam MD, Kellam JF (2018) Fracture and dislocation classification compendium-2018. J Orthop Trauma 32(Suppl 1):S1–S170. https://doi.org/10.1097/BOT.0000000000001063
Heim UF (1989) Trimalleolar fractures: late results after fixation of the posterior fragment. SLACK Incorporated Thorofare, NJ. p. 1053–1059.
Switaj PJ, Weatherford B, Fuchs D, Rosenthal B, Pang E, Kadakia AR (2014) Evaluation of posterior malleolar fractures and the posterior pilon variant in operatively treated ankle fractures. Foot Ankle Int 35(9):886–95. https://doi.org/10.1177/1071100714537630
Hansen ST (2000) Functional reconstruction of the foot and ankle. Lippincott Williams & Wilkins.
Keiler A, Riechelmann F, Thoni M, Brunner A, Ulmar B (2020) Three-dimensional computed tomography reconstruction improves the reliability of tibial pilon fracture classification and preoperative surgical planning. Arch Orthop Trauma Surg 140(2):187–195. https://doi.org/10.1007/s00402-019-03259-8
Wang Y, Wang J, Luo CF (2016) Modified posteromedial approach for treatment of posterior pilon variant fracture. BMC Musculoskelet Disord 17:328. https://doi.org/10.1186/s12891-016-1182-9
Chaparro F, Ahumada X, Urbina C, Lagos L, Vargas F, Pellegrini M, Barahona M, Bastias C (2019) Posterior pilon fracture: epidemiology and surgical technique. Injury 50(12):2312–2317. https://doi.org/10.1016/j.injury.2019.10.007
Bian L, Liu P, Yuan Z, Sha Y (2020) Stereo information of skeletal data based on CT sequence medical images. J Infect Public Health 13(12):2049–2054. https://doi.org/10.1016/j.jiph.2019.06.022
Amorosa LF, Brown GD, Greisberg J (2010) A surgical approach to posterior pilon fractures. J Orthop Trauma 24(3):188–93. https://doi.org/10.1097/BOT.0b013e3181b91927
Weber M (2004) Trimalleolar fractures with impaction of the posteromedial tibial plafond: implications for talar stability. Foot Ankle Int 25(10):716–27. https://doi.org/10.1177/107110070402501005
Yi Y, Chun DI, Won SH, Park S, Lee S, Cho J (2018) Morphological characteristics of the posterior malleolar fragment according to ankle fracture patterns: a computed tomography-based study. BMC Musculoskelet Disord 19(1):51. https://doi.org/10.1186/s12891-018-1974-1
Hou Z, Zhang Q, Zhang Y, Li S, Pan J, Wu H (2009) A occult and regular combination injury: the posterior malleolar fracture associated with spiral tibial shaft fracture. J Trauma 66(5):1385–90. https://doi.org/10.1097/TA.0b013e31817fdf0a
Hou Z, Zhang L, Zhang Q, Yao S, Pan J, Irgit K, Zhang Y (2012) The “communication line” suggests occult posterior malleolar fracture associated with a spiral tibial shaft fracture. Eur J Radiol 81(3):594–7. https://doi.org/10.1016/j.ejrad.2011.01.039
Sun C, Peng X, Fei Z, Li C, Zhou Q, Xu W, Dong Q (2021) The CT morphological characteristics and the clinical management strategy of posterior malleolar fractures with talar subluxation. Am J Transl Res 13(6):6478–6487
Yde J (1980) The Lauge Hansen classification of malleolar fractures. Acta Orthop Scand 51(1):181–92. https://doi.org/10.3109/17453678008990784
Broos PL, Bisschop AP (1992) A new and easy classification system for ankle fractures. Int Surg 77(4):309–12
Papachristou G, Efstathopoulos N, Levidiotis C, Chronopoulos E (2003) Early weight bearing after posterior malleolar fractures: an experimental and prospective clinical study. J Foot Ankle Surg 42(2):99–104. https://doi.org/10.1016/s1067-2516(03)70009-x
Farsetti P, Caterini R, Potenza V, De Luna V, De Maio F, Ippolito E (2009) Immediate continuous passive motion after internal fixation of an ankle fracture. J Orthop Traumatol 10(2):63–9. https://doi.org/10.1007/s10195-009-0048-4
Forberger J, Sabandal PV, Dietrich M, Gralla J, Lattmann T, Platz A (2009) Posterolateral approach to the displaced posterior malleolus: functional outcome and local morbidity. Foot Ankle Int 30(4):309–14. https://doi.org/10.3113/FAI.2009.0309
Hong-Chuan W, Shi-Lian K, Heng-Sheng S, Gui-Gen P, Ya-Fei Z (2010) Immediate internal fixation of open ankle fractures. Foot Ankle Int 31(11):959–64. https://doi.org/10.3113/FAI.2010.0959
Purnell GJ, Glass ER, Altman DT, Sciulli RL, Muffly MT, Altman GT (2011) Results of a computed tomography protocol evaluating distal third tibial shaft fractures to assess noncontiguous malleolar fractures. J Trauma 71(1):163–8. https://doi.org/10.1097/TA.0b013e3181edb88f
Di Giorgio L, Touloupakis G, Theodorakis E, Sodano L (2013) A two-choice strategy through a medial tibial approach for the treatment of pilon fractures with posterior or anterior fragmentation. Chin J Traumatol 16(5):272–6
Hoelsbrekken SE, Kaul-Jensen K, Morch T, Vika H, Clementsen T, Paulsrud O, Petursson G, Stiris M, Stromsoe K (2013) Nonoperative treatment of the medial malleolus in bimalleolar and trimalleolar ankle fractures: a randomized controlled trial. J Orthop Trauma 27(11):633–7. https://doi.org/10.1097/BOT.0b013e31828e1bb7
Erdem MN, Erken HY, Burc H, Saka G, Korkmaz MF, Aydogan M (2014) Comparison of lag screw versus buttress plate fixation of posterior malleolar fractures. Foot Ankle Int 35(10):1022–30. https://doi.org/10.1177/1071100714540893
Hong CC, Nashi N, Prosad Roy S, Tan KJ (2014) Impact of trimalleolar ankle fractures: how do patients fare post-operatively? Foot Ankle Surg 20(1):48–51. https://doi.org/10.1016/j.fas.2013.10.001
Kim MB, Lee YH, Kim JH, Lee JE, Baek GH (2015) Lateral transmalleolar approach and miniscrews fixation for displaced posterolateral fragments of posterior malleolus fractures in adults: a consecutive study. J Orthop Trauma 29(2):105–9. https://doi.org/10.1097/BOT.0000000000000155
Verhage SM, Schipper IB, Hoogendoorn JM (2015) Long-term functional and radiographic outcomes in 243 operated ankle fractures. J Foot Ankle Res 8:45. https://doi.org/10.1186/s13047-015-0098-1
Choi JY, Kim JH, Ko HT, Suh JS (2015) Single oblique posterolateral approach for open reduction and internal fixation of posterior malleolar fractures with an associated lateral malleolar fracture. J Foot Ankle Surg 54(4):559–64. https://doi.org/10.1053/j.jfas.2014.09.043
Endo J, Yamaguchi S, Saito M, Morikawa T, Akagi R, Sasho T (2016) Changes in the syndesmotic reduction after syndesmotic screw fixation for ankle malleolar fractures: one-year longitudinal evaluations using computer tomography. Injury 47(10):2360–2365. https://doi.org/10.1016/j.injury.2016.07.031
Chan KB, Lui TH (2016) Role of ankle arthroscopy in management of acute ankle fracture. Arthroscopy 32(11):2373–2380. https://doi.org/10.1016/j.arthro.2016.08.016
Naumann MG, Sigurdsen U, Utvag SE, Stavem K (2017) Associations of timing of surgery with postoperative length of stay, complications, and functional outcomes 3–6 years after operative fixation of closed ankle fractures. Injury 48(7):1662–1669. https://doi.org/10.1016/j.injury.2017.03.039
Vidovic D, Elabjer E, Muskardin IVA, Milosevic M, Bekic M, Bakota B (2017) Posterior fragment in ankle fractures: anteroposterior vs posteroanterior fixation. Injury 48(Suppl 5):S65–S69. https://doi.org/10.1016/S0020-1383(17)30743-X
Shi HF, Xiong J, Chen YX, Wang JF, Qiu XS, Huang J, Gui XY, Wen SY, Wang YH (2017) Comparison of the direct and indirect reduction techniques during the surgical management of posterior malleolar fractures. BMC Musculoskelet Disord 18(1):109. https://doi.org/10.1186/s12891-017-1475-7
Zhong S, Shen L, Zhao JG, Chen J, Xie JF, Shi Q, Wu YH, Zeng XT (2017) Comparison of posteromedial versus posterolateral approach for posterior malleolus fixation in trimalleolar ankle fractures. Orthop Surg 9(1):69–76. https://doi.org/10.1111/os.12308
Zhou Q, Lu H, Wang Z, Yu S, Zhang H (2017) Posterolateral approach with buttress plates and cannulated screw fixation for large posterior malleolus fractures. J Foot Ankle Surg 56(6):1173–1179. https://doi.org/10.1053/j.jfas.2017.05.028
Wang X, Zhang C, Yin JW, Wang C, Huang JZ, Ma X, Wang CW, Wang X (2017) Treatment of medial malleolus or pure deltoid ligament injury in patients with supination-external rotation Type IV ankle fractures. Orthop Surg 9(1):42–48. https://doi.org/10.1111/os.12318
Xing W, Wang Y, Sun L, Wang L, Kong Z, Zhang C, Zhang Z (2018) Ankle joint dislocation treating dislocated trimalleolar fractures accompanied with the complex posterior malleolus fracture without separation of the tibiofibular syndesmosis. Medicine (Baltimore) 97(37):e12079. https://doi.org/10.1097/MD.0000000000012079
Baek JH, Kim TY, Kwon YB, Jeong BO (2018) Radiographic change of the distal tibiofibular joint following removal of transfixing screw fixation. Foot Ankle Int 39(3):318–325. https://doi.org/10.1177/1071100717745526
Levack AE, Warner SJ, Gausden EB, Helfet DL, Lorich DG (2018) Comparing functional outcomes after injury-specific fixation of posterior malleolar fractures and equivalent ligamentous injuries in rotational ankle fractures. J Orthop Trauma 32(4):e123–e128. https://doi.org/10.1097/BOT.0000000000001104
Kim YJ, Lee JH (2018) Posterior inferior tibiofibular ligament release to achieve anatomic reduction of posterior malleolar fractures. J Foot Ankle Surg 57(1):86–90. https://doi.org/10.1053/j.jfas.2017.08.012
Miller MA, McDonald TC, Graves ML, Spitler CA, Russell GV, Jones LC, Replogle W, Wise JA, Hydrick J, Bergin PF (2018) Stability of the syndesmosis after posterior malleolar fracture fixation. Foot Ankle Int 39(1):99–104. https://doi.org/10.1177/1071100717735839
Huang Z, Liu Y, Xie W, Li X, Qin X, Hu J (2018) Pre-operative radiographic findings predicting concomitant posterior malleolar fractures in tibial shaft fractures: a comparative retrospective study. BMC Musculoskelet Disord 19(1):86. https://doi.org/10.1186/s12891-018-1982-1
Xing W, Xie P, Wang L, Liu C, Cui J, Zhang Z, Sun L (2018) The application of intraoperative ankle dislocation approach in the treatment of the unstable trimalleolar fractures involving posterior ankle comminuted fracture: a retrospective cohort study. BMC Surg 18(1):23. https://doi.org/10.1186/s12893-018-0356-9
Bartonicek J, Rammelt S, Kasper S, Malik J, Tucek M (2019) Pathoanatomy of Maisonneuve fracture based on radiologic and CT examination. Arch Orthop Trauma Surg 139(4):497–506. https://doi.org/10.1007/s00402-018-3099-2
Hendrickx LAM, Cain ME, Sierevelt IN, Jadav B, Kerkhoffs G, Jaarsma RL, Doornberg JN (2019) Incidence, predictors, and fracture mapping of (occult) posterior malleolar fractures associated with tibial shaft fractures. J Orthop Trauma 33(12):e452–e458. https://doi.org/10.1097/BOT.0000000000001605
Kellam PJ, Haller JM, Rothberg DL, Higgins TF, Marchand LS (2019) Posterior malleolar fracture morphology in tibial shaft versus rotational ankle fractures: the significance of the computed tomography scan. J Orthop Trauma 33(12):e459–e465. https://doi.org/10.1097/BOT.0000000000001601
Meijer DT, de Muinck Keizer RO, Stufkens SAS, Schepers T, Sierevelt IN, Kerkhoffs G, Goslings JC, Doornberg JN (2019) Quantification of postoperative posterior malleolar fragment reduction using 3-dimensional computed tomography (Q3DCT) determines outcome in a prospective pilot study of patients with rotational type ankle fractures. J Orthop Trauma 33(8):404–410. https://doi.org/10.1097/BOT.0000000000001486
Meijer DT, Gevers Deynoot BDJ, Stufkens SA, Sierevelt IN, Goslings JC, Kerkhoffs G, Doornberg JN (2019) What factors are associated with outcomes scores after surgical treatment of ankle fractures with a posterior malleolar fragment? Clin Orthop Relat Res 477(4):863–869. https://doi.org/10.1097/CORR.0000000000000623
Testa G, Ganci M, Amico M, Papotto G, Giardina SMC, Sessa G, Pavone V (2019) Negative prognostic factors in surgical treatment for trimalleolar fractures. Eur J Orthop Surg Traumatol 29(6):1325–1330. https://doi.org/10.1007/s00590-019-02430-6
Lee SH, Cho HG, Yang JH (2021) Predisposing factors for chronic syndesmotic instability following syndesmotic fixation in ankle fracture: minimum 5-year follow-up outcomes. Foot Ankle Surg 27(7):777–783. https://doi.org/10.1016/j.fas.2020.10.001
Zhang K, Jia X, Qiang M, Chen S, Wang S, Wang D, Chen Y (2020) Quantitative evaluation of articular involvement of posterior malleolus associated with operative indication: a comparative study of six methods based on radiography and CT. Biomed Res Int 2020:6745626. https://doi.org/10.1155/2020/6745626
Yang Y, He W, Zhou H, Xia J, Li B, Yu T (2020) Combined posteromedial and posterolateral approaches for 2-part posterior malleolar fracture fixation. Foot Ankle Int 41(10):1234–1239. https://doi.org/10.1177/1071100720937637
Wang Z, Yuan C, Zhu G, Geng X, Zhang C, Huang J, Ma X, Wang X (2020) A retrospective study on the morphology of posterior malleolar fractures based on a CT scan: whether we ignore the importance of fracture height. Biomed Res Int 2020:2903537. https://doi.org/10.1155/2020/2903537
Wang Z, Sun J, Yan J, Gao P, Zhang H, Yang Y, Jin Q (2020) Comparison of the efficacy of posterior-anterior screws, anterior-posterior screws and a posterior-anterior plate in the fixation of posterior malleolar fractures with a fragment size of >/= 15 and < 15. BMC Musculoskelet Disord 21(1):570. https://doi.org/10.1186/s12891-020-03594-7
Lee SW, Lee KJ, Park CH, Kwon HJ, Kim BS (2020) The valid diagnostic parameters in bilateral CT scan to predict unstable syndesmotic injury with ankle fracture. Diagnostics (Basel). https://doi.org/10.3390/diagnostics10100812
He JQ, Ma XL, Xin JY, Cao HB, Li N, Sun ZH, Wang GX, Fu X, Zhao B, Hu FK (2020) Pathoanatomy and injury mechanism of typical maisonneuve fracture. Orthop Surg 12(6):1644–1651. https://doi.org/10.1111/os.12733
Liu Z, Tang G, Guo S, Cai B, Li Q (2020) Therapeutic effects of internal fixation with support plates and cannulated screws via the posterolateral approach on supination external rotation stage IV ankle fracture. Pak J Med Sci 36(3):438–444. https://doi.org/10.12669/pjms.36.3.1671
Martin KD, Tripp CT, Huh J (2021) Outcomes of posterior arthroscopic reduction and internal fixation (PARIF) for the posterior malleolar fragment in trimalleolar ankle fractures. Foot Ankle Int 42(2):157–165. https://doi.org/10.1177/1071100720955149
Yu T, Ying J, Liu J, Huang D, Yan H, Xiao B, Zhuang Y (2021) Percutaneous posteroanterior screw fixation for Haraguchi type 1 posterior malleolar fracture in tri-malleolar fracture: operative technique and randomized clinical results. J Orthop Surg (Hong Kong) 29(1):2309499021997996. https://doi.org/10.1177/2309499021997996
Ceccarini P, Rinonapoli G, Antinolfi P, Caraffa A (2021) Effectiveness of ankle arthroscopic debridement in acute, subacute ankle- bimalleolar, and trimalleolar fractures. Int Orthop 45(3):721–729. https://doi.org/10.1007/s00264-020-04882-6
Black AT, Stowers JM, Tenley J, Hu CY, Eshetu T, Spielfogel WD, Katchis SD, RahnamaVaghef A, Weiner LS (2021) The association between lateral radiographs and axial computed tomography of posterior malleolar fractures as a tool for predicting medial malleolar extension: a multi-center retrospective analysis. J Foot Ankle Surg 60(5):897–901. https://doi.org/10.1053/j.jfas.2021.03.002
Fidan F, Polat A, Cetin MU, Kazdal C, Yavuz U, Lapcin O, Ozkaya U (2021) Fixation of posterior malleolar fractures with posterior plating through a posterolateral approach. J Am Podiatr Med Assoc. https://doi.org/10.7547/20-100
Erinc S, Cam N (2021) Does it matter the fixation method of the posterior malleolar fragment in trimalleolar fractures? Acta Chir Orthop Traumatol Cech 88(3):204–210 (Zalezi na metode fixace zadniho maleolarniho fragmentu u trimaleolarni zlomeniny?)
Seo J, Yang KH, Shim DW, Cho H, Park YC (2022) Marginal impaction associated with posterior malleolar fracture in rotational ankle injury. Injury 53(2):756–761. https://doi.org/10.1016/j.injury.2021.12.013
Patton BK, Orfield NJ, Clements JR (2022) Does the lauge-hansen injury mechanism predict posterior malleolar fracture morphology? J Foot Ankle Surg. https://doi.org/10.1053/j.jfas.2022.02.013
Sun C, Fei Z, Peng X, Li C, Zhou Q, Dong Q, Xu W (2022) Posterior locking plate fixation of bartonicek type IV posterior malleolar fracture: a focus on die-punch fragment size. J Foot Ankle Surg 61(1):109–116. https://doi.org/10.1053/j.jfas.2020.08.036
Funding
Open Access funding enabled and organized by Projekt DEAL. No funding was received for conducting this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that they have no conflict of interest.
Ethical approval
The study was approved by the local ethics committee of the medical board in Hamburg, Germany (WF-093/21).
Informed consent
This study did not involve human participants.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Terstegen, J., Weel, H., Frosch, KH. et al. Classifications of posterior malleolar fractures: a systematic literature review. Arch Orthop Trauma Surg 143, 4181–4220 (2023). https://doi.org/10.1007/s00402-022-04643-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-022-04643-7