
Abstract
Background
Distal splenorenal shunt and coronary caval shunt are commonly used for selective decompression of esophagogastric varices, but they may not solve severe hypersplenism and their application may be hampered by the presence of splenic venous thrombosis or a left gastric vein (LGV) situated deeply behind the pancreas. On the other hand, some patients have an LGV entering the splenic vein (SV). We tried to work out a new selective shunt for this group of patients.
Methods
Sixteen patients with severe hypersplenism and esophagogastric varices received coronary renal shunt using the SV following splenectomy. After splenectomy, the proximal portion of the SV and the LGV was isolated from the pancreas. The isolated SV was divided at a point 3–5 cm left to its junction with the LGV. The proximal orifice was anastomosed to the left renal vein, and the distal orifice was ligated. A clip was applied to the SV for occlusion between the portal vein and LGV. The right gastric and gastroepiploic vessels were divided to block backflow from the portal vein and to reduce the arterial inflow of the varices.
Results
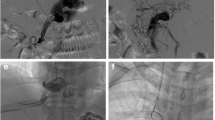
No operative mortality or procedure-related complications occurred. Postoperative computed tomography and endoscopy showed that all the shunts were patent and that the varices had been obliterated or markedly alleviated. In the 6–36 months’ follow-up period, no recurrent variceal hemorrhage or encephalopathy occurred.
Conclusion
Coronary renal shunt combined with splenectomy can achieve the goal of selective decompression of esophagogastric varices. It would become an alternative means of selective variceal decompression for patients whose LGV enters the SV.




Similar content being viewed by others


References
Pal S (2012) Current role of surgery in portal hypertension. Indian J Surg 74:55–66
Lodge JP, Mavor AI, Giles GR (1990) Does the Warren shunt correct hypersplenism? HPB Surg 2:41–49
Warren WD, Millikan WJ Jr, Henderson JM et al (1984) Selective variceal decompression after splenectomy or splenic vein thrombosis. Ann Surg 199:694–701
Inokuchi K, Beppu K, Koyanagi N et al (1984) Fifteen years’ experience with left gastric venous caval shunt for esophageal varices. World J Surg 8:716–721. https://doi.org/10.1007/BF01655768
Widrich WC, Srinivasan M, Semine MC et al (1984) Collateral pathways of the left gastric vein in portal hypertension. AJR Am J Roentgenol 142:375–382
Acknowledgements
The authors wish to acknowledge Dr. Da Zhi Chen’s valuable help in image processing and the patients’ follow-up.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Tian, M., Yang, Y. & Jia, D. Coronary Renal Shunt with Splenectomy (CRSS) for Selective Variceal Decompression. World J Surg 43, 590–593 (2019). https://doi.org/10.1007/s00268-018-4796-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-018-4796-2