
Abstract
Objectives
To compare our experience with N-butyl cyanoacrylate glue as the primary embolic agent versus other embolic agents for transcatheter arterial embolization (TAE) in refractory peptic ulcer bleeding and to identify factors associated with early rebleeding and 30-day mortality.
Methods
Retrospective study of 148 consecutive patients comparing the clinical success rate in 78 patients managed with Glubran®2 N-butyl cyanoacrylate metacryloxysulfolane (NBCA-MS) alone or with other agents and 70 with other embolic agents only (coils, microspheres, ethylene-vinyl alcohol copolymer, or gelatin sponge) at a university center in 2008–2019. Univariate and multivariate logistic regression analyses were done to identify prognostic factors.
Results
The technical success rate was 95.3% and the primary clinical success was 64.5%. The early rebleeding and day-30 mortality rates were 35.4% and 21.3%, respectively. Rebleeding was significantly less common with than without Glubran®2 (OR, 0.47; 95% CI, 0.22–0.99; p = .047) and significantly more common with coils used alone (OR, 20.4; 95% CI, 10.13–50.14; p = .024). The only other factor independently associated with early rebleeding was having two or more comorbidities (OR, 20.14; 95% CI, 10.01–40.52; p = .047). Day-30 mortality was similar in the two treatment groups. A lower initial hemoglobin level was significantly associated with higher day-30 mortality (OR, 10.38; 95% CI, 10.10–10.74; p = .006). Fluoroscopy time was significantly shorter with Glubran®2 (20.8 ± 11.5 min vs. 35.5 ± 23.4 min, p = .002). Both groups (Glubran®2 vs. other agents) had similar rates of overall complications (10.7% vs. 9.1%, respectively, p = .786).
Conclusions
Glubran®2 NBCA-MS as the primary agent allowed for faster and better clinical success compared to other embolic agents when used for TAE to safely stop refractory peptic ulcer bleeding.
Key Points
• Choice of embolic agent for arterial embolization of refractory peptic ulcer bleeding is still debated. We compared our experience with N-butyl cyanoacrylate (NBCA) glue vs. other embolic agents.
• The use of Glubran®2 NBCA glue in the endovascular management of refractory peptic ulcer bleeding was significantly faster and more effective, and at least as safe compared to other embolic agents.
• NBCA glue offers several advantages compared to other embolic agents and provides rapid hemostasis when used for arterial embolization to treat refractory peptic ulcer bleeding. It should be the first-line therapy.




Similar content being viewed by others


Abbreviations
- CI:
-
Confidence interval
- CT:
-
Computed tomography
- EVOH:
-
Ethylene-vinyl alcohol
- GDA:
-
Gastroduodenal artery
- INR:
-
International normalized ratio
- LGA:
-
Left gastric artery
- LGEA:
-
Left gastroepiploic artery
- NBCA-MS:
-
N-butyl cyanoacrylate metacryloxysulfolane
- NSAID:
-
Non-steroidal anti-inflammatory drug
- PRBCs:
-
Packed red blood cells
- RGA:
-
Right gastric artery
- RGEA:
-
Right gastroepiploic artery
- SD:
-
Standard deviation
- SIR:
-
Society of Interventional Radiology
- SMA:
-
Superior mesenteric artery
- TAE:
-
Transcatheter arterial embolization
- UGIB:
-
Upper gastrointestinal bleeding
References
Gralnek IM, Dumonceau JM, Kuipers EJ et al (2015) Diagnosis and management of nonvariceal upper gastrointestinal hemorrhage: European Society of Gastrointestinal Endoscopy (ESGE) guideline. Endoscopy 47:a1–a46
Van Leerdam ME (2008) Epidemiology of acute upper gastrointestinal bleeding. Best Pract Res Clin Gastroenterol 22:209–224
Hearnshaw SA, Logan RF, Lowe D, Travis SP, Murphy MF, Palmer KR (2011) Acute upper gastrointestinal bleeding in the UK: patient characteristics, diagnoses and outcomes in the 2007 UK audit. Gut 60:1327–1335
Chiu PW, Ng EK, Cheung FK et al (2009) Predicting mortality in patients with bleeding peptic ulcers after therapeutic endoscopy. Clin Gastroenterol Hepatol 7:311–316
Lu Y, Loffroy R, Lau JY, Barkun A (2014) Multidisciplinary management strategies for acute non-variceal upper gastrointestinal bleeding. Br J Surg 101:e34–e50
Rösch J, Dotter CT, Brown MJ (1972) Selective arterial embolization. A new method for control of acute gastrointestinal bleeding. Radiology 102:303–306
Ripoll C, Bañares R, Beceiro I et al (2004) Comparison of transcatheter arterial embolization and surgery for treatment of bleeding peptic ulcer after endoscopic treatment failure. J Vasc Interv Radiol 15:447–450
Beggs AD, Dilworth MP, Powell SL, Atherton H, Griffiths EA (2014) A systematic review of transarterial embolization versus emergency surgery in treatment of major nonvariceal upper gastrointestinal bleeding. Clin Exp Gastroenterol 7:93–104
Sverdén E, Mattsson F, Lindström D, Sondén A, Lu Y, Lagergren J (2019) Transcatheter arterial embolization compared with surgery for uncontrolled peptic ulcer bleeding: a population-based cohort study. Ann Surg 269:304–309
Kyaw M, Tse Y, Ang D, Ang TL, Lau J (2014) Embolization versus surgery for peptic ulcer bleeding after failed endoscopic hemostasis: a meta-analysis. Endosc Int Open 2:E6–E14
Schenker MP, Duszak R, Soulen MC et al (2001) Upper gastrointestinal hemorrhage and transcatheter embolotherapy: clinical and technical factors impacting success and survival. J Vasc Interv Radiol 12:1263–1271
Ang D, Teo EK, Tan A et al (2012) A comparison of surgery versus transcatheter angiographic embolization in the treatment of nonvariceal upper gastrointestinal bleeding uncontrolled by endoscopy. Eur J Gastroenterol Hepatol 24:929–938
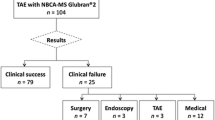
Abdulmalak G, Chevallier O, Falvo N et al (2018) Safety and efficacy of transcatheter embolization with Glubran®2 cyanoacrylate glue for acute arterial bleeding: a single-center experience with 104 patients. Abdom Radiol (NY) 43:723–733
Yonemitsu T, Kawai N, Sato M et al (2009) Evaluation of transcatheter arterial embolization with gelatin sponge particles, microcoils, and n-butyl cyanoacrylate for acute arterial bleeding in a coagulopathic condition. J Vasc Interv Radiol 20:1176–1187
Kim PH, Tsauo J, Shin JH, Yun SC (2017) Transcatheter arterial embolization of gastrointestinal bleeding with N-butyl cyanoacrylate: a systematic review and meta-analysis of safety and efficacy. J Vasc Interv Radiol 28:522–531
Filippiadis DK, Binkert C, Pellerin O, Hoffmann RT, Krajina A, Pereira PL (2017) Cirse quality assurance document and standards for classification of complications: the Cirse classification system. Cardiovasc Intervent Radiol 40:1141–1146
Stata (2017) Stata Statistical Software: Release 15. StataCorp, LLC, College Station
Mickey RM, Greenland S (1989) The impact of confounder selection criteria on effect estimation. Am J Epidemiol 129:125–137
Forrest JAH, Finlayson NDC, Schearman DJC (1974) Endoscopy of upper gastrointestinal bleeding. Lancet 2:394–397
Loffroy R, Guiu B, D’Athis P et al (2009) Arterial embolotherapy for endoscopically unmanageable acute gastroduodenal hemorrhage: predictors of early rebleeding. Clin Gastroenterol Hepatol 7:515–523
Jae HJ, Chung JW, Jung AY, Lee W, Park JH (2007) Transcatheter arterial embolization of nonvariceal upper gastrointestinal bleeding with N-butyl cyanoacrylate. Korean J Radiol 8:48–56
Spiliopoulos S, Inchingolo R, Lucatelli P et al (2018) Transcatheter arterial embolization for bleeding peptic ulcers: a multicenter study. Cardiovasc Intervent Radiol 41:1333–1339
Loffroy R, Guiu B, Cercueil JP, Krausé D (2009) Endovascular therapeutic embolisation: an overview of occluding agents and their effects on embolised tissues. Curr Vasc Pharmacol 7:250–263
Toyoda H, Nakano S, Kumada T et al (1996) Estimation of usefulness of N-butyl-2-cyanoacrylate-lipiodol mixture in transcatheter arterial embolization for urgent control of life-threatening massive bleeding from gastric or duodenal ulcer. J Gastroenterol Hepatol 11:252–258
Loffroy R, Rao P, Ota S, De Lin M, Kwak BK, Geschwind JF (2010) Embolization of acute nonvariceal upper gastrointestinal hemorrhage resistant to endoscopic treatment: results and predictors of recurrent bleeding. Cardiovasc Intervent Radiol 33:1088–1100
Ichiro I, Shushi H, Akihiko I, Yasuhiko I, Yasuyuki Y (2011) Empiric transcatheter arterial embolization for massive bleeding from duodenal ulcers: efficacy and complications. J Vasc Interv Radiol 22:911–916
Aina R, Oliva VL, Therasse E et al (2001) Arterial embolotherapy for upper gastrointestinal hemorrhage: outcome assessment. J Vasc Interv Radiol 12:195–200
Mille M, Huber J, Wlasak R et al (2015) Prophylactic transcatheter arterial embolization after successful endoscopic hemostasis in the management of bleeding duodenal ulcer. J Clin Gastroenterol 49:738–745
Pollak JS, White RI (2001) The use of cyanoacrylate adhesives in peripheral embolization. J Vasc Interv Radiol 12:907–913
Takeuchi Y, Morishita H, Sato Y et al (2014) Guidelines for the use of NBCA in vascular embolization devised by the Committee of Practice Guidelines of the Japanese Society of Interventional Radiology (CGJSIR), 2012 edition. Jpn J Radiol 32:500–517
Lang EK (1992) Transcatheter embolization in management of hemorrhage from duodenal ulcer: long-term results and complications. Radiology 182:703–707
Huang YS, Chang CC, Liou JM, Jaw FS, Liu KL (2014) Transcatheter arterial embolization with N-butyl cyanoacrylate for nonvariceal upper gastrointestinal bleeding in hemodynamically unstable patients: results and predictors of clinical outcomes. J Vasc Interv Radiol 25:1850–1857
Hur S, Jae HJ, Lee H, Lee M, Kim HC, Chung JW (2017) Superselective embolization for arterial upper gastrointestinal bleeding using N-butyl cyanoacrylate: a single-center experience in 152 patients. J Vasc Interv Radiol 28:1673–1680
Lenhart M, Paetzel C, Sackmann M et al (2010) Superselective arterial embolisation with a liquid polyvinyl alcohol copolymer in patients with acute gastrointestinal haemorrhage. Eur Radiol 20:1994–1999
Funding
The authors state that this work has not received any funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Guarantor
The scientific guarantor of this publication is Romaric Loffroy.
Conflict of interest
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Statistics and biometry
One of the authors has significant statistical expertise: Serge Aho-Gléglé, MD, Department of Epidemiology and Biostatistics, François-Mitterrand University Hospital, Dijon, France.
Informed consent
Written informed consent was not required for this study because of the retrospective nature of the study in an emergency setting.
Ethical approval
Institutional Review Board approval was not required because of the retrospective nature of the study in an emergency setting.
Methodology
• retrospective
• case-control study
• observational
• performed at one institution
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Loffroy, R., Desmyttere, AS., Mouillot, T. et al. Ten-year experience with arterial embolization for peptic ulcer bleeding: N-butyl cyanoacrylate glue versus other embolic agents. Eur Radiol 31, 3015–3026 (2021). https://doi.org/10.1007/s00330-020-07427-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-020-07427-y