
Abstract
Bone material strength index (BMSi) values are obtained using impact microindentation, which assesses the ability of bone to resist indentation. Differences in BMSi between men and women are unclear, and to date, BMSi sex differences have not been compared for individuals from the same population. Therefore, we compared BMSi values for men and women drawn from the same geographical location in Australia. Participants (n = 220) were from the Geelong Osteoporosis Study. BMSi was measured, following international published guidelines, using an OsteoProbe for participants at recent follow-up phases (women 2022–2023 and men 2016–2022). Women (n = 55) were age matched to men (n = 165) in a 1:3 ratio. A two-sample t test was used to determine the intergroup difference in mean BMSi. Linear regression was also performed, adjusting for weight and height. Median (IQR) ages for men and women were 67.0 (61.7–71.5) and 67.4 (62.0–71.2) years (p = 0.998). Men were heavier (81.0 ± 10.9 vs 71.0 ± 13.9 kg, p < 0.001) and taller (173.9 ± 6.4 vs 161.5 ± 7.5 cm, p < 0.001) than women. Mean (± SD) BMSi for women (75.7 ± 7.4) was lower than for men (82.8 ± 6.8) (p < 0.001). The difference persisted after adjustment for weight and height (mean ± SE: 76.5 ± 1.1 vs 82.5 ± 0.6, p < 0.001). Given the higher fracture risk observed for women, the higher mean BMSi values in men are consistent with cross sectional data suggesting this measure may be useful in fracture prediction.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Impact microindentation (IMI) is a relatively new technique that uses a handheld device known as the OsteoProbe [1] to assess fracture resistance of cortical bone at the mid-tibia. The device measures the indentation distance of the bone and compares it to the indentation distance of a polymethyl methacrylate reference material [2]. The ratio of these two indendation distances is then expressed as a unitless value called Bone Material Strength Index (BMSi).
Although sex differences in bone mineral density and fracture risk have been clearly reported [3,4,5], differences in BMSi between men and women are unclear. However, the recently published international healthy reference intervals suggest that there may be a difference between men and women [6]. To date, BMSi sex differences have not been compared for individuals from the same population, which is important, as differences have been reported between women from different geographical regions, namely Norway and Spain [7]. Therefore, in this study, we compared BMSi for men and women matched for age and drawn from the same geographical location in Australia.
Methods
Participants
Participants were from the Geelong Osteoporosis Study [8], a longitudinal cohort study situated in south-eastern Australia. Data for this study were derived from the most recent follow-up phases, which were 2022–2023 for women and 2016–2022 for men. This study included 55 women, who were age-matched to men (n = 165) in a 1:3 ratio, resulting in a total of 220 participants.
Impact Microindentation (IMI)
IMI measurements to determine BMSi were performed following international recommended guidelines [9] using an OsteoProbe device (Active Life Technologies, Santa Barbara, CA, USA). The same device was used for both men and women. Measurements were performed on the mid-tibia, at the midpoint from the medial border of the tibial plateau to the distal edge of the medial malleolus. Briefly, local anaesthetic was applied to the measurement area, and then the probe tip was inserted through the skin. The operator then performed the measurements by pressing down the outer housing of the device. As reported previously [10], participants experienced minimal discomfort during measurements.
The first measurement for each participant was systematically discarded. This is because the first measurement is often affected by insufficient penetration through the periosteum. Following this, at least 8 measurements were performed, and between each one, the device tip was moved approximately 2 mm. Measurements were considered invalid if they appeared outside the “green zone” area indicated by the software. Additionally, measurements were removed if the operator reported abnormal bone “texture” while performing the measurements.
During the relevant follow-up phases of the Geelong Osteoporosis Study, there were four trained operators performing IMI measurements. However, almost three quarters of the measurements (73.6%) were performed by one operator (PR-M). The coefficient of variation (CV) for microindentation was 2% for repeated measures. Precision was calculated as the mean (expressed as %) of SD/mean for two sets of indentations for 10 participants.
Other Data
Weight and height were measured to the nearest 0.1 kg and 0.1 cm, using electronic scales and a Harpenden stadiometer, respectively. Body mass index (BMI) was calculated as weight(kg)/height(m)2. Participants self-reported their use of anti-fracture medication (e.g. bisphosphonates, other antiresorptives).
Statistical Analyses
Participant characteristics were described using means and standard deviations (SD) or medians with interquartile range (IQR) as appropriate. A two-sample t test was used to determine unadjusted differences in mean BMSi between men and women. Additionally, linear regression analyses adjusting for weight and height were performed. A sensitivity analysis was also performed excluding those taking anti-fracture medications. Analyses were completed using Minitab (Minitab, version 19, State College, PA, USA) and Stata (Version 17. StataCorp. 2017. Stata Statistical Software: Release 17. College Station, TX: StataCorp LLC).
Results
Descriptive Characteristics
Table 1 shows the participant characteristics. Men were heavier and taller than women. Despite this, BMI was similar for men and women.
Differences in Bone Material Strength Index
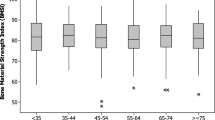
The mean (± SD) BMSi for women was lower than for men (Table 1, Fig. 1, p < 0.001). After adjustment for weight and height, this association persisted. For women, adjusted mean BMSi was lower than that for men (mean ± SE: 76.5 ± 1.1 vs 82.5 ± 0.6, p < 0.001).

Bone material strength index values for men and women
In the sensitivity analysis, there were eight participants (5 women, 3 men) taking an anti-fracture medication. Exclusion of these participants did not change the results; women had lower BMSi in unadjusted (mean ± SD: 75.4 ± 7.3 vs 82.8 ± 6.9, p < 0.001) and adjusted (mean ± SE: 76.1 ± 1.2 vs 82.6 ± 0.6, p < 0.001) analyses.
Discussion
This study indicated that mean BMSi was higher for men compared to women drawn from the same population, independent of differences in weight and height.
These results are in agreement with a recently published study describing reference intervals for men and women from multiple international sites [6]. The study reported BMSi values of 84.4 ± 6.9 for men and 79.0 ± 9.1 for women (p < 0.001). These values are similar to that reported in our study, however, our study included age-matched individuals drawn from the same underlying population. This is important, as some differences have been reported between different geographical areas [7].
Many other previous studies including IMI measurements have included only one sex, usually women. However, a few have included both men and women. One study measured 50 individuals with human immunodeficiency virus (HIV) and 35 healthy volunteers [11]. Among individuals with HIV, men had a higher BMSi than women (median (IQR): 85 (83–87) vs 80 (77–83); p < 0.001). However, among the control group, no differences between men and women were observed (median (IQR): 92 (88–96) vs 89 (86–93), p = 0.07). The reason for differences between our study and this previous study could include that the control group were volunteers, whereas the participants in our study were unselected and derived from the general population. Additionally, the median age for individuals in our study was higher (approximately 67 years vs 36 years) and thus our study may have captured greater bone loss and microarchitectural deterioration that occurs at menopause in women. In another study that included 37 individuals with primary hyperparathyroidism [12], there was no difference in mean BMSi between men and women (79.6 ± 4.4 vs 77.7 ± 6.1, p = 0.404). However, when compared to controls (n = 37), those with primary hyperparathyroidism had lower mean BMSi (78.2 ± 5.7 vs 82.8 ± 4.5, p < 0.001). Again this is different to what was reported in our study, however, the sample size for the study was small (9 men, 28 women) and consequently there may not have been sufficient power to observe any differences. Additionally, no differences were observed between men and women with primary hyperparathyroidism, but the presence of the disease may have resulted in lower BMSi, regardless of sex.
There are also several studies that have included men and women who had sustained a fracture. Two of these studies included participants with fragility fracture compared to individuals without fracture, and both studies reported no differences between men and women [13, 14]. The third study compared participants with high and low trauma fractures, also reporting no differences between men and women [15]. Similar to the study including individuals with primary hyperparathyroidism, it is possible that fracture status has a larger impact on BMSi value than sex. However, the sample sizes in some of these studies were small and thus, larger studies would be needed to confirm this possibility.
Only one previous study has examined associations between risk of incident fracture and BMSi [16]. The study included 647 women aged 75 to 80 years, and reported that, unexpectedly, higher BMSi was associated with an increased risk of fracture. Further studies are needed to replicate this observation, as well as investigate whether there are sex differences in the association between BMSi and incident fracture.
Our study has some strengths and limitations. One major strength is that the men and women were from the same population, age-matched, and not selected on the basis of disease. Additionally the OsteoProbe operators and device were the same for both groups. The sample size was sufficient, and a power analysis showed the study had > 90% power to observe differences in BMSi between men and women. One limitation is that we are unable to provide any longitudinal data, to determine if the differences observed in BMSi between men and women also translate to a difference in fracture risk.
Conclusion
These data support previous work that showed differences in BMSi between men and women, using pooled data from different geographical settings. This also contributes to baseline data for investigating the ability of BMSi to predict sex-specific fracture risk. Given the higher fracture risk observed among women, the higher mean BMSi values in men is consistent with cross sectional data and may explain, in part, why fracture risk is lower in men than women.
References
Bridges D, Randall C, Hansma PK (2012) A new device for performing reference point indentation without a reference probe. Rev Sci Instrum 83:44301
Randall C, Bridges D, Guerri R et al (2013) Applications of a new handheld reference point indentation instrument measuring bone material strength. J Med Device 7:41005
Kaufman J-M (2021) Management of osteoporosis in older men. Aging Clin Exp Res 33:1439–1452. https://doi.org/10.1007/s40520-021-01845-8
Sutton RAL, Dian L, Guy P (2011) Osteoporosis in men: an underrecognized and undertreated problem. B C Med J 53:535–540
International Osteoporosis Foundation (2022) International Osteoporosis Foundation | Bone Health. https://www.osteoporosis.foundation/health-professionals/fragility-fractures/epidemiology
Rufus-Membere P, Holloway-Kew KL, Diez-Perez A et al (2023) Reference intervals for bone impact microindentation in healthy adults: a multi-centre international study. Calcif Tissue Int 112:338–349. https://doi.org/10.1007/s00223-022-01047-y
Duarte Sosa D, Vilaplana L, Guerri R et al (2015) Are the high hip fracture rates among Norwegian women explained by impaired bone material properties? J Bone Miner Res 30:1784–1789. https://doi.org/10.1002/jbmr.2537
Pasco JA, Nicholson GC, Kotowicz MA (2012) Cohort profile: Geelong osteoporosis study. Int J Epidemiol 41:1565–1575
Diez-Perez A, Bouxsein ML, Eriksen EF et al (2016) Technical note: Recommendations for a standard procedure to assess cortical bone at the tissue-level in vivo using impact microindentation. Bone Rep 5:181–185. https://doi.org/10.1016/j.bonr.2016.07.004
Rufus-Membere PG, Holloway-Kew KL, Diez-Perez A et al (2018) Feasibility and tolerability of bone impact microindentation testing: a cross-sectional, population-based study in Australia. BMJ Open 8:e023959. https://doi.org/10.1136/bmjopen-2018-023959
Guerri-Fernandez R, Molina D, Villar-Garcia J et al (2016) Brief report: HIV infection is associated with worse bone material properties, independently of bone mineral density. J Acquir Immune Defic Syndr 72:314–318. https://doi.org/10.1097/qai.0000000000000965
Schoeb M, Winter EM, Sleddering MA et al (2021) Bone material strength index as measured by impact microindentation is low in patients with primary hyperparathyroidism. J Clin Endocrinol Metab 106:e2527–e2534. https://doi.org/10.1210/clinem/dgab207
Malgo F, Hamdy NAT, Papapoulos SE, Appelman-Dijkstra NM (2017) Bone material strength index as measured by impact microindentation is low in patients with fractures irrespective of fracture site. Osteoporos Int 28:2433–2437. https://doi.org/10.1007/s00198-017-4054-8
Malgo F, Hamdy NA, Papapoulos SE, Appelman-Dijkstra NM (2015) Bone material strength as measured by microindentation in vivo is decreased in patients with fragility fractures independently of bone mineral density. J Clin Endocrinol Metab 100:2039–2045. https://doi.org/10.1210/jc.2014-4346
Schoeb M, Winter EM, Malgo F et al (2022) Bone material strength index as measured by in vivo impact microindentation is normal in subjects with high-energy trauma fractures. Osteoporos Int 33:1511–1519. https://doi.org/10.1007/s00198-022-06368-0
Jaiswal R, Zoulakis M, Axelsson KF et al (2023) Increased bone material strength index is positively associated with the risk of incident osteoporotic fractures in older Swedish women. J Bone Miner Res 38:860–868. https://doi.org/10.1002/jbmr.4816
Acknowledgements
This study was funded by Amgen Inc. and the National Health and Medical Research Council (Australia). KLH-K is supported by an Alfred Deakin Postdoctoral Research Fellowship; PR-M by a Deakin University Postgraduate Industry Research Scholarship; KBA by an Australian Government Research Training Program Scholarship; JWH was supported by a Deakin University Postgraduate Research Scholarship.
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions. This study was funded by Amgen Inc., National Health and Medical Research Council, Alfred Deakin Postdoctoral Research Fellowship, Deakin University Postgraduate Industry Research Scholarship, Australian Government Research Training Program Scholarship, Deakin University Postgraduate Research Scholarship.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
AD-P owns shares of Active Life Scientific, Inc., the manufacturer of the reference point indentation device. KLH-K, PR-M, KBA, JWH, MAK, and JAP have no competing interests to declare.
Ethical Approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Barwon Health Human Research Ethics Committee (projects 92/01 and 00/56). Each participant provided informed consent to participate in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Holloway-Kew, K.L., Rufus-Membere, P.G., Anderson, K.B. et al. Mean Bone Material Strength Index Values for Women are Lower Than Those for Men: Data from a Single Geographical Location. Calcif Tissue Int 113, 511–514 (2023). https://doi.org/10.1007/s00223-023-01133-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00223-023-01133-9