
Abstract
Purpose
To investigate the outcomes of transcatheter arterial embolization (TAE) for the treatment of peptic ulcer bleeding (PUB).
Materials and Methods
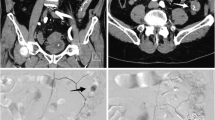
This is a retrospective, multicenter study, which investigated all patients who underwent TAE for the treatment of severe upper gastrointestinal hemorrhage from peptic ulcers in five European centers, between January 1, 2012 and May 1, 2017. All patients had undergone failed endoscopic hemostasis. Forty-four patients (male; mean age 74.0 ± 11.1 years, range 49–94), with bleeding from duodenum (36/44; 81.8%) or gastric ulcer (8/44; 18.2%) were followed up to 3.5 years (range 2–1354 days). In 42/44 cases, bleeding was confirmed by pre-procedural CT angiography. In 50% of the cases, coils were deployed, while in the remaining glue, microparticles, gel foam and combinations of the above were used. The study’s outcome measures were 30-day survival technical success (occlusion of feeding vessel and/or no extravasation at completion DSA), overall survival, bleeding relapse and complication rates.
Results
The technical success was 100%. The 30-day survival rate was 79.5% (35/44 cases). No patients died due to ongoing or recurrent hemorrhage. Re-bleeding occurred in 2/44 cases (4.5%) and was successfully managed with repeat TAE (one) or surgery (one). The rate of major complications was 4.5% (2/44; one acute pancreatitis and one partial pancreatic ischemia), successfully managed conservatively. According to Kaplan–Meier analysis survival was 71.9% at 3.5 years.
Conclusions
TAE for the treatment of PUB was technically successful in all cases and resulted in high clinical success rate. Minimal re-bleeding rates further highlight the utility of TAE as the second line treatment of choice, after failed endoscopy.


Similar content being viewed by others


References
Gralnek IM, Barkun AN, Bardou M. Management of acute bleeding from a peptic ulcer. N Engl J Med. 2008;359(9):928–37.
Lee CW, Sarosi GA Jr. Emergency ulcer surgery. Surg Clin North Am. 2011;91(5):1001–13.
Abe N, Takeuchi H, Yanagida O, Sugiyama M, Atomi Y. Surgical indications and procedures for bleeding peptic ulcer. Dig Endosc. 2010;22(Suppl 1):S35–7.
Kyaw M, Tse Y, Ang D, Ang TL, Lau J. Embolization versus surgery for peptic ulcer bleeding after failed endoscopic hemostasis: a meta-analysis. Endosc Int Open. 2014;2(1):E6–14.
Wang YR, Richter JE, Dempsey DT. Trends and outcomes of hospitalizations for peptic ulcer disease in the United States, 1993–2006. Ann Surg. 2010;251(1):51–8.
Sverdén E, Mattsson F, Lindström D, Sondén A, Lu Y, Lagergren J. Transcatheter arterial embolization compared with surgery for uncontrolled peptic ulcer bleeding: a population-based cohort study. Ann Surg. 2017. https://doi.org/10.1097/sla.0000000000002565.
Gralnek IM, Dumonceau JM, Kuipers EJ, et al. Diagnosis and management of nonvariceal upper gastrointestinal hemorrhage: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy. 2015;47(10):a1–46.
Wong TCF, Wong TT, Chiu PWY, et al. A comparison of angiographic embolization with surgery after failed endoscopic hemostasis to bleeding peptic ulcers. Gastrointest Endosc. 2011;73:900–8.
Beggs AD, Dilworth MP, Powell SL, et al. A systematic review of transarterial embolization versus emergency surgery in treatment of major nonvariceal upper gastrointestinal bleeding. Clin Exp Gastroenterol. 2014;7:93–104.
Loggers SAI, Koedam TWA, Giannakopoulos GF, Vandewalle E, Erwteman M, Zuidema WP. Definition of hemodynamic stability in blunt trauma patients: a systematic review and assessment amongst Dutch trauma team members. Eur J Trauma Emerg Surg. 2017;43(6):823–33.
Filippiadis DK, Binkert C, Pellerin O, Hoffmann RT, Krajina A, Pereira PL. Cirse quality assurance document and standards for classification of complications: the cirse classification system. Cardiovasc Interv Radiol. 2017;40(8):1141–6.
Ichiro I, Shushi H, Akihiko I, Yasuhiko I, Yasuyuki Y. Empiric transcatheter arterial embolization for massive bleeding from duodenal ulcers: efficacy and complications. J Vasc Interv Radiol. 2011;22(7):911–6.
Laffroy Lin M, Thompson C, Harsha A, Rao P. A comparison of the results of arterial embolization for bleeding and non-bleeding gastroduodenal ulcers. Acta Radiol. 2011;152(10):1076–82.
Wang YL, Cheng YS, Liu LZ, He ZH, Ding KH. Emergency transcatheter arterial embolization for patients with acute massive duodenal ulcer hemorrhage. World J Gastroenterol. 2012;18:4765–70.
Loffroy R. Management of duodenal ulcer bleeding resistant to endoscopy: surgery is dead! World J Gastroenterol. 2013;19(7):1150–1.
Loffroy R, Guiu B. Role of transcatheter arterial embolization for massive bleeding from gastroduodenal ulcers. World J Gastroenterol. 2009;15:5889–97.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed Consent
Procedural informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Spiliopoulos, S., Inchingolo, R., Lucatelli, P. et al. Transcatheter Arterial Embolization for Bleeding Peptic Ulcers: A Multicenter Study. Cardiovasc Intervent Radiol 41, 1333–1339 (2018). https://doi.org/10.1007/s00270-018-1966-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00270-018-1966-4