
Abstract
Objective
To systematically determine the accuracy of Liver Imaging Reporting and Data System treatment response (LR-TR) algorithm for diagnosing the viability of hepatocellular carcinoma (HCC) treated with locoregional therapy (LRT).
Methods
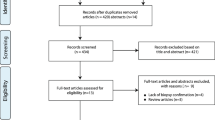
Original studies reporting the diagnostic accuracy of LR-TR algorithm on dynamic contrast-enhanced computed tomography or magnetic resonance imaging (MRI) were identified in MEDLINE and EMBASE up to June 1, 2020. The meta-analytic summary sensitivity and specificity of LR-TR algorithm were calculated using a bivariate random-effects model. Subgroup analyses and meta-regression analysis were performed to explore study heterogeneity.
Results
We found six studies reporting the accuracy of LR-TR viable category (601 observations in 453 patients). The meta-analytic pooled sensitivity and specificity of LR-TR viable category were 63% (95% confidence interval [CI], 39–81%; I2 = 88%) and 96% (95% CI, 91–99%; I2 = 76%), respectively. The meta-analytic pooled sensitivity and specificity of LR-TR viable or equivocal category combined were 71% (95% CI, 55–84%; I2 = 89%) and 87% (95% CI, 73–94% I2 = 80%), respectively. Studies which used only MRI showed a trend towards higher sensitivity (71% [95% CI, 46–88%]) with a comparable specificity (95% [95% CI, 86–99%]) of LR-TR viable category compared to the whole group. The type of reference standard and study design were significantly associated with study heterogeneity (p ≤ 0.01).
Conclusions
The LR-TR viable category had high specificity but suboptimal sensitivity for diagnosing the viability of HCC after LRT. Substantial study heterogeneity was noted, and it was significantly associated with the type of reference standard and study design.
Key Points
• The meta-analytic pooled sensitivity and specificity of LR-TR viable category were 63% (95% CI, 39–81%) and 96% (95% CI, 91–99%), respectively.
• The meta-analytic pooled sensitivity and specificity of LR-TR viable or equivocal category combined were 71% (95% CI, 55–84%) and 87% (95% CI, 73–94%), respectively.
• The type of reference standard and study design were the factors significantly influencing study heterogeneity (p ≤ 0.01).


Similar content being viewed by others


Abbreviations
- AUC:
-
Area under the curve
- CI:
-
Confidence interval
- CT:
-
Computed tomography
- EASL:
-
European Association for the Study of the Liver
- HCC:
-
Hepatocellular carcinoma
- HSROC:
-
Hierarchical summary receiver operating characteristic
- LI-RADS:
-
Liver Imaging Reporting and Data System
- LRT:
-
Locoregional therapy
- LR-TR:
-
LI-RADS treatment response
- mRECIST:
-
modified Response Evaluation Criteria in Solid Tumors
- MRI:
-
Magnetic resonance imaging
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- QUADAS:
-
Quality Assessment of Diagnostic Accuracy Studies
References
Bruix J, Sherman M (2011) Management of hepatocellular carcinoma: an update. Hepatology 53:1020–1022
Heimbach JK, Kulik LM, Finn RS et al (2018) AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology 67:358–380
Cescon M, Cucchetti A, Ravaioli M, Pinna AD (2013) Hepatocellular carcinoma locoregional therapies for patients in the waiting list. Impact on transplantability and recurrence rate. J Hepatol 58:609–618
Ho MH, Yu CY, Chung KP et al (2011) Locoregional therapy-induced tumor necrosis as a predictor of recurrence after liver transplant in patients with hepatocellular carcinoma. Ann Surg Oncol 18:3632–3639
Allard MA, Sebagh M, Ruiz A et al (2015) Does pathological response after transarterial chemoembolization for hepatocellular carcinoma in cirrhotic patients with cirrhosis predict outcome after liver resection or transplantation? J Hepatol 63:83–92
American College of Radiology. Liver Imaging Reporting and Data System v2017. Available via https://www.acr.org/Clinical-Resources/Reporting-and-Data-Systems/LI-RADS/CT-MRI-LI-RADS-v2017. Accessed 12 June 2020
Lencioni R, Llovet JM (2010) Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis 30:52–60
Bruix J, Sherman M, Llovet JM et al (2001) Clinical management of hepatocellular carcinoma. Conclusions of the Barcelona-2000 EASL conference. European Association for the Study of the Liver. J Hepatol 35:421–430
Shropshire EL, Chaudhry M, Miller CM et al (2019) LI-RADS treatment response algorithm: performance and diagnostic accuracy. Radiology 292:226–234
Chaudhry M, McGinty KA, Mervak B et al (2020) The LI-RADS version 2018 MRI treatment response algorithm: evaluation of ablated hepatocellular carcinoma. Radiology 294:320–326
Cools KS, Moon AM, Burke LMB, McGinty KA, Strassle PD, Gerber DA (2020) Validation of the Liver Imaging Reporting and Data System treatment response criteria after thermal ablation for hepatocellular carcinoma. Liver Transpl 26:203–214
Kim SW, Joo I, Kim HC et al (2020) LI-RADS treatment response categorization on gadoxetic acid-enhanced MRI: diagnostic performance compared to mRECIST and added value of ancillary features. Eur Radiol 30:2861–2870
Seo N, Kim MS, Park MS et al (2020) Evaluation of treatment response in hepatocellular carcinoma in the explanted liver with Liver Imaging Reporting and Data System version 2017. Eur Radiol 30:261–271
Saleh TY, Bahig S, Shebrya N, Ahmed AY (2019) Value of dynamic and DWI MRI in evaluation of HCC viability after TACE via LI-RADS v2018 diagnostic algorithm. Egypt J Radiol Nucl Med 50:113
Liberati A, Altman DG, Tetzlaff J et al (2009) The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ 339:b2700
Whiting PF, Rutjes AW, Westwood ME et al (2011) QUADAS-2: a revised tool for the Quality Assessment of Diagnostic Accuracy Studies. Ann Intern Med 155:529–536
Kielar A, Fowler KJ, Lewis S et al (2018) Locoregional therapies for hepatocellular carcinoma and the new LI-RADS treatment response algorithm. Abdom Radiol (NY) 43:218–230
Kloeckner R, Otto G, Biesterfeld S, Oberholzer K, Dueber C, Pitton MB (2010) MDCT versus MRI assessment of tumor response after transarterial chemoembolization for the treatment of hepatocellular carcinoma. Cardiovasc Intervent Radiol 33:532–540
Shim JH, Han S, Shin YM et al (2013) Optimal measurement modality and method for evaluation of responses to transarterial chemoembolization of hepatocellular carcinoma based on enhancement criteria. J Vasc Interv Radiol 24:316–325
Cha DI, Lee MW, Kim YK et al (2014) Assessing patients with hepatocellular carcinoma meeting the Milan criteria: is liver 3 tesla MR with gadoxetic acid necessary in addition to liver CT? J Magn Reson Imaging 39:842–852
Kakihara D, Nishie A, Harada N et al (2014) Performance of gadoxetic acid-enhanced MRI for detecting hepatocellular carcinoma in recipients of living-related-liver-transplantation: comparison with dynamic multidetector row computed tomography and angiography-assisted computed tomography. J Magn Reson Imaging 40:1112–1120
Tacconelli E (2010) Systematic reviews: CRD’s guidance for undertaking reviews in health care. Lancet Infect Dis 10:226
Nohr EA, Liew Z (2018) How to investigate and adjust for selection bias in cohort studies. Acta Obstet Gynecol Scand 97:407–416
Ng J, Wu J (2012) Hepatitis B- and hepatitis C-related hepatocellular carcinomas in the United States: similarities and differences. Hepat Mon 12:e7635
Llovet JM, Bruix J (2003) Systematic review of randomized trials for unresectable hepatocellular carcinoma: chemoembolization improves survival. Hepatology 37:429–442
Funding
The authors state that this work has not received any funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Guarantor
The scientific guarantor of this publication is Joon-Il Choi.
Conflict of interest
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.
Statistics and biometry
No complex statistical methods were necessary for this paper.
Informed consent
Written informed consent was not required for this study because this study was meta-analysis.
Ethical approval
Institutional Review Board approval was not required because this study was meta-analysis.
Methodology
• Retrospective
• Meta-analysis
• Performed at one institution
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
ESM 1
(DOCX 131 kb)
Rights and permissions
About this article

Cite this article
Youn, S.Y., Kim, D.H., Choi, S.H. et al. Diagnostic performance of Liver Imaging Reporting and Data System treatment response algorithm: a systematic review and meta-analysis. Eur Radiol 31, 4785–4793 (2021). https://doi.org/10.1007/s00330-020-07464-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-020-07464-7