
Abstract
Background
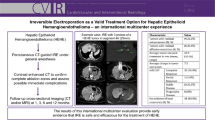
To retrospectively assess liver tumor ablation margins using intraprocedural PET/CT images from FDG PET/CT-guided microwave or cryoablation procedures and to correlate minimum margin measurements with local progression outcomes.
Methods
Fifty-six patients (ages 36 to 85, median 62; 32 females) with 77 FDG-avid liver tumors underwent 60 FDG PET/CT guided, percutaneous microwave, or cryoablation procedures. Single breath-hold PET/CT images were used for intraprocedural assessment of the tumor ablation margin: liver tumors remained visible on PET immediately following ablation; microwave ablation zones were visible using contrast-enhanced CT; cryoablation zones (ice balls) were visible using unenhanced CT. Two readers retrospectively determined ablation margin assessability and measured the minimum ablation margin on intraprocedural PET/CT (n = 77) and postprocedural MRI (n = 56). Local tumor progression was assessed on all available follow-up imaging (1–49 months, mean 15). Local tumor progression was correlated with PET/CT minimum margin measurements using clustered survival models for 61 tumors.
Results
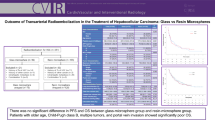
Minimum ablation margins were more often assessable using intraprocedural PET/CT (≥ 73/77 tumors, 95%) than postprocedural MRI (≤ 35/56 tumors, 63%). In 61 tumors with PET/CT-assessable margins (excluding tumors with overlapping ablations after PET/CT), there was a 6-fold increased risk of local tumor progression [hazard ratio (HR) 6.05; P = 0.004] for minimum ablation margins < 5 mm.
Conclusion
Breath-hold PET/CT scans, during PET/CT-guided microwave or cryoablation procedures for FDG-avid liver tumors, enable reliable intraprocedural assessment of the entire tumor ablation margin; a minimum PET/CT ablation margin threshold of 5 mm correlates well with local tumor progression outcomes.








Similar content being viewed by others

Data availability
The datasets generated and analyzed during the current study are not publicly available as the data are contained within our hospital electronic medical record but are available from the corresponding author on reasonable request.
References
Marrero JA, Kulik LM, Sirlin CB, et al. Diagnosis, staging, and management of hepatocellular carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology. 2018 Aug;68(2):723–50. https://doi.org/10.1002/hep.29913.
Ruers T, Van Coevorden F, Punt CJA, et al. Local treatment of unresectable colorectal liver metastases: results of a randomized phase II trial. J Natl Cancer Inst. 2017;109(9):djx015. https://doi.org/10.1093/jnci/djx015.
Meijerink MR, Puijk RS, van Tilborg AAJM, et al. Radiofrequency and microwave ablation compared to systemic chemotherapy and to partial hepatectomy in the treatment of colorectal liver metastases: a systematic review and meta-analysis. Cardiovasc Intervent Radiol. 2018;41(8):1189–204. https://doi.org/10.1007/s00270-018-1959-3.
Benson AB, Venook AP, Al-Hawary MM, Mwanzi SA, Al EN et al. NCCN Guidelines Version 1.2020 - Colon Cancer. NCCN Harmon Guidel. 1.2020. https://doi.org/10.1093/med/9780199664535.003.0012
Wang X, Sofocleous CT, Erinjeri JP, et al. Margin size is an independent predictor of local tumor progression after ablation of colon cancer liver metastases. Cardiovasc Intervent Radiol. 2013;36(1):166–75. https://doi.org/10.1007/s00270-012-0377-1.
Kim KH, Yoon YS, Yu CS, et al. Comparative analysis of radiofrequency ablation and surgical resection for colorectal liver metastases. J Korean Surg Soc. 2011;81(1):25–34. https://doi.org/10.4174/jkss.2011.81.1.25.
Sotirchos VS, Petrovic LM, Gönen M, et al. Colorectal cancer liver metastases: Biopsy of the ablation zone and margins can be used to predict oncologic outcome. Radiology. 2016;280(3):949–59. https://doi.org/10.1148/radiol.2016151005.
Ahmed M. Image-guided tumor ablation: Standardization of terminology and reporting criteria-a 10-year update. Radiology. 2014;273(1):241–60. https://doi.org/10.1148/radiol.14132958.
Kim YS, Lee WJ, Rhim H, Lim HK, Choi D, Lee JY. The minimal ablative margin of radiofrequency ablation of hepatocellular carcinoma (> 2 and < 5 cm) needed to prevent local tumor progression: 3D quantitative assessment using CT image fusion. Am J Roentgenol. 2010;195(3):758–65. https://doi.org/10.2214/AJR.09.2954.
Jiang C, Liu B, Chen S, Peng Z, Xie X, Kuang M. Safety margin after radiofrequency ablation of hepatocellular carcinoma: precise assessment with a three-dimensional reconstruction technique using CT imaging. Int J Hyperth. 2018;34(8):1135–41. https://doi.org/10.1080/02656736.2017.1411981.
Minami Y, Kudo M. Imaging modalities for assessment of treatment response to nonsurgical hepatocellular carcinoma therapy: contrast-enhanced US, CT, and MRI. Liver Cancer. 2015;4(2):106–14. https://doi.org/10.1159/000367733.
Mauri G, De Beni S, Forzoni L, et al. Virtual navigator automatic registration technology in abdominal application. In: 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBC 2014. 2014, 5570-5574 https://doi.org/10.1109/EMBC.2014.6944889
Kim KW, Lee JM, Klotz E, et al. Safety margin assessment after radiofrequency ablation of the liver using registration of preprocedure and postprocedure CT images. Am J Roentgenol. 2011 May;196(5):W565–72. https://doi.org/10.2214/AJR.10.5122.
Brace CL, Diaz TA, Hinshaw JL, Lee FT. Tissue contraction caused by radiofrequency and microwave ablation: a laboratory study in liver and lung. J Vasc Interv Radiol. 2010;21(8):1280–6. https://doi.org/10.1016/j.jvir.2010.02.038.
Sommer CM, Sommer SA, Mokry T, et al. Quantification of tissue shrinkage and dehydration caused by microwave ablation: experimental study in kidneys for the estimation of effective coagulation volume. J Vasc Interv Radiol. 2013;24(8):1241–8. https://doi.org/10.1016/j.jvir.2013.04.008.
Sainani NI, Shyn PB, Tatli S, Morrison PR, Tuncali K, Silverman SG. PET/CT-guided radiofrequency and cryoablation: is tumor fluorine-18 fluorodeoxyglucose activity dissipated by thermal ablation? J Vasc Interv Radiol. 2011;22(3):354–60. https://doi.org/10.1016/j.jvir.2010.11.027.
Shyn PB, Tremblay-Paquet S, Palmer K, et al. Breath-hold PET/CT-guided tumour ablation under general anaesthesia: accuracy of tumour image registration and projected ablation zone overlap. Clin Radiol. 2017;72(3):223–9. https://doi.org/10.1016/j.crad.2016.10.017.
Mauri G, Porazzi E, Cova L, Restelli U, Tondolo T, Bonfanti M, et al. Intraprocedural contrast-enhanced ultrasound (CEUS) in liver percutaneous radiofrequency ablation: clinical impact and health technology assessment. Insights Imaging. 2014;5(2):209–16. https://doi.org/10.1007/s13244-014-0315-7.
Shyn PB, Casadaban LC, Sainani NI, et al. Intraprocedural ablation margin assessment by using ammonia perfusion PET during FDG PET/CT–guided Liver tumor ablation: a pilot study. Radiology. 2018;288(1):138–45. https://doi.org/10.1148/radiol.2018172108.
Shyn PB, Bird JR, Koch RM, et al. Hepatic microwave ablation zone size: correlation with total energy, net energy, and manufacturer-provided chart predictions. J Vasc Interv Radiol. 2016;27(9):1389–96. https://doi.org/10.1016/j.jvir.2016.05.009.
Shyn PB. Interventional positron emission tomography/computed tomography: State-of-the-art. Tech Vasc Interv Radiol. 2013;16(3):182–90. https://doi.org/10.1053/j.tvir.2013.02.014.
Shyn PB, Mauri G, Alencar RO, Tatli S, Shah SH, Morrison PR, et al. Percutaneous image-guided cryoablation of liver tumors: predicting local progression on 24-hour MR imaging. AJR Am J Roentgenol. 2014;203(2):W181–91. https://doi.org/10.2214/AJR.13.10747.
Shady W, Petre EN, Gonen M, et al. Percutaneous radiofrequency ablation of colorectal cancer liver metastases: factors affecting outcomes-a 10-year experience at a single center. Radiology. 2016;278(2):601–11. https://doi.org/10.1148/radiol.2015142489.
Schaible J, Pregler B, Bäumler W, et al. Safety margin assessment after microwave ablation of liver tumors: inter- and intrareader variability. Radiol Oncol. 2020;54:57–61. https://doi.org/10.2478/raon-2020-0004.
Cornelis F, Storchios V, Violari E, et al. 18F-FDG PET/CT is an immediate imaging biomarker of treatment success after liver metastasis ablation. J Nucl Med. 2016;57(7):1052–7. https://doi.org/10.2967/jnumed.115.171926.
Cornelis FH, Petre EN, Vakiani E, et al. Immediate postablation 18 F-FDG injection and corresponding SUV are surrogate biomarkers of local tumor progression after thermal ablation of colorectal carcinoma liver metastases. J Nucl Med. 2018;59(9):1360–5. https://doi.org/10.2967/jnumed.117.194506.
Solomon SB, Cornelis F. Interventional molecular imaging. J Nucl Med. 2016 Apr;57(4):493–6. https://doi.org/10.2967/jnumed.115.161190.
Shyn PB, Tatli S, Sahni VA, Sadow CA, Forgione K, Mauri G, et al. PET/CT-guided percutaneous liver mass biopsies and ablations: targeting accuracy of a single 20-second breath-hold PET acquisition. Clin Radiol. 2014;69(4):410–5. https://doi.org/10.1016/j.crad.2013.11.013.
Ryan ER, Sofocleous CT, Schöder H, et al. Split-dose technique for FDG PET/CT-guided percutaneous ablation: a method to facilitate lesion targeting and to provide immediate assessment of treatment effectiveness. Radiology. 2013;268(1):288–95. https://doi.org/10.1148/radiol.13121462.
Khandani AH, Calvo BF, O’Neil BH, Jorgenson J, Mauro MA. A pilot study of early 18F-FDG PET to evaluate the effectiveness of radiofrequency ablation of liver metastases. Am J Roentgenol. 2007;189(5):1199–202. https://doi.org/10.2214/AJR.07.2126.
Yan Z, Khorasani R, Levesque VM, Gerbaudo VH, Shyn PB. Liver tumor F-18 FDG-PET before and immediately after microwave ablation enables imaging and quantification of tumor tissue contraction. Eur J Nucl Med Mol Imaging. 2020. https://doi.org/10.1007/s00259-020-05104-2.
Hu EY, Levesque VM, Bay CP, Seol JG, Shyn PB. Liver tumor ablation procedure duration and estimated patient radiation dose: comparing positron emission tomography/CT and CT guidance. J Vasc Interv Radiol. 2020;31(7):1052–9. https://doi.org/10.1016/j.jvir.2019.11.036.
Povoski SP, Sarikaya I, White WC, et al. Comprehensive evaluation of occupational radiation exposure to intraoperative and perioperative personnel from 18F-FDG radioguided surgical procedures. Eur J Nucl Med Mol Imaging. 2008;35(11):2026–34. https://doi.org/10.1007/s00259-008-0880-4.
Materials availability
The datasets generated and analyzed during the current study are not publicly available as the data are contained within our hospital electronic medical record but are available from the corresponding author on reasonable request.
Code availability
Not applicable.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Institutional Review Board (IRB) reviewed and approved the study. The study was conducted in compliance with the Health Insurance Portability and Accountability Act. The need for informed consent was waived by the IRB due to the retrospective nature of this study.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Miscellanea
Rights and permissions
About this article

Cite this article
Casadaban, L.C., Catalano, P.J., Lee, L.K. et al. Assessing ablation margins of FDG-avid liver tumors during PET/CT-guided thermal ablation procedures: a retrospective study. Eur J Nucl Med Mol Imaging 48, 2914–2924 (2021). https://doi.org/10.1007/s00259-021-05206-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-021-05206-5