
Abstract
Background
This study aimed to document thyroidectomy outcomes in the surgical endocrine unit, Mulago Hospital, Kampala, Uganda. The burden of global surgical disease is currently receiving much attention, especially in countries experiencing epidemiological transition. There is a paucity of publications on surgical outcomes from Sub-Saharan Africa. International thyroid guidelines from high-income countries do not factor in the logistical challenges or the advanced pathology faced by the surgeon in resource-limited settings.
Methods
This was a prospective cohort study in 2013. Eight peri-operative variables of poor outcome were analysed statistically against six outcomes variables. Data was collected from 0 to 6 months post-operatively.
Results
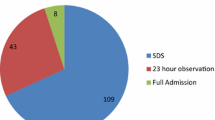
Forty-two thyroidectomies were performed over a 3-month period (female = 38). Intraoperative events recorded included rebleeding = 10 %, infection = 0 %, transient voice symptoms = 30 %, transient hypocalcaemia = 12.5 %, recurrent laryngeal nerve (RLN) paralysis = 7.5 % and permanent hypocalcaemia = 15 %. There was a weak powered association between RLN paralysis and total thyroidectomy and smaller thyroid size. There were associations between large thyroid size and both permanent hypocalcaemia and rebleeding. Younger patients showed statistically more transient voice changes compared to older patients. Older patients were statistically more likely to develop rebleeding. Shorter operative duration was associated with transient voice change, permanent hypocalcaemia and rebleeding. Airway difficulties and transient hypocalcaemia were statistically significant in prolonged procedures.
Conclusions
Whilst the thyroidectomy outcomes are not equal to international standards, an acceptable standard is achievable in this resource-limited setting. Poor outcomes are multifactorial but extremes of thyroid size, extremes of operation duration and total thyroidectomies all have statistically poorer outcomes in this setting.

Similar content being viewed by others


References
World Bank. http://data.worldbank.org/country/uganda
Andersson M et al (2005) Current global iodine status and progress over the last decade towards the elimination of iodine deficiency. Bull World Health Organ 83(7):518–525
Bimenya GS et al (2002) Monitoring the severity of iodine deficiency disorders in Uganda. Afr Health Sci 2(2):63–68
Taga I et al (2008) Youth of West-Cameroon are at high risk of developing IDD due to low dietary iodine and high dietary thiocyanate. Afr Health Sci 8(3):180–185
Kishosha PA, Galukande M, Gakwaya AM (2011) Selenium deficiency a factor in endemic goiter persistence in Sub-Saharan Africa. World J Surg 35(7):1540–1545. doi:10.1007/s00268-011-1096-5
Woodruff SL et al (2010) Global variation in the pattern of differentiated thyroid cancer. Am J Surg 200(4):462–466
Guilbert JJ (2006) The World Health Report 2006: working together for health. Educ Health (Abingdon) 19(3):385–387
Ozgediz D et al (2008) Africa’s neglected surgical workforce crisis. Lancet 371(9613):627–628
Ozgediz D et al (2008) The neglect of the global surgical workforce: experience and evidence from Uganda. World J Surg 32(6):1208–1215. doi:10.1007/s00268-008-9473-4
Grimes CE et al (2011) Systematic review of barriers to surgical care in low-income and middle-income countries. World J Surg 35(5):941–950. doi:10.1007/s00268-011-1010-1
American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer et al (2009) Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid 19(11):1167–1214. doi:10.1089/thy.2009.0110
Chandrasekhar SS et al (2013) Clinical practice guideline: improving voice outcomes after thyroid surgery. Otolaryngol 148(6 Suppl):S1–S37
British Thyroid Association (2007) Guidelines for the management of thyroid cancer. http://www.british-thyroid-association.org/news/Docs/Thyroid_cancer_guidelines_2007.pdf
Henry LR, Abad JD, Stojadinovic A (2012) The voice, not the nerve, is the functionally relevant endpoint. J Surg Oncol 106(8):1005–1006
Bergenfelz AO (2008) Complications of thyroid surgery. Scandinavian quality register for thyroid and parathyroid surgery. Langenbecks Arch Surg 393:667–673
Fualal J (2012) Characterising thyroid disease and identifying barriers to care in Uganda. World J Endocr Surg 4(2):47–53
Ogbera AO, Kuku SF (2011) Epidemiology of thyroid diseases in Africa. Indian J Endocrinol Metab 15(Suppl 2):S82–S88
Rumstadt B et al (2008) Thyroid surgery in Burkina Faso, West Africa: experience from a surgical help program. World J Surg 32(12):2627–2630. doi:10.1007/s00268-008-9775-6
Acknowledgments
The author would like to thank Professor K. Barry, Mayo General Hospital, Ireland for his help.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
O Donohoe, N., Kintu-Luwaga, R., Bolger, J. et al. A Prospective Analysis of Thyroidectomy Outcomes in a Resource-Limited Setting. World J Surg 39, 1708–1711 (2015). https://doi.org/10.1007/s00268-015-3009-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-015-3009-5