
Abstract
Purpose
Dietary supplement use is common in Northern Europe. Many dietary supplements contain 100% of nutrient reference values (NRV) of micronutrients. This study investigates the contribution of dietary supplements to micronutrient intake, the prevalence of excess intake of micronutrients, and parental characteristics of dietary supplement use in Danish children.
Methods
Data on 499 4–10-year-old children from the Danish National Survey of Diet and Physical Activity 2011–2013 were analysed using non-parametric statistics to compare micronutrient intake from the diet and dietary supplements to the reference intake (RI), and to the tolerable Upper Intake Level (UL) for users and non-users of dietary supplements. Furthermore, characteristics of the parents of users and non-users of dietary supplements were examined by logistic regression analysis.
Results
Sixty-four percent of the children were dietary supplement users. Multivitamin-mineral supplements were the most frequently used type of supplement (60%). Children of never-smokers were more likely to use supplements than children of smokers. Users had significantly higher total intakes of 15 micronutrients compared to non-users. Intakes of vitamin A, zinc, and iodine from the diet alone exceeded ULs in 12–30% of the children. Use of dietary supplements gave rise to 21–73% of children in exceedance of the aforementioned three ULs as well as the UL for iron (6–45%).
Conclusion
Dietary supplement use was common among 4–10-year-old Danish children and resulted in a considerable proportion of users exceeding the ULs for vitamin A, zinc, iodine, and iron. The long-term health consequences of exceeding these ULs for children are unknown.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Use of dietary supplements is widespread in Europe, especially in the Nordic countries, and multivitamin/mineral supplements (MVMSs) are the most commonly used type of supplement in most European countries [1,2,3,4,5,6,7]. Parents typically choose to administer MVMSs to their children to prevent and treat ill health and deficiencies [8,9,10,11]. This is contrary to the fact that health authorities do not recommend use of MVMSs in healthy children. In Denmark, health authorities recommend only vitamin D supplementation year-round for children under 4 years, iron for children born prematurely, and calcium for children allergic to dairy [12].
In Europe, the content of vitamins and minerals in dietary supplements must be declared as a percentage of the nutrient reference value (NRV). NRVs are common across all European countries and represent the average requirement for vitamins and minerals for children and adults. However, the average requirement encompasses large variation, since requirements differ based on gender, age group, and other factors [1]. Supplement manufacturers use the European NRVs as a reference, and the majority of multivitamin/mineral supplements registered in Denmark contain 100% or more of the NRVs for most micronutrients [13, 14]. Thus, by taking a daily multivitamin/mineral product on top of an adequate diet, there may be a risk of Danes exceeding their requirements for vitamins and minerals. Children are especially at risk of consuming micronutrients at levels above the upper intake levels (ULs), since the margins between recommended levels of daily intake and ULs are smaller for children than for adults. However, little is known about how the common European NRVs fit with dietary habits in individual European countries such as Denmark, and how dietary supplements affect the total micronutrient intake of children specifically. Whilst data on dietary supplement use by Danish adults and adolescents has been published [3, 13, 15], there is a paucity of data on dietary supplement use by Danish children. The aim of the present study was to examine the use of dietary supplements in a nationwide sample of Danish children aged 4–10 years and assess the risk of excessive micronutrient intakes, as well as to determine the predictors of dietary supplement use.
Methods
Participants
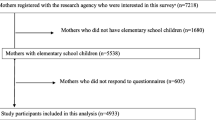
A random sample was drawn from the Danish Civil Registration System [16] in order to obtain a representative sample of the Danish population. The present study comprises 499 children aged 4–10 years. The response rate was 54% and 67% for the entire survey population (age 4–75 years) and for 4–14-year-olds, respectively [17]. The response rate was not calculated for the age range 4–10 years. The study population was divided into two age groups: 4–6-year-olds and 7–10-year-olds. As children aged ≥ 11 years are recommended the same dose of vitamins as adults, this study only includes children aged 4–10 years. Verbal consent was obtained from the parents of the children.
Data collection
Data are derived from the Danish National Survey of Diet and Physical Activity (DANSDA) 2011–13, which is a nationwide cross-sectional survey. The methods of the survey are described in more details elsewhere [17]. Briefly, information was collected on the parents’ socio-economic status and health beliefs and on the child’s lifestyle, and anthropometric measurements were taken on the children during a face-to-face interview. Data were collected from April 2011 to August 2013. Dietary data were collected by means of a validated 7-day pre-coded dietary record using household measures and series of photographs to estimate portion sizes [18, 19]. Intakes of nutrients from the diet (including iodine from mandatory fortification of salt) were calculated using the software system General Intake Estimation (GIES) version 1.000.i6 and the Danish Food Composition Database version 7.0 (www.foodcomp.dk). The Danish Food Composition database is hosted at the National Food Institute, Technical University of Denmark and updated regularly. Samples of food and drinks are collected throughout the year to account for seasonal variation in the content of nutrients. The products analysed are selected based on retail GfK ConsumerScan’s household purchasing data. Average daily intakes of foods and nutrients were estimated for each participant. Participants were included in the data analysis if they had recorded their diet for at least four days.
As part of the face-to-face interview, information on use of dietary supplements in the past year was collected, including use of MVMS, vitamin C, fish oil/cod liver oil, iron, calcium with or without vitamin D, vitamin D and ‘other types’ of dietary supplements. The question about ‘other types’ was open-ended. MVMS were defined as products containing three or more vitamins with or without minerals and other active ingredients (e.g. fish oil, probiotics or herbs) [20,21,22]. Exceptions were protein supplements containing vitamins and/or minerals and products containing B vitamins only. In approximately 90% of interviews, the mother of the participating child was interviewed. Brand names as well as consumption frequency were recorded for the different supplements used. However, for multivitamin/mineral products no brand names were collected since the products in this category were similar. Information was collected on the daily and month-to-month frequencies of supplement intake, as well as on the dose. Nutrient composition of the supplements reported in the present study were obtained from the Danish Veterinary and Food Administration’s database of registered dietary supplements [23]. Product information not included in the database was obtained from direct communication with supplement manufacturers, supplement labels or Internet websites. For products reported by participants with insufficient detail to match a known product, generic nutrient profiles were assigned, e.g. a generic vitamin D supplement for vitamin D products reported without the brand name. These generic nutrient profiles were created using a weighted average according to frequency of use of each product reported for every supplement type. Additionally, a generic MVMS were created based on GfK ConsumerScan’s household purchasing data for MVMSs. The GfK ConsumerScan household panel was comprised of about 3,000 representative Danish households, and data reflect real purchasing behaviour of individual households over extended periods [3]. GfK data from 2011 to 2013 was used.
Participants were classified as supplement users if they reported taking at least one dietary supplement within the last year, irrespective of the frequency of use and whether the product contained vitamins, minerals, or both. For assessment of individual micronutrients, participants were classified as users if they consumed a supplement containing the given micronutrient. Those who did not consume the particular nutrient in supplemental form were classified as non-users of that nutrient, even if they consumed a supplement containing other nutrients. In this paper,’dietary intake’ refers to micronutrients obtained from foods and drinks and ‘total intake’ refers to the sum of micronutrients from food, drinks, and dietary supplements.
Tolerable Upper Intake Level (UL) values established by the Scientific Committee on Food (SCF) and EFSA (European Food Safety Authority) were used to assess the proportion of children at potential risk of excessive nutrient intakes [24]. Where no UL values were listed by SCF, guidance levels (GLs) or temporary guidance levels (TGLs) were applied as suggested by a British [25] and a Danish expert group, respectively [26]. The proportion of participants whose intake of individual micronutrients exceeded the UL and whose intake exceeded the UL by 150% were calculated.
Statistical analyses
All statistical analyses were performed in SPSS (version 25, IBM SPSS Statistics). Continuous variables were not normally distributed and therefore groups were compared using the Mann–Whitney U test. The relationship between categorical variables and supplement use was explored by a Chi-squared test. When the expected number was less than five in a group, the Fisher’s exact 2-sided P-value is reported. When the independent variable included two categories, the continuity correction P-value is reported. In cases with more than two categories, the Pearson P-value is reported. Proportions are expressed as percentages and the corresponding 95% confidence intervals (CIs) were calculated using the Clopper-Pearson method.
Associations between dietary supplement use (user/non-user) and education (highest in household), smoking status, self-perceived dietary habits, intention to eat healthily, self-perceived health, age, sex, BMI, physical activity, fruit and vegetable intake and fish intake were examined by binary logistic regression analysis. A stepwise backward logistic regression approach was used, and all explanatory variables were included as categorical variables. Only variables significantly associated with supplement use were included in the final model. The results are presented as odds ratios (ORs) and 95% CIs. Collinearity diagnostics showed no indications of dependence between the factors included. A P-value less than 0.05 was considered significant.
Data on education, smoking status, self-perceived dietary habits and health, intention to eat healthily pertained to the parent of the participating child. The parent was asked if his/her dietary habits were sufficiently healthy and could answer: ‘not at all’, ‘partly’, ‘to some extent’ or ‘very much’. Intention to eat healthily was measured as ‘never’, ‘sometimes, ‘often’, or ‘very often’. Some categories of BMI, education, smoking status, and self-perceived health were merged prior to statistical analyses due to low number of participants in some categories. The highest educational attainment in the household was divided into two categories: ‘basic school/vocational education’ and ‘higher education’. As for parental smoking status, the ‘smoker’ category included those who smoked every day and those who smoked occasionally. The two other categories were ‘never-smokers’ and ‘former smokers’. After merging the categories ‘not so good’ and ‘poor’ self-perceived health answers were divided into four categories: ‘excellent’, ‘very good’, ‘good’ and ‘not so good or poor’. Continuous variables for physical activity, BMI, fruit and vegetable intake and fish intake’ were converted into categorical variables. Physical activity (pedometer-determined steps per day) had four categories: < 5000, 5000–9999, 10.000–14.999 and ≥ 15,000 steps/day. Fruit and vegetable intake was divided into three categories: < 200, 200–399.9, and ≥ 400 g/10 MJ/day. Fish intake was split into four categories: < 50, 50–199.9, 200–349.9 and ≥ 350 g/10 MJ/week. BMI had two categories ‘underweight/normal weight’ and ‘overweight/obesity’. The International Obesity Task Force age-specific and gender-specific BMI cut-off points for normal weight, overweight, and obesity were used [27, 28].
To assess dietary quality, the diet of each participant was given a diet quality score (Danish Diet Quality Index). This was based on how well their diet complied with five of the official Danish dietary guidelines for fruit and vegetables, fish, whole grain, saturated fatty acids, and added sugars. The calculation method of this score is published in detail elsewhere [29].
The ratio between energy intake and basic metabolic rate was used to classify the participants as under-reporters (EI/BMR < 1.121), plausible reporters (2.892 > EI/BMR ≥ 1.121), and over-reporters (EI/BMR ≥ 2.892) of energy intake. BMR was estimated using the gender and age-specific Schofield equations [30].
Results
Characteristics of the study population
Sixty-four percent of the 499 children were users of dietary supplements (Table 1). There was no difference in the proportion of supplement users between boys and girls, the two age groups, educational attainment, self-rated health, dietary quality score or median BMI of the child or parent. There was a significantly smaller proportion of smokers and a higher proportion of never-smokers among the supplement users (P = 0.003). The results of the logistic regression analysis confirmed this, as smoking status was the only significant independent variable associated with dietary supplement use (Table 2). Parental education (highest in household), intention to eat healthily (parent), self-perceived dietary habits (parent), sex, BMI, physical activity (pedometer-determined steps per day), fruit and vegetable intake and fish intake showed no association with use of dietary supplements (data not shown).
Types and number of dietary supplements
MVMSs were by far the most common type of supplement with 60% of users reporting taking a MVMS, and fish oil was the second most popular type of supplement (Table 3). Seventeen percent reported taking other types of supplements, including single vitamin and mineral supplements, fish oil, yeast-based supplements, dietary fibre supplements, probiotics, protein supplements and herbal/botanical products. Fifty percent consumed one dietary supplement and 12% consumed two dietary supplements (Table 4). Only a small proportion of the children consumed three or four dietary supplements (≤ 2%). There were no significant differences in use of the different types of supplements or the number of dietary supplements taken between the two age groups or between boys and girls.
Micronutrient intakes and proportions of study population in exceedance of ULs
There were no significant differences in dietary intakes of 17 selected micronutrients among users and non-users (Table 5). However, dietary supplement users had significantly higher median total intakes of 15 of these 17 micronutrients compared with non-users. Total calcium and total magnesium intakes were not significantly different between dietary supplement users and non-users, although for calcium it was borderline significant (P = 0.057, n = 499).
In both age groups, dietary intakes of vitamin A (retinol), zinc and iodine exceeded ULs in 11.5–30.1% of the children (Tables 6 and 7). When considering the total retinol intake in 4–6-year-old users, 43.1% exceeded the UL for retinol and 16.9% exceeded the UL by 150%. The latter proportion was significantly different from the proportion of non-users exceeding the UL by 150% (4.1%, P = 0.015). Furthermore, supplement use resulted in 45.4% of children exceeding the TGL for iron (total intake in users vs non-users, P < 0.001). For 73% of 4–6-year-old users, total zinc intake exceeded the UL and for 10.8% it exceeded the UL by ≥ 150%, which is significantly different from non-users (0%, P = 0.009).
In 7–10-year-olds, 12–15% of supplement users and non-users had dietary intakes in exceedance of the ULs for retinol and zinc. However, the proportion of non-users exceeding the UL for iodine was significantly higher (26.4%, P = 0.025) than the proportion of users exceeding the UL for iodine through diet alone (15.2%). As for total iodine intake in users, the proportion exceeding UL was similar to that in non-users. Supplement use meant that a significantly higher proportion of users (6.4%, P = 0.003, Fisher’s exact test) exceeded the UL for iron compared with non-users (0%).
Misreporting of energy
In the study population (n = 484), 96.5% were classified as plausible reporters of energy, 2.5% as under-reporters and 1.0% as over-reporters. There was no significant difference in the proportion of misreporters of energy between users and non-users of dietary supplements (P = 0.589).
Discussion
In this study, the use of dietary supplements and the intake of 17 selected micronutrients were investigated in Danish children aged 4–10 years. The aim was to assess whether dietary supplement use leads to micronutrient intakes that exceed the respective ULs. Nearly two-thirds of children in the study had used a dietary supplement in the past year. This is similar to the proportion of Danish adults using dietary supplements (60%) [3, 15], but is a higher proportion compared to children in other European countries [1, 6,7,8, 31] and in many other developed countries (1.1–45.5%) [32,33,34,35,36,37,38]. However, differences in data collection methodology (e.g. duration of reference periods and types of dietary supplements recorded) makes it difficult to compare use of dietary supplements between countries. The reference period of 12 months in the present study and use of any type of dietary supplement (including herbal supplements, fish oil, yeast extracts, probiotics, etc.) may explain the relatively high percentage of supplement users in the present study.
MVMSs were the most popular type of dietary supplement in Danish children, similar to statistics in other Western countries [8, 11, 31, 32, 37]. The widespread use of dietary supplements in Danish children led to a considerable proportion of supplement users exceeding the ULs for retinol, zinc, iodine and TGL for iron. The Danish diet is rich in vitamin A, zinc, and iodine, and for a considerable proportion of the participants (11.5–30.1%), the diet alone provided retinol, zinc, iodine at levels that exceeded the ULs for these three micronutrients. The high iodine intake is mainly due to a high intake of milk which provides nearly half of the iodine in the diet of children. Furthermore, cereals and table salt are other significant sources of iodine (each about 15%). Main contributors of zinc are cereals, meat, and milk providing 73% of the total intake. The high retinol intake is mainly due to liver pâté and liver. About two thirds of vitamin A in the Danish diet is in the form of retinol. Adding a dietary supplement on top of a nutrient-adequate diet, led to an even greater proportion of the study population exceeding the ULs for these three micronutrients, although the proportions of users and non-users exceeding the UL were only significantly different in the case of zinc. However, in the case of retinol, the proportion exceeding the UL by 150% was significantly higher among users than non-users. Also, supplement use led to a significantly larger proportion of users exceeding the UL for iron compared with non-users.
In contrast to surveys of adults where former smokers were more likely to use dietary supplements [15, 37, 39,40,41], we found that supplement use was significantly higher in children whose parents were never-smokers, whereas the proportion of users among children of former smokers was not significantly different from that of children of smokers. This was confirmed in a logistic regression analysis where we found smoking status to be the only significant variable associated with dietary supplement use, with smokers being less likely to use dietary supplements than never-smokers. Similar associations between parental smoking status and supplement use in children have been reported in NHANES [42] and in a German survey [8]. In other surveys, use of dietary supplements in children were associated with a more prudent diet, healthier lifestyle, higher parental income and education, but also with chronic illness [8, 11, 32, 41, 43]. In adults, dietary supplement use has been linked with other healthy lifestyle choices [41, 44]. In studies on Danish adults other factors were also associated with dietary supplement use, including age, sex, self-perceived health status [15], intention to eat a healthy diet [3], health index and educational attainment [43]. However, in contrast to other studies [41, 45], we did not find significant differences in micronutrient intakes from the diet between users and non-users, nor did the diet quality score differ. The small sample size in the present study could be a reason why we did not find more factors associated with dietary supplement use or any significant differences in dietary intakes. However, this may also be due to differences in the factors associated with dietary supplement use between adults and children and in between countries. Studies show that in younger children, dietary supplement use often reflects the parents’ dietary supplement use [41, 46]. This could also explain why there was no difference in dietary supplement use between boys and girls in this survey, whereas surveys of adults showed that women are more likely to consume dietary supplements [2, 3, 15]. We observed a non-significant higher proportion of children using MVMSs in 4–6 year olds compared to 7–10 year olds which is in accordance with findings in other surveys [11, 33].
Compared to other European countries, Danish children have a high dietary iodine intake [1]. This is despite a relatively low iodine fortification level (13 µg iodine/kg salt until mid-2019) in Denmark and fortification of only table salt and salt added to bread and bakery products [47, 48]. High intakes of dairy products, bread, cereals and, to a lesser extent, marine foods may explain the high iodine content of the diet of Danish children [17, 48]. Tap water is also an important source of iodine in Denmark, although the iodine content of tap water varies with geography [47]. In the present survey, a considerable proportion of children had a dietary iodine intake that exceeded the UL. When adding the iodine from supplements on top of a high dietary intake, about a third of 4–6-year-olds and 26% of 7–10-year-olds exceeded the UL for iodine. Following reporting of the DANSDA survey results [17], the Danish Veterinary and Food Administration recommended removing iodine from MVMSs marketed for children. Several manufacturers have subsequently revised the formulation of their MVMSs products for children. The Danish Health Authority recommends parents avoid giving MVMSs containing iodine to 3–10-year-old children who drink milk [12]. However, the mandatory iodine fortification programme was revised in 2019 and the iodine content of salt changed from 13 to 20 mg/kg. Thus, many children may still be at risk of exceeding the UL for iodine, although use of MVMSs may contribute less to excess iodine intake now.
It has previously been reported that Danish children have a high zinc intake (95% percentile > UL) compared with children in other European countries [1]. In the present survey, 22% of the children aged 4–6 years and 14–15% aged 7–10 years had a dietary zinc intake that exceeded the UL for the respective age groups. With even more zinc provided by dietary supplements, 73% of 4–6-year-old users and 45% of 7–10-year-old users exceeded the UL. Similar findings have been reported children in other high-income countries [33, 49, 50]. However, exceedance of the UL for zinc does not appear to be associated with adverse effects and is therefore not considered an issue [24, 51].
Iron intake exceeded TGL among supplement users in both age groups. The higher prevalence of excess iron intake in 4–6-year-olds may be due to provision of the same vitamin/mineral supplements to 4–6 and 7–10 years-olds. However, a significant proportion of children in the present study concurrently exceeded the TGL due to the small margin between the RI and TGL. Chronic excess iron intake could be problematic as there is no biological mechanism for excreting excess iron [52] and the consequence can be iron overload. Iron overload can lead to health issues such as gastrointestinal bleeding, diarrhoea and nausea [26]. As no UL for iron has been established for children in Europe, we chose to use the TGL suggested by Rasmussen et al. [26]. We are aware that the US Institute of Medicine (IoM) has published a UL for iron of 40 mg/day for children. No children in this study exceeded the IoM UL for iron. However, as discussed by Rasmussen et al. [26] the IoM UL is based on observations of acute adverse gastrointestinal effects and the UL does not consider population groups vulnerable to iron overload. Rasmussen et al. extrapolated the provisional maximum tolerable daily intake (PMTDI) established at 0.8 mg/kg bodyweight by FAO/WHO Joint Expert Group on Food Additives in 2003 to children based on surface area [26].
We also found that a high proportion (12–30%) of children exceeded the UL for retinol. When looking at the diet alone this was especially true among 4–6-year-olds. Among supplement users, 43.1% of 4–6-year-olds exceeded the UL for retinol, whereas 20.7% of 7–10-year-olds exceeded the UL. The diet of Danish children is generally rich in vitamin A due to frequent consumption of food items such a pork liver pâté, liver, and carrots. Especially the youngest children have a vitamin A-rich diet [17]. Limiting further retinol intake from dietary supplements would help prevent toxic effects of prolonged excessive vitamin A intake. Long term hypervitaminosis A can lead to hepatotoxicity, hypercalcemia, and skin and bone changes [53]; however, data on the long-term effects of excessive retinol intake in children is scarce at present [33]. To our knowledge, no adverse effects from excessive retinol intake in Danish children have been reported. However, adverse events related to dietary supplement use are not systematically recorded in Denmark. The 5th percentile for vitamin A intake in this study population (4–10 years old children) is approx. 400 RE, which is the RI for 6–9-year-olds, and the median intake is 2.5-fold the RI. Thus, reducing the amount of vitamin A in dietary supplements is unlikely to lead to widespread vitamin A insufficiency in Danish children.
Children whose diet provided vitamin and/or mineral intakes above ULs had a higher energy intake and consumed more foods rich in iodine (dairy products, bread, cereals, salt), retinol (pork liver pâté, liver) and zinc (meat, bread, cereals, dairy products) than children whose diets did not provide excessive levels of micronutrients (data not shown). Excess micronutrient intakes obtained through the diet is less concerning due to variation in diet over time.
Children are particularly vulnerable to excess intake of micronutrients because they are growing and because of the small margin between optimal intake and excess intake [35]. The ULs for children are extrapolated from adult values on the basis of metabolic body weight [24, 54] and the margins between the Estimated Average Requirements and ULs are smaller for young children than for adults due to the use of a greater uncertainty factor in the calculation of ULs for children [54]. This could partly explain why a larger proportion of children than adults exceed ULs through the diet and why a relatively larger proportion of dietary supplement users amongst children exceed ULs [1]. Another factor contributing to excess intakes is consumption of fortified foods. As fortified foods become more common in Denmark, these foods also need to be regarded as significant sources of micronutrients.
The strength of the Danish National Survey of Diet and Physical Activity is that it is based on a random sample of the general population, it has a high response rate among children, the reference period for dietary supplement use was 12 months, and the habitual diet was recorded for 7 days. Whilst a reference period of 12 months may be a strength in that it accounts for supplements consumed episodically, it may also be susceptible to difficulties in recalling supplements used occasionally or many months ago. It may also be considered a limitation that any supplement use in the past 12 months categorizes a person as a user. This may partly explain the high proportion of users in Denmark compared to other countries. Measuring dietary intake in children is difficult and often prone to reporting error with under-reporting of energy being frequent, but some over-reporting also occurs [55, 56]. However, in this study, 96.5% were classified as plausible reporters of energy making misreporting a minor issue. The contents of micronutrients such as iodine and selenium are highly variable in some foods. However, the national food composition database in Denmark is updated regularly, the vitamin and mineral contents of many foods have been analysed and seasonal variation is taken into account when collecting samples for analyses. Missing data in databases can lead to underestimation of the intake of micronutrients, however, there are few missing values in the food composition data used in DANSDA.
Another limitation is the calculation using a generic MVMS instead of the specific MVMS taken by participants. Two studies found greater accuracy with using more specific types of MVMSs in calculations of micronutrient intakes from supplements compared to using a generic MVMS [57, 58]. Furthermore, due to the small sample size, we did not distinguish between daily, frequent and occasional users of dietary supplements, nor did we exclude mis-reporters of dietary intake from the analyses. Improvements in methodology will make the estimation of micronutrient intakes from dietary supplements more accurate in future surveys compared to the present survey.
In conclusion, MVMSs are the most commonly consumed dietary supplement. Most dietary supplements users consumed only one dietary supplement. Only smoking status of the parent was significantly associated with supplement use, with children of non-smoking parents more likely to be supplement users. There were no differences in dietary intakes of micronutrients between dietary supplement users and non-users. However, a considerable proportion of children consumed excess amounts of retinol, iodine, and zinc through their diet. With dietary supplements further increasing intake of retinol, iodine, and zinc, some children reached very high intakes of these three micronutrients. The consequences of chronic excessive intake of retinol, iodine and zinc in children is unknown. Excess zinc and iodine may be less of a problem than excess iron and retinol, which can cause longer-term health issues in the form of hepatic fibrosis [53, 59]. Supplement use also led to excess iron intake in some children, particular in the youngest children. We acknowledge that the diet of some children may provide insufficient amounts of zinc, iodine, and iron (data not shown); thus, for those consuming a suboptimal diet, a dietary supplement may be beneficial. However, median intakes of zinc and iodine were above the RIs, indicating that the prevalence of inadequate zinc and iodine intakes is low. For most Danish 4–10-year-olds, the diet seems to provide enough micronutrients with the exception of vitamin D. Thus, most Danish children do not need dietary supplements.
Data availability
In accordance with Danish law and GDPR, the data and the analytical scripts used in the present study can only be accessed through the servers at The Technical University of Denmark and requires a Disclosure Declaration. Access and a Disclosure Declaration can be granted upon request if the applicant fulfils the criteria for access. The Technical University of Denmark can be contacted by email: camp@food.dtu.dk or apbj@food.dtu.dk.
References
Flynn A, Hirvonen T, Mensink G et al (2009) Intake of selected nutrients from foods, from fortification and from supplements in various European countries. Food Nutr Res. https://doi.org/10.3402/FNR.V53I0.2038
Skeie G, Braaten T, Hjartåker A et al (2009) Use of dietary supplements in the european prospective investigation into cancer and nutrition calibration study. Eur J Clin Nutr 63:S226–S238. https://doi.org/10.1038/ejcn.2009.83
Tetens I, Biltoft-Jensen A, Spagner C et al (2011) Intake of micronutrients among Danish adult users and non-users of dietary supplements. Food Nutr Res. https://doi.org/10.3402/fnr.v55i0.7153
Sicińska E, Pietruszka B, Januszko O, Kałuża J (2019) Different socio-demographic and lifestyle factors can determine the dietary supplement use in children and adolescents in central-eastern Poland. Nutrients. https://doi.org/10.3390/nu11030658
Perlitz H, Mensink GBM, Barbosa CL et al (2019) Use of vitamin and mineral supplements among adolescents living in germany—results from eskimo ii. Nutrients 11:1208. https://doi.org/10.3390/nu11061208
Irish Universities Nutrition Alliance (IUNA) (2020) National Children’s Food Survey II. Case Med Res. https://doi.org/10.31525/ct1-nct04286932
van Rossum CTM, Buurma-Rethans EJM, Dinnissen CS, et al (2020) National Institute for Public Health and the Environment. The diet of the Dutch: Results of the Dutch National Food Consumption Survey 2012–2016
Sichert-Hellert W, Kersting M (2004) Vitamin and mineral supplements use in German children and adolescents between 1986 and 2003: Results of the DONALD study. Ann Nutr Metab 48:414–419. https://doi.org/10.1159/000083574
Elliott C (2019) Assessing vitamins, minerals and supplements marketed to children in Canada. Int J Environ Res Public Health 16:4326. https://doi.org/10.3390/ijerph16224326
Dwyer JT, Saldanha LG, Bailen RA et al (2022) Do multivitamin/mineral dietary supplements for young children fill critical nutrient gaps? J Acad Nutr Diet 122:525–532. https://doi.org/10.1016/J.JAND.2021.10.019
Dwyer J, Nahin RL, Rogers GT et al (2013) Prevalence and predictors of children’s dietary supplement use: the 2007 national health interview survey. Am J Clin Nutr 97:1331–1337. https://doi.org/10.3945/ajcn.112.052373
The Danish Veterinary and Food Administration Hvem har gavn af kosttilskud? (Who benefits from taking dietary supplements?). https://altomkost.dk/fakta/kosttilskud/hvem-har-gavn-af-kosttilskud/. Accessed 7 Mar 2022
Gille M-B, Biltoft-Jensen A, Hartkopp HB et al (2010) Brug af kosttilskud blandt unge danskere - og sammenhæng med næringsstofindtag, kostkvalitet og livsstilsfaktorer (Use of dietary supplements among Danish adolescents - and association with nutrient intake, diet quality, and lifestyle factors). Tech Univ Denmark, Natl Food Institute
Mason P (2007) One is okay, more is better? Pharmacological aspects and safe limits of nutritional supplements. Proc Nutr Soc 66:493–507. https://doi.org/10.1017/S0029665107005812
Knudsen VK, Rasmussen LB, Haraldsdóttir J et al (2002) Use of dietary supplements in Denmark is associated with health and former smoking. Public Health Nutr 5:463–468. https://doi.org/10.1079/PHN2001276
Pedersen CB (2011) The Danish civil registration system. Scand J Public Health 39:22–25. https://doi.org/10.1177/1403494810387965
Pedersen AN, Christensen T, Matthiessen J, Knudsen VK, Sørensen MR, Biltoft-Jensen AP, Hinsch HJ et al (2015) Danskernes kostvaner 2011–2013. Hovedresultater. (Dietary Habits in Denmark 2011–2013. Main results). Natl Food Institute, Tech Univ Denmark
Biltoft-Jensen A, Hjorth MF, Trolle E et al (2013) Comparison of estimated energy intake using Web-based dietary assessment software with accelerometer-determined energy expenditure in children. Food Nutr Res 57:21434. https://doi.org/10.3402/FNR.V57I0.21434
Rothausen BW, Matthiessen J, Groth MV et al (2012) Comparison of estimated energy intake from 2×24-hour recalls and a seven-day food record with objective measurements of energy expenditure in children. Food Nutr Res 56:1–10. https://doi.org/10.3402/FNR.V56I0.12221
Radimer K, Bindewald B, Hughes J et al (2004) Dietary supplement use by US adults: data from the national health and nutrition examination survey, 1999–2000. Am J Epidemiol 160:339–349
Yetley EA (2007) Multivitamin and multimineral dietary supplements: definitions, characterization, bioavailability, and drug interactions. Am J Clin Nutr 85(suppl):269S–276S
Comerford KB (2013) Recent developments in multivitamin/mineral research. Adv Nutr 4:644–656
Kosttilskudsportal. Fødevarestyrelsen (Dietary supplement database. Danish Veterinary and Food Administration). https://www.foedevarestyrelsen.dk/Foedevarer/Kosttilskud/Sider/SøgIKosttilskud.aspx. Accessed 1 Jun 2022
European Food Safety Authority (2006) Tolerable upper intake levels for vitamins and minerals. EFSA scientific committee on food and scientific panel on dietetic products, nutrition and allergies. The European Food Safety Authority. Parma, Italy
The Expert Group on Vitamins and Minerals. 2003. Safe upper levels for vitamins and minerals. https://cot.food.gov.uk/sites/default/files/vitmin2003.pdf
Rasmussen SE, Andersen NL, Dragsted LO, Larsen JC (2006) A safe strategy for addition of vitamins and minerals to foods. Eur J Nutr 45:123–135. https://doi.org/10.1007/s00394-005-0580-9
Cole TJ, Bellizzi MC, Flegal KM, Dietz WH (2000) Establishing a standard definition for child overweight and obesity worldwide: international survey. Br Med J 320:1240–1243. https://doi.org/10.1136/bmj.320.7244.1240
Cole TJ, Lobstein T (2012) Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr Obes 7:284–294. https://doi.org/10.1111/J.2047-6310.2012.00064.X
Knudsen VK, Fagt S, Trolle E et al (2012) Evaluation of dietary intake in Danish adults by means of an index based on food-based dietary guidelines. Food Nutr Res 56:17129. https://doi.org/10.3402/fnr.v56i0.17129
Schofield WN (1985) Predicting basal metabolic rate, new standards and review of previous work. Hum Nutr Clin Nutr 39(Suppl 1):5–41
Huybrechts I, Maes L, Vereecken C et al (2010) High dietary supplement intakes among Flemish preschoolers. Appetite 54:340–345. https://doi.org/10.1016/j.appet.2009.12.012
Stierman B, Mishra S, Gahche JJ et al (2020) Dietary supplement use in children and adolescents aged ≤19 years - United States, 2017–2018. MMWR Morb Mortal Wkly Rep 69:1557–1562. https://doi.org/10.15585/MMWR.MM6943A1
Bailey RL, Fulgoni VL, Keast DR et al (2012) Do dietary supplements improve micronutrient sufficiency in children and adolescents? J Pediatr 161:837-842.e3. https://doi.org/10.1016/j.jpeds.2012.05.009
Keshavarz P, Shafiee M, Islam N et al (2021) Prevalence of vitamin-mineral supplement use and associated factors among canadians: results from the 2015 canadian community health survey. Appl Physiol Nutr Metab 46:1370–1377. https://doi.org/10.1139/apnm-2021-0090
Kobayashi E, Nishijima C, Sato Y et al (2018) The prevalence of dietary supplement use among elementary, junior high, and high school students: a nationwide survey in Japan. Nutrients. https://doi.org/10.3390/NU10091176
Gong W, Liu A, Yao Y et al (2018) Nutrient supplement use among the chinese population: a cross-sectional study of the 2010–2012 China nutrition and health surveillance. Nutrients 10:1733. https://doi.org/10.3390/nu10111733
O’Brien SK, Malacova E, Sherriff JL, Black LJ (2017) The prevalence and predictors of dietary supplement use in the Australian population. Nutrients. https://doi.org/10.3390/nu9101154
Jeon JH, Seo MY, Kim SH, Park MJ (2021) Dietary supplement use in Korean children and adolescents, KNHANES 2015–2017. Public Health Nutr 24:957–964. https://doi.org/10.1017/S1368980020003419
Bailey RL, Gahche JJ, Miller PE et al (2013) Why US adults use dietary supplements. JAMA Intern Med 173:355–361. https://doi.org/10.1001/jamainternmed.2013.2299
Touvier M, Niravong M, Volatier JL et al (2009) Dietary patterns associated with vitamin/mineral supplement use and smoking among women of the E3N-EPIC cohort. Eur J Clin Nutr 63:39–47. https://doi.org/10.1038/sj.ejcn.1602907
Rock CL (2007) Multivitamin-multimineral supplements: who uses them? Am J Clin Nutr. https://doi.org/10.1093/AJCN/85.1.277S
Picciano MF, Dwyer JT, Radimer KL et al (2007) Dietary supplement use among infants, children, and adolescents in the United States, 1999–2002. Arch Pediatr Adolesc Med 161:978–985. https://doi.org/10.1001/ARCHPEDI.161.10.978
Kofoed CLF, Christensen J, Dragsted LO et al (2015) Determinants of dietary supplement use - healthy individuals use dietary supplements. Br J Nutr 113:1993–2000. https://doi.org/10.1017/S0007114515001440
Bailey RL, Fakhouri TH, Park Y et al (2015) Multivitamin-mineral use is associated with reduced risk of cardiovascular disease mortality among women in the United States. J Nutr 145:572–578. https://doi.org/10.3945/jn.114.204743
Shaikh U, Byrd RS, Auinger P (2009) Vitamin and mineral supplement use by children and adolescents in the 1999–2004 national health and nutrition examination survey: relationship with nutrition, food security, physical activity, and health care access. Arch Pediatr Adolesc Med 163:150–157. https://doi.org/10.1001/archpediatrics.2008.523
Martin CL, Murphy SP, Novotny R (2008) Contribution of dietary supplements to nutrient adequacy among children in Hawaii. J Am Diet Assoc 108:1874–1880. https://doi.org/10.1016/j.jada.2008.08.013
Rasmussen LB, Jørgensen T, Perrild H et al (2014) Mandatory iodine fortification of bread and salt increases iodine excretion in adults in Denmark - A 11-year follow-up study. Clin Nutr 33:1033–1040. https://doi.org/10.1016/j.clnu.2013.10.024
Outzen M, Lund CE, Christensen T et al (2022) Assessment of iodine fortification of salt in the Danish population. Eur J Nutr 61:2939–2951. https://doi.org/10.1007/s00394-022-02826-x
Shakur YA, Tarasuk V, Corey P, O’Connor DL (2012) A comparison of micronutrient inadequacy and risk of high micronutrient intakes among vitamin and mineral supplement users and nonusers in Canada. J Nutr 142:534–540. https://doi.org/10.3945/jn.111.149450
Butte NF, Fox MK, Briefel RR et al (2010) Nutrient intakes of US infants, toddlers, and preschoolers meet or exceed dietary reference intakes. J Am Diet Assoc 110:S27–S37. https://doi.org/10.1016/j.jada.2010.09.004
Wuehler S, de Romaña DL, Haile D et al (2022) Reconsidering the tolerable upper levels of zinc intake among infants and young children: a systematic review of the available evidence. Nutrients 14:1938
Bailey RL, Fulgoni VL, Keast DR, Dwyer JT (2011) Dietary supplement use is associated with higher intakes of minerals from food sources. Am J Clin Nutr 94:1376–1381. https://doi.org/10.3945/ajcn.111.020289
Anselmo F, Driscoll MS (2021) Deleterious side effects of nutritional supplements. Clin Dermatol 39:745–756. https://doi.org/10.1016/j.clindermatol.2021.05.002
Engle-Stone R, Vosti SA, Luo H et al (2019) Weighing the risks of high intakes of selected micronutrients compared with the risks of deficiencies. Ann N Y Acad Sci 1446:81–101. https://doi.org/10.1111/nyas.14128
Forrestal SG (2011) Energy intake misreporting among children and adolescents: a literature review. Matern Child Nutr 7:112–127
Livingstone MBE, Robson PJ, Wallace JMW (2004) Issues in dietary intake assessment of children and adolescents. Br J Nutr 92:S213–S222. https://doi.org/10.1079/bjn20041169
Park SY, Murphy SP, Wilkens LR et al (2006) Allowing for variations in multivitamin supplement composition improves nutrient intake estimates for epidemiologic studies. J Nutr 136:1359–1364. https://doi.org/10.1093/jn/136.5.1359
Murphy SP, White KK, Park SY, Sharma S (2007) Multivitamin-multimineral supplements’ effect on total nutrient intake. Am J Clin Nutr. https://doi.org/10.1093/ajcn/85.1.280S
Martini L, Pecoraro L, Salvottini C et al (2020) Appropriate and inappropriate vitamin supplementation in children. J Nutr Sci 9:e20. https://doi.org/10.1017/jns.2020.12
Nordic Council of Ministers (2014) Nordic nutrition recommendations 2012. Integrating nutrition and physical activity, 5th edn. Nord, Copenhagen
Acknowledgements
The authors would like to thank all the participants who took part in the Danish National Survey of Diet and Physical activity, data warehouse manager Karsten Kørup for assistance with data processing and Ophelia Zeng Pedersen for proofreading.
Funding
Open access funding provided by Royal Danish Library. This research received no external funding.
Author information
Authors and Affiliations
Contributions
CC analysed and interpreted the data and wrote the first draft of the paper. JM, SF and ABJ designed the study, interpreted the data, and contributed to the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
The Danish National Surveys on Diet and Physical Activity have been conducted in accordance with the guidelines laid down in the Declaration of Helsinki and have been approved by the Danish Data Protection Agency. According to Danish law, a favourable opinion from an Ethical Research Ethics Committee was not required to conduct this survey.
Consent to participate
Verbal informed consent was obtained from the parents of all children participating.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Christensen, C., Matthiessen, J., Fagt, S. et al. Dietary supplements increase the risk of excessive micronutrient intakes in Danish children. Eur J Nutr 62, 2449–2462 (2023). https://doi.org/10.1007/s00394-023-03153-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00394-023-03153-5