
Abstract
Background
Surgical debulking of primary neuroendocrine tumors (NETs) and hepatic resection of metastatic NET disease may each independently improve overall survival. However, evidence for combined primary site debulking and metastasectomy on survival and impact on short-term perioperative outcomes is limited.
Methods
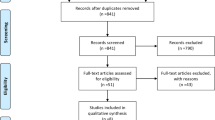
The 2014–2016 ACS-NSQIP targeted hepatectomy database was queried for all patients undergoing liver resection for metastatic NET. Secondary procedure codes were evaluated for major concurrent operations. Multivariable analysis was performed to determine risk factors for 30-day morbidity and mortality.
Results
A total of 472 patients were identified, of whom 153 (32.4%) underwent ≥1 additional concurrent major operation. The most common concurrent procedures were small bowel resection (14.6%), partial colectomy (8.9%), and radical lymphadenectomy (7.4%). Among all patients, overall 30-day mortality and morbidity were 1.5% and 25.6%, respectively. Modifiable and treatment-related factors associated with increased major postoperative morbidity risk included >10% weight loss within six months of surgery (p = 0.05), increasing number of hepatic lesions treated (p = 0.05), and biliary reconstruction (p = 0.001). No major concurrent procedure was associated with increased 30-day morbidity (all p > 0.05).
Conclusions
Approximately one-third of patients with stage IV NET underwent combined hepatic and multi-organ resection. Although modifiable and treatment-related factors predictive of perioperative morbidity were identified, performance of concurrent major procedures did not increase perioperative morbidity. These results support consideration of multi-organ resection in carefully selected patients with metastatic NET.
Similar content being viewed by others


References
Kunz PL, Reidy-Lagunes D, Anthony LB et al (2013) Consensus guidelines for the management and treatment of neuroendocrine tumors. Pancreas 42:557–577
Cisco R, Lin D, Kebebew E (2019) Aggressive resection of neuroendocrine tumor (NET) liver metastases: NET neutral or gain? Surgery 165:176–177
Rinke A, Müller HH, Schade-Brittinger C et al (2009) Placebo-controlled, double-blind, prospective, randomized study on the effect of octreotide LAR in the control of tumor growth in patients with metastatic neuroendocrine midgut tumors: a report from the PROMID Study Group. J Clin Oncol 27:4656–4663
Caplin ME, Pavel M, Ćwikła JB et al (2014) Lanreotide in metastatic enteropancreatic neuroendocrine tumors. N Engl J Med 371:224–233
Yao JC, Shah MH, Ito T et al (2011) Everolimus for advanced pancreatic neuroendocrine tumors. N Engl J Med 364:514–523
Raymond E, Dahan L, Raoul JL et al (2011) Sunitinib malate for the treatment of pancreatic neuroendocrine tumors. N Engl J Med 364:501–513
Sarmiento JM, Heywood G, Rubin J et al (2003) Surgical treatment of neuroendocrine metastases to the liver: a plea for resection to increase survival. J Am Coll Surg 197:29–37
Glazer ES, Tseng JF, Al-Refaie W et al (2010) Long-term survival after surgical management of neuroendocrine hepatic metastases. HPB 12:427–433
Graff-Baker AN, Sauer DA, Pommier SJ et al (2014) Expanded criteria for carcinoid liver debulking: maintaining survival and increasing the number of eligible patients. Surgery 156:1369–1376 (discussion 1376-1367)
Maxwell JE, Sherman SK, O’Dorisio TM et al (2016) Liver-directed surgery of neuroendocrine metastases: what is the optimal strategy? Surgery 159:320–333
Morgan RE, Pommier SJ, Pommier RF (2018) Expanded criteria for debulking of liver metastasis also apply to pancreatic neuroendocrine tumors. Surgery 163:218–225
Pavel M, Baudin E, Couvelard A et al (2012) ENETS consensus guidelines for the management of patients with liver and other distant metastases from neuroendocrine neoplasms of foregut, midgut, hindgut, and unknown primary. Neuroendocrinology 95:157–176
Pavel M, O’Toole D, Costa F et al (2016) ENETS consensus guidelines update for the management of distant metastatic disease of intestinal, pancreatic, bronchial Neuroendocrine Neoplasms (NEN) and NEN of unknown primary site. Neuroendocrinology 103:172–185
Howe JR, Cardona K, Fraker DL et al (2017) The surgical management of small bowel neuroendocrine tumors: consensus guidelines of the North American neuroendocrine tumor society. Pancreas 46:715–731
Bursac Z, Gauss CH, Williams DK et al (2008) Purposeful selection of variables in logistic regression. Source Code Biol Med 3:17
Jarnagin WR, Gonen M, Fong Y et al (2002) Improvement in perioperative outcome after hepatic resection: analysis of 1,803 consecutive cases over the past decade. Ann Surg 236:397–406 (discussion 406-397)
van den Broek MA, Olde Damink SW, Dejong CH et al (2008) Liver failure after partial hepatic resection: definition, pathophysiology, risk factors and treatment. Liver Int 28:767–780
Windsor JA, Hill GL (1988) Weight loss with physiologic impairment. A basic indicator of surgical risk. Ann Surg 207:290–296
Kneuertz PJ, Pitt HA, Bilimoria KY et al (2012) Risk of morbidity and mortality following hepato-pancreato-biliary surgery. J Gastrointest Surg 16:1727–1735
Kadaba RS, Bowers KA, Khorsandi S et al (2017) Complications of biliary-enteric anastomoses. Ann R Coll Surg Engl 99:210–215
Zafar SN, Khan MR, Raza R et al (2011) Early complications after biliary enteric anastomosis for benign diseases: a retrospective analysis. BMC Surg 11:19
Eskander MF, Bliss LA, Yousafzai OK et al (2015) A nationwide assessment of outcomes after bile duct reconstruction. HPB 17:753–762
Shah CP, Mramba LK, Bishnoi R et al (2019) Survival trends of metastatic small intestinal neuroendocrine tumor: a population-based analysis of SEER database. J Gastrointest Oncol 10:869–877
Tierney JF, Chivukula SV, Wang X et al (2019) Resection of primary tumor may prolong survival in metastatic gastroenteropancreatic neuroendocrine tumors. Surgery 165:644–651
Ye H, Xu HL, Shen Q et al (2019) Palliative resection of primary tumor in metastatic nonfunctioning pancreatic neuroendocrine tumors. J Surg Res 243:578–587
Feng T, Lv W, Yuan M et al (2019) Surgical resection of the primary tumor leads to prolonged survival in metastatic pancreatic neuroendocrine carcinoma. World J Surg Oncol 17:54
Lin C, Dai H, Hong X et al (2018) The prognostic impact of primary tumor resection in pancreatic neuroendocrine tumors with synchronous multifocal liver metastases. Pancreatology 18(5):608–614
Fairweather M, Swanson R, Wang J et al (2017) Management of neuroendocrine tumor liver metastases: long-term outcomes and prognostic factors from a large prospective database. Ann Surg Oncol 24:2319–2325
Croome KP, Burns JM, Florencia GQ et al (2016) Hepatic resection for metastatic neuroendocrine cancer in patients with bone metastases. Ann Surg Oncol 23:3693–3698
Watzka FM, Fottner C, Miederer M et al (2015) Surgical therapy of neuroendocrine neoplasm with hepatic metastasis: patient selection and prognosis. Langenbecks Arch Surg 400:349–358
Partelli S, Inama M, Rinke A et al (2015) Long-term outcomes of surgical management of pancreatic neuroendocrine tumors with synchronous liver metastases. Neuroendocrinology 102:68–76
Oncology NCPGi neuroendocrine and adrenal tumors (2019)
Mayo SC, de Jong MC, Bloomston M et al (2011) Surgery versus intra-arterial therapy for neuroendocrine liver metastasis: a multicenter international analysis. Ann Surg Oncol 18:3657–3665
Daskalakis K, Karakatsanis A, Hessman O et al (2018) Association of a prophylactic surgical approach to stage IV small intestinal neuroendocrine tumors with survival. JAMA Oncol 4:183–189
Gaujoux S, Gonen M, Tang L et al (2012) Synchronous resection of primary and liver metastases for neuroendocrine tumors. Ann Surg Oncol 19:4270–4277
Addeo P, Bertin JB, Imperiale A et al (2020) Outcomes of simultaneous resection of small bowel neuroendocrine tumors with synchronous liver metastases. World J Surg 44:2377–2368. https://doi.org/10.1007/s00268-020-05467-5
Funding
There were no internal or external sources of funding for this project.
Author information
Authors and Affiliations
Contributions
All authors have made substantial contributions to the conception and design of the work; acquisition, analysis, and interpretation of data for the work; drafting the work or providing critical revisions; and all approved of the final version to be published. All authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Conflicts of interest
The American College of Surgeons National Surgical Quality Improvement Program and the hospitals participating in the ACS-NSQIP are the source of the data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors.
Ethical approval
This study was granted exemption status after review by an independent institutional review board.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The results and opinions expressed in this article are those of the authors, and do not reflect the opinions or official policy of the United States Army or the Department of Defense.
Rights and permissions
About this article

Cite this article
Heidenreich, B.M., Kemp Bohan, P.M., Flor, R.J. et al. Examining Perioperative Risk Associated with Simultaneous Resection of Primary Neuroendocrine Tumors and Synchronous Hepatic Metastases. World J Surg 45, 531–542 (2021). https://doi.org/10.1007/s00268-020-05847-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-020-05847-x