
Abstract
Background
Early colorectal cancer (ECC) is defined as T1NXM0 colorectal cancer (CRC). Although a non-negligible number of T1-CRCs presents metastatic lymph-nodes, local excision is increasingly proposed as alternative to radical resection. Several criteria have been suggested to identify low-risk T1-CRC, but recommendations on this topic are still heterogeneous. This study aims to identify criteria associated with N+ T1-CRC, to select patients to undergo (or not) local excision.
Methods
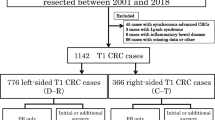
A retrospective analysis of demographic, clinical, and histology criteria of 122 consecutive T1-CRC patients undergoing radical resection at Parma University Hospital between 2000 and 2018 has been performed.
Results
Lymph-node metastasis (LNM) was observed in 15/122 patients (12.3%). No LNM was observed among well-differentiated (G1) tumors (0/37), while 10/65 (15.4%) G2 cases as well as 5/20 (25%) G3 patients presented LNM. G1 was associated with absence of LNM (p = 0.013). After excluding G1 patients, the rate of N + T1-CRC was 17.6% (15/85). LNM was observed in 4/8 (50%) patients with lymphovascular invasion (LVI) and in 11/77 (14.2%) without LVI. LVI resulted being associated with LNM (p < 0.042). LNM was reported in 28.3% of cases with a tumor infiltration >4.25 mm (13/46), compared to 5.1% in cases with an infiltration ≤4.25 mm (2/39) (p = 0.012). In Cox regression analysis, the higher hazard ratio (HR) was reported for the LVI + and infiltration >4.25 mm (HR 24.849).
Conclusions
In patients with ECC (pT1NXM0), good differentiation (G1), absence of lymphovascular invasion (LVI-), and tumor radial infiltration ≤4.25 mm may allow performing local resection and avoiding radical surgery.


Similar content being viewed by others


References
Siegel RL, Miller KD, Jemal A (2018) Cancer statistics, 2018. CA Cancer J Clin 68:7–30. https://doi.org/10.3322/caac.21442
Jemal A, Bray F, Center MM et al (2011) Global cancer statistics. CA Cancer J Clin 61:69–90. https://doi.org/10.3322/caac.20107
Compton CC, Byrd DR, Garcia-Aguilar J et al (2012) Colon and rectum (sarcomas, lymphomas, and carcinoid tumors of the large intestine are not included). https://doi.org/10.1007/978-1-4614-2080-4_14
Bianco F, Arezzo A, Agresta F et al (2015) Practice parameters for early colon cancer management: Italian Society of Colorectal Surgery (Società Italiana di Chirurgia Colo-Rettale; SICCR) guidelines. Tech Coloproctol 19:577–585. https://doi.org/10.1007/s10151-015-1361-y
Freeman HJ (2013) Early stage colon cancer. World J Gastroenterol 19:8468–8473. https://doi.org/10.3748/wjg.v19.i46.8468
Paik N, Chang J-I, Kim ER et al (2019) Su 1730 Long-term outcome and surveillance strategies of endoscopic resection for early colorectal cancer. Gatrointest Endosc 89:AB398–AB398. https://doi.org/10.1016/j.gie.2019.03.602
Labianca R, Nordlinger B, Beretta GD et al (2013) Early colon cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 24(Suppl 6):vi64–72. https://doi.org/10.1093/annonc/mdt354
The Italian ColoRectal Anastomotic Leakage (iCral) study group (2019) Colorectal surgery in Italy: a snapshot from the iCral study group. Updates Surg 71:339–347. https://doi.org/10.1007/s13304-018-00612-1
Sakuragi M, Togashi K, Konishi F et al (2003) Predictive factors for lymph node metastasis in T1 stage colorectal carcinomas. Dis Colon Rectum 46:1626–1632. https://doi.org/10.1007/bf02660767
Okabe S, Shia J, Nash G et al (2004) Lymph node metastasis in T1 adenocarcinoma of the colon and rectum. J Gastrointest Surg 8:1032–101040. https://doi.org/10.1016/j.gassur.2004.09.038
Ferlay J, Soerjomataram I, Dikshit R et al (2015) Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer 136:E359–386. https://doi.org/10.1002/ijc.29210
Council of the European Union (2003) Council Recommendation of 2 December 2003 on cancer screening (2003/878/EC). Off J Eur Union 34−38
Beaton C, Twine CP, Williams GL et al (2013) Systematic review and meta-analysis of histopathological factors influencing the risk of lymph node metastasis in early colorectal cancer. Colorectal Dis 15:788–797. https://doi.org/10.1111/codi.12129
Lezoche E, Baldarelli M, Lezoche G et al (2012) Randomized clinical trial of endoluminal locoregional resection versus laparoscopic total mesorectal excision for T2 rectal cancer after neoadjuvant therapy. Br J Surg 99:1211–1218. https://doi.org/10.1002/bjs.8821
Yamamoto S, Watanabe M, Hasegawa H et al (2004) The risk of lymph node metastasis in T1 colorectal carcinoma. Hepatogastroenterology 51:998–1000
Yun JA, Huh JW, Kim HC et al (2016) Local recurrence after curative resection for rectal carcinoma: the role of surgical resection. Medicine (Baltimore) 95:e3942. https://doi.org/10.1097/md.0000000000003942
Bikhchandani J, Ong GK, Dozois EJ et al (2015) Outcomes of salvage surgery for cure in patients with locally recurrent disease after local excision of rectal cancer. Dis Colon Rectum 58:283–287. https://doi.org/10.1097/dcr.0000000000000283
Arezzo A, Bianco F, Agresta F et al (2015) Practice parameters for early rectal cancer management: Italian Society of Colorectal Surgery (Società Italiana di Chirurgia Colo-Rettale; SICCR) guidelines. Tech Coloproctol 19:587–593. https://doi.org/10.1007/s10151-015-1362-x
Xu X, Zhang C, Ni X et al (2020) Population-based analysis on predictors for lymph node metastasis in T1 colon cancer. Surg Endosc 34:4030–4040. https://doi.org/10.1007/s00464-019-07192-0
Kaneko I, Tanaka S, Oka S et al (2007) Lymphatic vessel density at the site of deepest penetration as a predictor of lymph node metastasis in submucosal colorectal cancer. Dis Colon Rectum 50:13–21. https://doi.org/10.1007/s10350-006-0745-5
Suzuki A, Togashi K, Nokubi M et al (2009) Evaluation of venous invasion by Elastica van Gieson stain and tumor budding predicts local and distant metastases in patients with T1 stage colorectal cancer. Am J Surg Pathol 33:1601–1607. https://doi.org/10.1097/PAS.0b013e3181ae29d6
Wada H, Shiozawa M, Sugano N et al (2013) Lymphatic invasion identified with D2–40 immunostaining as a risk factor of nodal metastasis in T1 colorectal cancer. Int J Clin Oncol 18:1025–1031. https://doi.org/10.1007/s10147-012-0490-9
Ishii M, Ota M, Saito S et al (2009) Lymphatic vessel invasion detected by monoclonal antibody D2–40 as a predictor of lymph node metastasis in T1 colorectal cancer. Int J Colorectal Dis 24:1069–1074. https://doi.org/10.1007/s00384-009-0699-x
Amin MB, Edge S, Greene F, Byrd DR, Brookland RK, Washington MK, Gershenwald JE, Compton CC, Hess KR et al (Eds.) (2017) AJCC Cancer Staging Manual (8th edition). Springer International Publishing: American Joint Commission on Cancer
Ueno H, Price AB, Wilkinson KH et al (2004) A new prognostic staging system for rectal cancer. Ann Surg 240:832–839. https://doi.org/10.1097/01.sla.0000143243.81014.f2
Batsakis JG (1985) Nerves and neurotropic carcinomas. Ann Otol Rhinol Laryngol 94:426–427
Washington MK, Berlin J, Branton P et al (2009) Protocol for the examination of specimens from patients with primary carcinoma of the colon and rectum. Arch Pathol Lab Med 133:1539–1551. https://doi.org/10.5858/133.10.1539
Kikuchi R, Takano M, Takagi K et al (1995) Management of early invasive colorectal cancer. Risk of recurrence and clinical guidelines. Dis Colon Rectum 38:1286–1295. https://doi.org/10.1007/bf02049154
Costi R, Beggi F, Reggiani V et al (2014) Lymph node ratio improves TNM and Astler-Coller’s assessment of colorectal cancer prognosis: an analysis of 761 node positive cases. J Gastrointest Surg 18:1824–1836. https://doi.org/10.1007/s11605-014-2591-4
Wada H, Shiozawa M, Katayama K et al (2015) Systematic review and meta-analysis of histopathological predictive factors for lymph node metastasis in T1 colorectal cancer. J Gastroenterol 50:727–734. https://doi.org/10.1007/s00535-015-1057-0
Benson AB, Venook AP, Al-Hawary MM et al (2018) NCCN guidelines insights: colon cancer, Version 2.2018. J Natl Compr Canc Netw 16:359–369. https://doi.org/10.6004/jnccn.2018.0021
Hashiguchi Y, Muro K, Saito Y et al (2020) Japanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines 2019 for the treatment of colorectal cancer. Int J Clin Oncol 25:1–42. https://doi.org/10.1007/s10147-019-01485-z
Benson AB, Venook AP, Al-Hawary MM et al (2018) Rectal cancer, Version 2.2018, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw 16:874–901. https://doi.org/10.6004/jnccn.2018.0061
Gimon TI, Dykstra MA, Chezar K et al (2020) Malignant colorectal polyp pathology: are we getting sufficient information to make decisions? Dis Colon Rectum 63:135–142. https://doi.org/10.1097/dcr.0000000000001538
Backes Y, Elias SG, Groen JN et al (2018) Histologic factors associated with need for surgery in patients with pedunculated T1 colorectal carcinomas. Gastroenterology 154:1647–1659. https://doi.org/10.1053/j.gastro.2018.01.023
Kudo S (1993) Endoscopic mucosal resection of flat and depressed types of early colorectal cancer. Endoscopy 25:455–461. https://doi.org/10.1055/s-2007-1010367
Aytac E, Gorgun E, Costedio MM et al (2016) Impact of tumor location on lymph node metastasis in T1 colorectal cancer. Langenbecks Arch Surg 401:627–632. https://doi.org/10.1007/s00423-016-1452-x
Dai W, Mo S, Xiang W et al (2020) The critical role of tumor size in predicting prognosis for T1 colon cancer. Oncologist 25:244–251. https://doi.org/10.1634/theoncologist.2019-0469
Ichimasa K, Kudo SE, Miyachi H et al (2017) Comparative clinicopathological characteristics of colon and rectal T1 carcinoma. Oncol Lett 13:805–810. https://doi.org/10.3892/ol.2016.5464
Ozawa T, Kandimalla R, Gao F et al (2018) A microRNA signature associated with metastasis of T1 colorectal cancers to lymph nodes. Gastroenterology 154:844–848.e847. https://doi.org/10.1053/j.gastro.2017.11.275
Author information
Authors and Affiliations
Contributions
Substantial contributions to the conception or design of the work, the acquisition, analysis, and interpretation of data for the work, drafting the work and revising it critically for important intellectual content, agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved: Andrea Morini, Alfredo Annicchiarico, Renato Costi. Substantial contributions to analysis, critically revision for important intellectual content, agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved: Andrea Morini, Alfredo Annicchiarico, Federica De Giorgi, Elena Ferioli, Filippo Montali, Pellegrino Crafa, Renato Costi. Final approval of the version to be published: Andrea Morini, Alfredo Annicchiarico, Federica De Giorgi, Elena Ferioli, Andrea Romboli, Filippo Montali, Pellegrino Crafa, Renato Costi.
Corresponding author
Ethics declarations
Ethics approval
Approved by the local Ethics Commission.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The manuscript has not been a podium or poster meeting presentation.
What does this paper add to the literature?
From the analysis of this cohort of patients with T1NXM0 colorectal cancer, a simple algorithm, based on LVI, tumor grading and depth of infiltration (≤ / > 4.5 mm), allowed identifying patients with high lymph-nodal metastasis risk to be referred to colorectal resection, and others who may skip surgery.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Morini, A., Annicchiarico, A., De Giorgi, F. et al. Local excision of T1 colorectal cancer: good differentiation, absence of lymphovascular invasion, and limited tumor radial infiltration (≤4.25 mm) may allow avoiding radical surgery. Int J Colorectal Dis 37, 2525–2533 (2022). https://doi.org/10.1007/s00384-022-04279-4
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00384-022-04279-4